

Abstract
Background/Goal
We sought to evaluate published evidence in aggregate regarding the impact of parenting style on the cognitive and behavioral outcomes of former preterm infants.
Methods
We searched five databases using germane MeSH terms. We defined parenting style as any descriptor of parenting using ≥2 dimensions on published parenting axes. We evaluated studies for quality of evidence and strength of recommendations using standardized tools and categorized summative recommendations by parenting axis and child outcome.
Results
Twenty-seven articles met our inclusion criteria. Parental responsivity is the only parenting axis strongly associated with both improved child cognition and behavior. Parental demandingness is associated only with improved child cognition, and parental warmth and rejection are associated only with child behavior. Parental coercion is not associated with subsequent child outcomes.
Conclusions
Parental responsivity may be essential to optimizing neurodevelopment in former preterm infants. More targeted studies are needed to inform this relationship and identify opportunities for intervention.
Keywords: parent, preterm, development
Introduction
Each year in the United States, approximately one in ten infants is born preterm before 37 weeks gestation (Martin, Hamilton, & Osterman, 2017). Of these preterm infants, 28% are born at less than 34 weeks gestation. Preterm-born children have higher rates of neurodevelopmental problems compared to term born infants. The earliest and smallest of these infants are most at risk for developmental delays (Aarnoudse-Moens, Weisglas-Kuperus, van Goudoever, & Oosterlaan, 2009; Bhutta, Cleves, Casey, Cradock, & Anand, 2002). The cognitive performance of school-aged children born preterm is directly proportional to their birthweight and gestational age (Bhutta, Cleves, Casey, Cradock, & Anand, 2002). Similarly, smaller and earlier-born preterm infants display more alterations in neurobehavior, including attention difficulties and increased internalizing and externalizing tendencies (Aarnoudse-Moens, Weisglas-Kuperus, van Goudoever, & Oosterlaan, 2009). More recent studies show that even infants born late preterm (34 to 37 weeks gestation), have increased rates of mental or physical developmental delay compared to their term counterparts (Woythaler, McCormick, & Smith, 2011; Petrini et al., 2009). These late preterm infants are more likely than term-born infants to require special education services at early school age (Chyi, Lee, Hintz, Gould, & Sutcliffe, 2008) and to manifest attention or internalizing behavioral problems (Talge et al., 2010). The worst outcomes of preterm born infants have multiple etiologies, from acute illness to interruption of the normal sequence of brain development. Parental factors also influence neurodevelopmental outcomes of preterm infants (Dilworth-Bart, Miller, & Hane, 2012; Hebert, 2002; Shah, Robbins, Coelho, & Poehlmann, 2013; Treyvaud et al., 2016).
Parenting is a critical social factor in child development that encompasses many psychological concepts, cultural norms, and practical considerations (Shah, Robbins, Coelho, & Poehlmann, 2013; Treyvaud et al., 2016). Parenting style is a multidimensional construct with at least eight major axes defined in the psychological literature and is relatively stable for an individual child in the absence of intervention (Baumrind, 1966; Brooks-Gunn, McCarton, & McCormick, 1998; Hall et al., 2015; Maupin & Fine, 2014; Melnyk et al., 2006; Skinner, Johnson, & Snyder, 2005). These axes include parental warmth, rejection, structure, chaos, autonomy support, coercion, demandingness, and responsivity (Baumrind, 1966; Skinner, Johnson, & Snyder, 2005). Parental warmth indicates a positive regard and nurturance of the parent towards the child, whereas rejection describes an experience of parental frustration and disapproval. Structure characterizes parental consistency in interactions with the child whereas chaos describes an erratic or unpredictable parental response. Autonomy support characterizes a style that allows the child opportunities to freely express him/herself, while coercion suggests parental restrictiveness and autocracy (Skinner, Johnson, & Snyder, 2005). In small children, parental demandingness characterizes the level of a parent’s expectations of the child and whether or not these expectations are developmentally commensurate to the child’s ability (Barrera, Rosenbaum, & Cunningham, 1986a; Barrera, Cunningham, & Rosenbaum, 1986b; Baumrind, 2005; Feldman, Eidelman, Sirota, & Weller, 2002; Herd, Whittingham, Sanders, Colditz, & Boyd, 2014; Melnyk et al., 2001; Smith, Brooks-Gunn, Kohen, & McCarton, 2001). Parental responsivity is often synonymous with parental sensitivity, and characterizes how well the parent reads a child’s verbal and non-verbal cues (Barrera, Rosenbaum, & Cunningham, 1986a; Barrera, Cunningham, & Rosenbaum, 1986b; Baumrind, 1966; Baumrind, 2005; Johnson et al., 2009; Maupin & Fine, 2014; Smith, Brooks-Gunn, Kohen, & McCarton, 2001; Smith, Landry, & Swank, 2006; Treyvaud et al., 2009; Treyvaud et al., 2016; Vinall, Miller, Synnes, & Grunau, 2013). While authors may use different words to describe these axes, these eight major style domains are consistent across published literature.
Studies of preterm infants have examined the impact of a single parenting axis (such as responsivity) on specific child outcomes, for example language or behavior (Treyvaud et al., 2009; Vinall, Miller, Synnes, & Grunau, 2013). No studies to date have examined associations between multiple axes of parenting style and neurodevelopmental outcomes. First, every single dimension of parenting is rarely represented in a study’s choice of parenting style definition. Secondly, sufficient power for an accurate assessment of a complex aggregate of behaviors in a prospective longitudinal cohort would require an impractically large sample size. Despite lack of feasibility, a study of the entirety of parenting style (rather than separate components) would be critical to further our understanding of how parenting influences developmental outcomes of former preterm infants. In particular, better characterization of the interactions between all the components of parenting style and the neurodevelopment of former preterm infants would allow opportunities for informed design of interventions promoting optimal outcomes. Heretofore, interventions centered on parenting characteristics to improve the neurodevelopment of preterm infants are highly variable in content, structure, intensity, and duration and focus (Bagner, Sheinkopf, Vohr, & Lester, 2010; Barrera, Rosenbaum, & Cunningham, 1986a; Barrera, Cunningham, & Rosenbaum, 1986b; Berlin, Brooks-Gunn, McCarton, & McCormick, 1998; Blair, Peters, & Lawrence 2003; Feldman, Eidelman, Sirota, & Weller, 2002; Herd, Whittingham, Sanders, Colditz, & Boyd, 2014; Johnson et al., 2009; Melnyk et al., 2001; Schappin et al., 2013).
Therefore, we aimed to address this gap in knowledge by leveraging rigorous systematic review tools to examine how intersecting components of parenting style may impact neurodevelopment of former preterm infants. We hypothesized that utilizing a systematic PRISMA approach to data collection and standardized analysis tools, we could determine which intersecting axes of parenting style are most strongly associated with optimal neurodevelopmental outcomes in former preterm infants. Ultimately, our goal is to inform healthcare professionals and policymakers in the future design of parenting interventions.
Methods
Search strategy
Inclusion Criteria
We included articles that contained at least two measured dimensions of behaviors on published parenting style axes (see Figure 1 and supplemental Table 1), used standardized child behavioral and cognitive outcomes and examined at least one former preterm infant at less than two years corrected age (Achenbach & Rescorla, 2000; Albers & Grieve, 2007; Carter & Briggs-Gowan, 2000; Carter, Briggs-Gowan, Jones, & Little, 2000; Dunn & Dunn, 1981; Eyberg & Pincus, 1999; Goodman, 1997; Hedrick, Prather, & Tobin, 1984; Roid, 2003; Semel, Wiig, & Secord, 2003; Wechsler, 1999). Assessment and intervention studies were allowed, as well as dissertations and other forms of grey literature.
Figure 1.
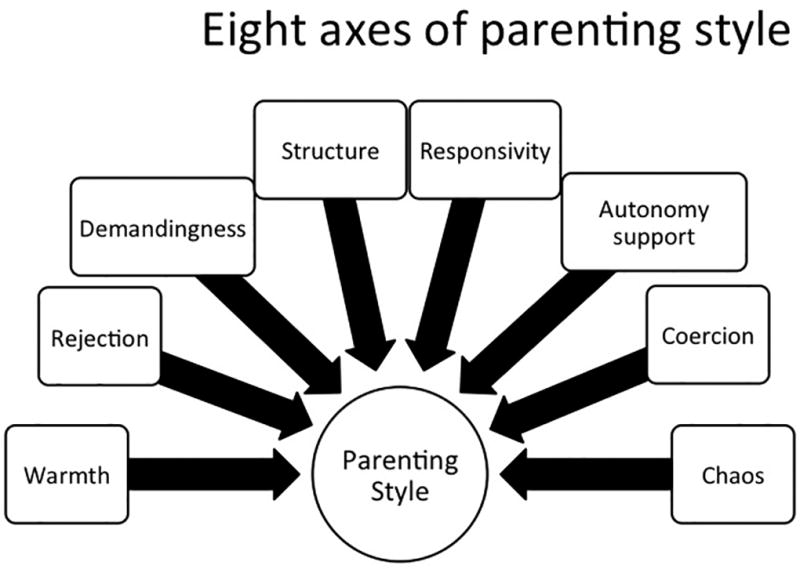
Figure 1 legend:
This figure depicts the eight axes seen in the literature that comprise parenting style (Baumrind 1967, Maccoby & Martin 1983, Skinner et al 2005).
Given our specific interest in parenting style, we included any assessment performed using tests with good psychometric properties for multiple aspects of cognition and behavior. If specific outcomes were further separated, not enough studies would remain in any one category to study a body of evidence on parenting style. We stipulated that the first assessment must have occurred at less than two years corrected age to ensure some standardization regarding follow up. Although the results reflect aggregate age data, we included only assessments at less than or equal to seven years of age. We kept the age range somewhat broad in order to enable us to study a body of evidence on parenting style in former preterm infants.
Exclusion Criteria
We excluded articles not written in English as well as letters, editorials, lectures, books, or notes.
The following databases were searched for relevant terms: Pubmed, PsycINFO, Google scholar, Embase, and Cumulative Index to Nursing and Allied Health Literature (CINAHL). Searches were run in July and August of 2016. Search terms included combinations of parenting, outcome, premature and infant as described below (or supplemental data).
Databases and search terms
Pubmed – ("Parenting" [Mesh] AND "Outcome Assessment (Health Care)" [Mesh]) OR ("Parenting/psychology" [Mesh] AND "Outcome Assessment (Health Care)" [Mesh] AND "Infant, Premature" [Mesh]) OR ("Parenting" [Mesh] AND "Outcome Assessment (Health Care)" [Mesh] AND "Intensive Care, Neonatal" [Mesh]) OR ("Parenting" [Mesh] AND "Outcome Assessment (Health Care)" [Mesh] AND "Critical Care" [Mesh]) OR ("Growth and Development"[Mesh] OR development[tiab] OR neurodevelopment[tiab]) AND ("Infant, Premature"[Mesh] OR premature infants[tiab] OR preterm infants[tiab]) AND ("Parenting" [Mesh] OR parenting[tiab] OR parenting styles[tiab]) AND ("infant"[MeSH Terms] OR "child, preschool"[MeSH Terms])
PsychINFO – ([parenting styles] AND [development OR outcomes] AND [infant premature OR preterm infants]) OR ([Growth and Development OR development OR neurodevelopment] AND [premature infant OR premature infants OR preterm infants OR preterm infants] AND [Parenting OR parenting OR parenting styles])
Google Scholar – (allintitle: parent AND preterm OR premature) OR (allintitle: parenting AND preterm OR premature) OR (allintitle: parenting AND outcomes OR development OR preterm OR premature) OR (allintitle: parenting AND preterm OR premature AND outcomes OR development)
Embase – ([Growth and Development OR development OR neurodevelopment] AND [premature infant OR premature infants OR preterm infants OR preterm infants] AND [Parenting OR parenting OR parenting styles])
CINAHL – ([Growth and Development OR development OR neurodevelopment] AND [premature infant OR premature infants OR preterm infants OR preterm infants] AND [Parenting OR parenting OR parenting styles])
We used the RTI Item Bank to evaluate the risk of bias for assessment or observational studies, AMSTAR methodological quality rating checklist for systematic reviews, and Cochrane Risk of Bias for randomized controlled trials to evaluate the quality of evidence for included studies (Higgins et al., 2011; Shea et al., 2009; Viswanathan & Berkman, 2012). Grading of Recommendations Assessment, Development and Evaluation (GRADE) guidelines informed the strength of recommendations for the compilation of articles included in this review (Dijkers, 2013). GRADE guidelines were created by the GRADE working group and have been widely adopted (Dijkers, 2013). Reliability testing has been performed on all scales utilized in this review (Hartling et al., 2013; Shea et al., 2009; Viswanathan & Berkman, 2012). See supplemental Tables 1 and 2 for quality of evidence details.
Types of participants
For inclusion in the review, the study cohorts contained at least one preterm infant with at least one assessment performed below two years of age. Specific age and weight criteria and follow up period for included studies are in listed in supplemental Table 1.
Data review and quality/recommendations identification
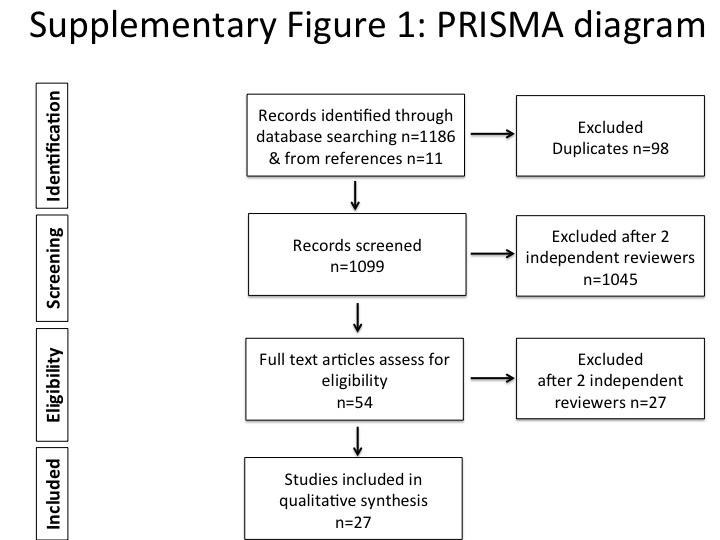
Two independent reviewers (authors 1 & 3) examined titles and abstracts generated by the initial search, assessed them for inclusion, and selected abstracts for inclusion. In the event of disagreement, the two reviewers reviewed all inclusion and exclusion criteria until agreement was reached. The reviewers then assessed the full text articles using a PRISMA data extraction format (see supplemental Figure 1). Reviewers determined quality of evidence with RTI Item Bank, AMSTAR, and Cochrane Risk of Bias tools, and determined recommendations using GRADE guidelines.
Results
Initial searches yielded 1186 results plus an additional 11 from reference materials. Each individual study in the single eligible systematic review was examined for possible individual inclusion in our review (Herd, Whittingham, Sanders, Colditz, & Boyd, 2014). Many of the studies had already been captured in our initial literature search. Duplicates, presentations, and book chapters were removed. Twenty-seven articles met criteria for inclusion in our systematic review. Supplemental Figure 3 highlights the PRISMA process of study selection.
Study characteristics
In the studies evaluated, children were assessed at ages that ranged from 0–18 years, although all examined at least some child outcomes at less than two years per our inclusion criteria. We also limited the included data from these studies to assessments of children less than or at seven years of age. The majority of studies contained only preterm infants in their cohorts (n=17). Most studies (n = 9) that included a full-term control group either analyzed preterm and full term groups separately or accounted for prematurity in the modeling strategies. We only included the analyses of the preterm groups in mixed studies, or of entire cohorts when the analysis accounted for prematurity in statistical modeling, to ensure that results were true for the preterm group specifically. The only study (n=1) that did not separate preterm from full term results had low quality of evidence for the purpose of this review (Schappin et al., 2013). This study included both preterm and full term infants with neonatal encephalopathy, although 88% of the cohort was preterm (Schappin et al., 2013).
One-third of the studies examined interventions to change parenting style (n=10) and the other two-thirds (n=17) assessed parenting style characteristics with respect to outcomes. All studies examined subsequent child neurodevelopmental outcomes. Studies included 8 randomized controlled trials (RCT), one systematic review, and 18 cohort studies. The number of participants ranged from 28 to 12,302 (median=188, excluding systematic review). Ten studies included a full-term group in addition to a preterm group.
The quality of evidence of the studies ranged from very low to high with 9 very low, 9 low, 7 moderate, and 2 high quality evidence studies (see supplemental Tables 1 and 2). The quality of evidence was skewed towards lower quality.
We classified the content of the included studies by parenting style axis and the neurodevelopmental outcome that was assessed in order to group and make GRADE recommendations most effectively. The majority of studies examined either child cognitive or behavioral outcomes, so data were sufficient to make a recommendation on these child outcomes. For the intervention studies that we included, the main factors that weakened the quality of evidence were imprecision, indirectness, or poorly measured parenting axes. For the assessment studies, the main factors that weakened the quality of evidence were generalizability issues, blending of preterm and full term data, imprecise axes, and nature of the grey literature (specifically, the one unpublished dissertation included).
Discussion
We based recommendations upon the number of studies and sample sizes, the quality of evidence, and the strength of associations within the studies. Strong recommendations indicate a preponderance of evidence that an association between the parenting axis and the child outcome does or does not exist. This evidence is derived from the agreement between studies, the number of studies, and the quality of evidence of the studies that inform that specific recommendation. Conditional recommendations are weaker than strong recommendations; they indicate either agreement among few studies or mixed evidence among the higher quality or greater number of studies. We made no recommendations when the results were completely mixed or when there was a paucity of studies.
Recommendations for cognitive outcomes (Figure 2a) and behavioral outcomes (Figure 2b) are displayed in a style adapted from Novak et al (2013) (Novak et al., 2013). The only strong positive association for cognitive outcomes was with parental responsivity, while conditional positive associations included parental demandingness, structure, and autonomy support. This review conditionally supported that no association can be demonstrated between coercion and cognitive outcomes. For behavioral outcomes, the strong positive associations were parental warmth and responsivity. Rejection demonstrated a strong negative association. Structure was a conditional positive recommendation. The evidence indicated that both parental autonomy support (strongly) and coercion (strongly) were not associated with child behavioral outcomes in former preterm infants.
Figure 2.
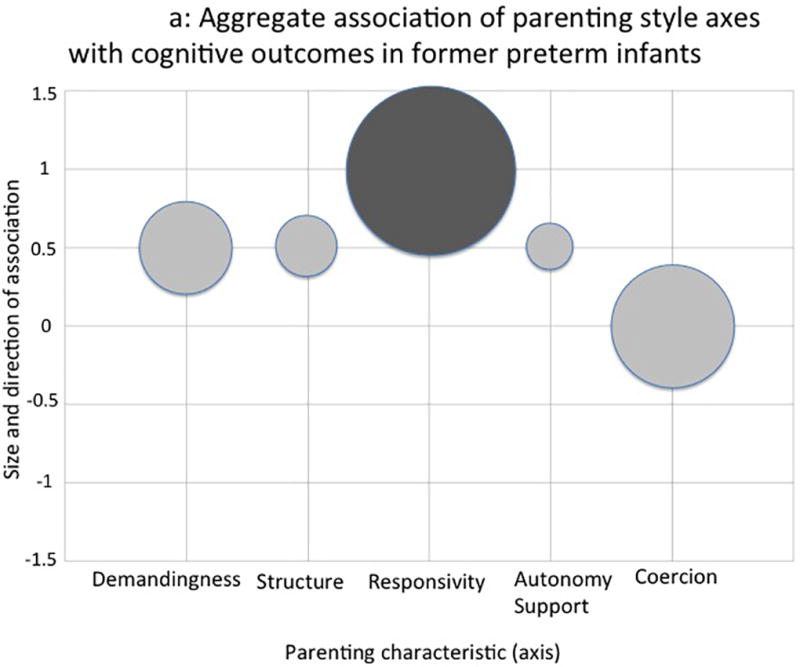
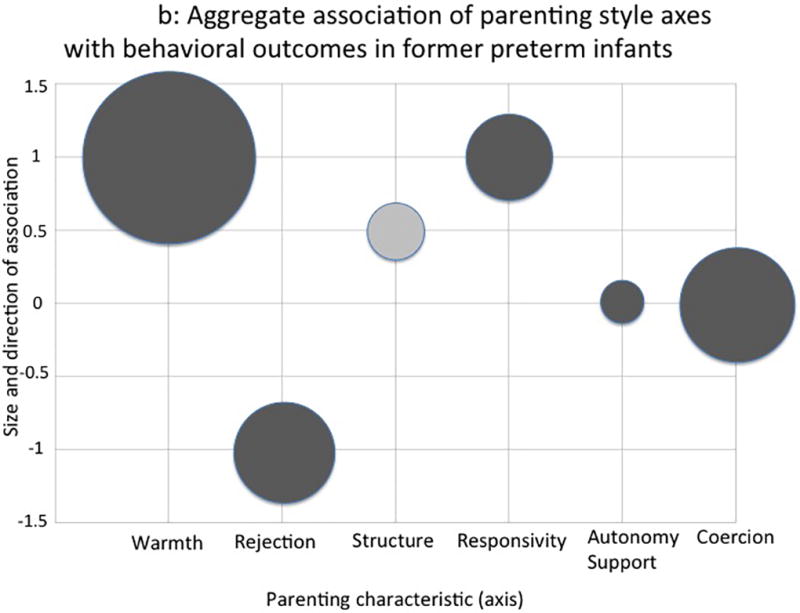
Figure 2a & 2b legend:
This figure represents the quantity and quality of the evidence relating parenting axes with either child cognitive (2a) or behavioral (2b) outcomes. Parenting style axes are defined as follows:
Warmth – positive affect and acceptance of child
Rejection – hostility or criticism towards child
Demandingness – degree of developmentally appropriate expectations
Structure – assertive control and consistency
Responsivity – sensitivity to child’s cues
Autonomy support – nondirective support and respect for child’s independence
Coercion – intrusiveness or over controlling
>0 (+ direction) indicates a positive association, 0 no association, and <0 (− direction) a negative association between the parenting axis and child outcome. The size of the circle represents the number of studies. The color of the circle indicates the strength of recommendation, with dark gray indicating strong recommendations in positive and negative directions, respectively. Light gray indicates a conditional recommendation. Axes for which recommendations could not be made were excluded from these figures.
Significance
This is the first systematic review to examine aggregate data in published literature regarding the impact of specific parenting style axes on specific child neurodevelopmental outcomes in former preterm infants. Among the publications reviewed, cognitive and behavioral child outcomes were the most commonly studied. The strategy of comparing these individual parenting qualities to child cognitive and behavioral outcomes allowed for a clearer look at which axes of parenting are most strongly associated with certain developmental outcomes in former preterm infants.
We showed that parental responsivity was the only axis strongly associated with both improved child cognitive and behavioral outcomes. Specific axes, such as parental demandingness, are associated with improved child cognition but not improved behavior. Other axes, such as parental warmth and rejection, are strongly associated with child behavioral outcomes, but not cognitive outcomes. Some parenting style axes were strongly not associated with child outcomes. For example, parental autonomy support was not associated with child behavioral outcomes, although it was associated with improved child cognitive outcomes. Parental coercion also was not associated with better or worse subsequent child cognition or behavior. No studies examined parental chaos.
Associations between parental warmth or rejection and subsequent child cognition were difficult to assess as evidence from studies was evenly split between studies that did or did not demonstrate associations. Although parental warmth is strongly associated with improved child behavioral outcomes and parental rejection is strongly associated with worse behavioral outcomes, we were unable to make recommendations regarding the relationships or lack thereof of between parental warmth or rejection and later child cognition in former preterm infants. In addition, because of the paucity of studies and low quality of evidence examining parental demandingness and child behavioral outcomes, we were unable to assess this association.
Included studies used varying methodology to describe and measure parental warmth. In most cases, warmth was coded during an observed parent-child interaction using a standardized coding tool (Poehlmann et al., 2012; Schappin et al., 2013; Smith, Landry, & Swank, 2006; Treyvaud et al., 2009). Warmth scales include positive affect, coded using positive expressions by a parent towards a child (e.g. smiling, clapping hands, praise) (Treyvaud et al., 2009). Warmth scales also include parental behaviors indicating concern or acceptance and/or supportive presence, positive regard, and emotional support towards the child (Schappin et al., 2013; Smith, Landry, & Swank, 2000). Warmth indicates a lack of observable frustration, hostility and criticism (Poehlmann et al., 2012; Vinall, Miller, Synnes, & Grunau, 2013). Increased parental warmth is associated with positive behavioral outcomes in former preterm infants as indicated by fewer internalizing and externalizing problems measured using standardized assessments such as the CBCL (Blair, Peters, & Lawrence 2003; Poehlmann et al., 2011; Shah, Robbins, Coelho, & Poehlmann, 2013; Vinall, Miller, Synnes, & Grunau, 2013). These childhood problems are precursors of later mental health problems, such as anxiety and depression in later life (Hofstra, Van Der Ende, & Verhulst, 2002).
Parental rejection is measured using the same parent-child observations as parental warmth. Rejection scores during interactions assess parental anger, hostility, criticism, disapproval, and frustration towards the child (Blair, Peters, & Lawrence 2003; Poehlmann et al., 2011; Poehlmann et al., 2012; Treyvaud et al., 2009). Parental rejection is associated with increased internalizing and externalizing behaviors in former preterm infants (Poehlmann et al., 2011; Poehlmann et al., 2012; Treyvaud et al., 2009). Given that parental rejection is described in these studies as the antithesis of parental warmth, it is intuitive that child behavioral outcomes after parental rejection are poor.
Parental demandingness describes the extent to which parents have developmentally appropriate expectations of the child: expectations are neither too high nor too low for the child’s age and stage. Demandingness is measured by coded parent-child interaction sessions and often by HOME scores. The HOME scales characterizing degree of parental demandingness concern the provision of appropriate play materials, opportunity for variety, developmentally appropriate rules, and cognitive stimulation in the home (Barrera, Cunningham, & Rosenbaum, 1986b; Feldman, Eidelman, Sirota, & Weller, 2002; Smith, Brooks-Gunn, Kohen, & McCarton, 2001). Increased parental demandingness may be associated with subsequent improved child standardized cognitive scores (e.g. Bayley Scales of Infant and Toddler Development) as it establishes an early framework for learning (Davis-Kean, 2005).
Structure is synonymous with parental assertive control and/or consistency. This axis is characterized in studies by standardized scales for coding the quality of assistance to the child during problem solving (Berlin, Brooks-Gunn, McCarton, & McCormick, 1998), the organization of the child’s physical environment (Feldman, Eidelman, Sirota, & Weller, 2002), parenting consistency (Brown, Speechley, Macnab, Natale, & Campbell, 2014), or the ability to sustain the child’s attention (Hebert, 2002). As with demandingness, parental structure is associated with improved cognition in former preterm infants. Parental structure is also associated with less internalizing and externalizing behavioral problems in these children (Bagner, Sheinkopf, Vohr, & Lester, 2010; Berlin, Brooks-Gunn, Spiker, & Zaslow, 1995; Blair, Peters, & Lawrence 2003). These associations may be mediated via the positive control pathways of teaching and guidance (Dwairy & Achoui, 2010).
Several studies measured parental responsivity using the emotional and verbal responsiveness scale of the HOME score (Barrera, Rosenbaum, & Cunningham, 1986a; Feldman, Eidelman, Sirota, & Weller, 2002; Melnyk et al., 2001), while others utilized coding rubrics (Smith et al., 2000; Smith et al., 2006). In some studies, responsivity was difficult to distinguish from warmth (Smith et al., 1996; Treyvaud et al., 2009; Treyvaud et al., 2016). For the purposes of this review, responsivity was more narrowly characterized as parental sensitivity, such that a parent responds to a child’s signaling (Johnson et al., 2009; Treyvaud et al., 2009; Treyvaud et al., 2016). This concept is well described in attachment theory (Dilworth-Bart, Miller, & Hane, 2012) and may explain why parental responsivity is strongly associated with improved child cognitive and behavioral outcomes in former preterm infants. These outcomes include improved scores on standard assessments such as the Bayley and Stanford Binet tests, increased math, language, and reading skills and decreased emotional symptoms, conduct problems, hyperactivity, and/or peer difficulties (Feldman, Eidelman, Sirota, & Weller, 2002; Smith et al., 2001; Treyvaud et al., 2016).
Parental autonomy support is coded as the degree to which the parent provides nondirective support and respects the child’s independence during a parent-child observation task (Schappin et al., 2013; Smith et al., 1996; Treyvaud et al., 2009; Treyvaud et al., 2016). Autonomy support is associated with improved cognitive scores on the Bayley and other standardized tests, as well as improved receptive and expressive language in former preterm infants. It is not associated with improved (or worse) child behavioral outcomes such as internalizing and externalizing behaviors (Schappin et al., 2013; Smith et al., 1996; Treyvaud et al., 2009). Given the relative fewer numbers of studies for autonomy support and child behavior, more studies may be needed to capture a relationship if one does indeed exist (see Figure 2b).
Parental coercion is coded during parent-child tasks using various instruments that determine parental intrusiveness, restrictiveness, taking over for the child too quickly, over controlling or directive behaviors (Dilworth-Bart, Miller, & Hane, 2012; Foster-Cohen, Friesen, Champion, & Woodward, 2010; Hebert, 2002; Poehlmann et al., 2011; Poehlmann et al., 2012; Shah, Robbins, Coelho, & Poehlmann, 2013; Smith et al., 1996; Smith, Landry, & Swank, 2000; Treyvaud et al., 2009; Treyvaud et al., 2016). Aggregate data support no positive or negative associations between parental coercion and subsequent child outcomes in former preterm infants. Cognition, language and math skills, delay of gratification, internalizing and externalizing behaviors, and/or peer difficulty all appear unaffected by parenting with a high degree of coercion (Foster-Cohen, Friesen, Champion, & Woodward, 2010; Hebert, 2002; Poehlmann et al., 2011; Treyvaud et al., 2009; Treyvaud et al., 2016). It is possible that greater parental directiveness does not hinder the development of former preterm children in the same way that it might full term children, perhaps through a secondary reduction in parental stress or some other parental gain in this specific population (Dwairy & Achoui, 2010; Melnyk et al., 2006). However, more research is needed to explore these complex dynamics.
Many of the interventional studies that met inclusion criteria for this systematic review had very low quality of evidence, primarily due to indirectness and/or poorly measured parenting axes, which were the determinants of interest for this review (see supplemental table 1 for more details). However, since the ultimate goal of this work is to promote the best outcomes for former preterm infants by understanding and eventually leveraging parenting style, some of the interventions that were higher quality for this review can offer valuable insights. The Infant Health and Development Program (IHDP) increased parental warmth and structure and was associated with improved child cognitive and behavioral outcomes (Berlin, Brooks-Gunn, McCarton, & McCormick, 1998; Blair, Peters, & Lawrence 2003). The IHDP was an intensive program that followed preterm infants from hospital discharge to three years of age. This multi-center intervention included home visits every one to two weeks, Child Development Centers for approximately 20 hours per week after age 12 months, and parent groups every other month (Berlin, Brooks-Gunn, McCarton, & McCormick, 1998). Sustained neurodevelopmental improvement at 5 years was noted for heavier (2001–2500 grams) but not lighter (≤2000 grams) preterm infants. This intervention also interacted with social variables, such as maternal education, such that children of less educated mothers benefitted more from the intervention than did children of more educated mothers (Berlin, Brooks-Gunn, McCarton, & McCormick, 1998).
A Kangaroo Care intervention improved parental warmth, responsivity, and demandingness, as well as six-month cognitive scores in children as compared to a matched control group without the intervention. Longer-term development was not followed (Feldman, Eidelman, Sirota, & Weller, 2002). Finally, Primary Care Triple P was an intervention that consisted of four sessions for parents of former preterm infants that began when the children were two to five years of age. This three and a half day training over two months focused on parental skills training. Parents also completed a standardized evaluation at the end of the training to demonstrate mastery of the material. This intervention did not alter the parenting axes of warmth, rejection, autonomy support, and demandingness nor was it associated with any change in child behavioral outcomes (Schappin et al., 2013).
These, and other interventions, highlight some key points and critical questions. First, child neurodevelopment is the constellation of genetics, medical course, and family, social, and environmental factors. Early intervention (EI) is not a cure all. Rather, EI seeks to modify one aspect of risk. In these cases, the goal of the EI was to boost family processes by way of improvements in parenting (Blair, Peters, & Lawrence 2003). The hope was that improvement in this one area could help promote the best development of the child, in spite of his/her other risk factors (for example, medical risk due to prematurity) (Berlin, Brooks-Gunn, McCarton, & McCormick, 1998). While the more effective interventions to alter parenting axes and subsequent child neurodevelopment in this review began at earlier ages, a full discussion of when to begin interventions, how long to continue them, and which population of premature infants should be targeted, although critical, is beyond the scope of this review.
Limitations of the review
Parenting style is an aggregate of several dimensions of dyadic behavior that build a social-emotional scaffolding for infant development. Because parenting style is difficult to define, we leveraged concepts and semantics in the current literature to study one possible framework. Others could certainly be conceptualized and evaluated, but the rigorous methodology of the current review would remain sound. The parenting style axes we included were based on qualitative measurements that could be subject to observer bias, although all demonstrated high inter-rater reliabilities. Some definitions of axes were more likely to impact certain outcomes. For example, in one study, the axis of autonomy support was defined as support to help the child manage emotions, behavior, and engage well. This definition suggests a direct association between autonomy support and child behavior (Treyvaud et al., 2016). However, since definitions varied among studies, examining the data in aggregate should have minimized the limitations of individualized definitions in a single study. For some studies, axes were not as clearly separated as in the review methodology. For example, the axis of responsivity can contain an element of warmth (Treyvaud et al., 2016). Accordingly, the level of evidence was downgraded for the studies without clearly defined axes.
Each axis was represented in few studies and many focused on a modifier of parenting style, such as child temperament (Dilworth-Bart, Miller, & Hane, 2012) or neonatal pain (Vinall, Miller, Synnes, & Grunau, 2013), on child outcome. Thus, quality of evidence from these studies was lower due to indirectness of measurements, unless the effects of parenting style axes were also analyzed without the modifier. Finally, several of the included studies examined parent-child synchrony, which can impact child developmental outcomes (Treyvaud et al., 2009; Treyvaud et al., 2016). Our review explored only the parental contribution to this dyadic relationship on child developmental outcomes. Other studies have focused on the child component of the dyad and on the effects of synergy on development. Finally, in addition to the parenting axes and parenting style, many other social, medical, and environmental factors not in the scope of this review contribute to child neurodevelopmental outcomes, although studies on parenting generally control or match for these variables.
Given the limited number of studies examining each child outcome, in our framework, we grouped all cognitive outcomes and all behavioral outcomes together as long as they were measured with standardized assessments. Cognitive outcomes included cognitive developmental testing, such as Bayley scores, as well as standardized evaluation of language, math, or reading skills (see supplemental Table 1 for exact outcome per study). Behavioral outcomes included internalizing and externalizing tendencies, social-emotional competence, and delay of gratification skills, among others. Given the multiplicity of assessment tools, it is possible that associations exist for a specific child behavioral outcome (for example, internalizing behaviors) that are diluted by the inclusion of all behavioral outcomes. However, not enough studies exist in the literature to date to separate out each individual component of child cognition and/or behavior. Similarly, for the ages at assessment, we attempted to provide an inclusive overview of early childhood, by mandating that subjects initially be assessed before the age of two years. As can be seen in our supplemental table of included studies, additional ages of assessment were in fact variable within the range of 1–7 years. Finally, we included all preterm infants rather than only extremely (<28 weeks) or late (34–37 weeks) preterm infants. However, limiting the literature to only one stratum of preterm infants would have prevented any systematic review. Future studies may be designed with consistent and specific cognitive and behavioral assessment tools, using a longitudinal schedule targeted to preterm infants and accounting for gestational age at birth.
Conclusion
The overall quality of evidence for the 27 studies we reviewed ranged from very low to high with a skew towards lower quality of evidence, usually due to imprecise characterization of parenting style axes. When all studies were considered in aggregate, recommendations would be strongly in favor of parental responsivity to improve cognitive outcomes of preterm infants and also (but with less accumulated evidence) in favor of demandingness. To improve behavioral outcomes of preterm infants, strong recommendations can be made in favor of parental styles emphasizing warmth, and to a lesser degree, responsivity. Therefore, for preterm infants, interventional studies targeting parenting style may need to consider training of responsivity, demandingness and warmth in combination. A more precise study distinguishing parental warmth from responsivity may also help determine if only one or both these axes may be beneficial in improving cognitive outcomes. The parenting axes most strongly associated with improved child cognitive and behavioral outcomes in former preterm infants are the most ideal targets for early intervention.
Supplementary Material
{kind=link}
Key Points.
This systematic review examines eight axes of parenting style and their associations with cognitive and behavioral outcomes of former preterm children in early childhood.
For behavioral measures, strong evidence indicates that parenting styles incorporating responsivity and warmth are associated with improved outcomes, while rejection is associated with worse outcomes and autonomy support and coercion do not appear to have any association with positive or negative outcomes.
For cognitive measures, the only strong evidence favors parental responsivity. Weaker evidence supports positive associations between parental demandingness, structure and autonomy support and improved child outcomes.
Acknowledgments
This work has been supported by NICHD T32 HD060554 and R01 HD081120 and by the John and Leslie Hooper Neonatal-Perinatal Medicine Endowment Fund. The authors would also like to thank Olena Chorna MM, MT-BC, CCRP, for her guidance.
Footnotes
The authors have no conflicts of interest to disclose.
Contributor Information
Mary Lauren M. Neel, Neonatal-Perinatal Medicine, Monroe Carell Jr. Children’s Hospital at Vanderbilt, Vanderbilt University Medical Center, mary.lauren.m.neel@vanderbilt.edu, 615-322-3476.
Ann R. Stark, Department of Pediatrics; Fellowship Program Director, Neonatal-Perinatal Medicine, Monroe Carell Jr. Children’s Hospital at Vanderbilt, Vanderbilt University Medical Center, ann.r.stark@vanderbilt.edu, 615-322-3475.
Nathalie L. Maitre, Department of Pediatrics; Principal Investigator, Center for Perinatal Research; Director, NICU Follow-Up Programs, Nationwide Children’s Hospital and the Ohio State University, nathalie.maitre@nationwidechildrens.org, 614-722-4559.
References
- 1.Aarnoudse-Moens CSH, Weisglas-Kuperus N, van Goudoever JB, Oosterlaan J. Meta-analysis of neurobehavioral outcomes in very preterm and/or very low birth weight children. Pediatrics. 2009;124:717–728. doi: 10.1542/peds.2008-2816. [DOI] [PubMed] [Google Scholar]
- 2.Achenbach TM, Rescorla LA. Research Center for Children, Youth, & Families. Burlington, VT, USA: University of Vermont; 2000. Manual for the ASEBA Preschool Forms and Profiles. [Google Scholar]
- 3.Albers CA, Grieve AJ. Test review: Bayley, N. (2006). Bayley scales of infant and toddler development–third edition. San Antonio, TX: Harcourt assessment. Journal of Psychoeducational Assessment. 2007;25:180–190. doi: 10.1177/0734282906297199. [DOI] [Google Scholar]
- 4.Aylward GP. Neurodevelopmental outcomes of infants born prematurely. Journal of Developmental & Behavioral Pediatrics. 2005;26:427–440. doi: 10.1097/01.DBP.0000452240.39511.d4. [DOI] [PubMed] [Google Scholar]
- 5.Bagner DM, Sheinkopf SJ, Vohr BR, Lester BM. Parenting intervention for externalizing behavior problems in children born premature: An initial examination. Journal of developmental and behavioral pediatrics: JDBP. 2010;31:209–216. doi: 10.1097/DBP.0b013e3181d5a294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Barrera ME, Cunningham CE, Rosenbaum PL. Low birth weight and home intervention strategies: preterm infants. Journal of Developmental & Behavioral Pediatrics. 1986b;7:361–366. [PubMed] [Google Scholar]
- 7.Barrera ME, Rosenbaum PL, Cunningham CE. Early home intervention with low-birth-weight infants and their parents. Child development. 1986a;57:20–33. doi: 10.2307/1130634. [DOI] [PubMed] [Google Scholar]
- 8.Baumrind D. Effects of authoritative parental control on child behavior. Child development. 1966;37:887–907. doi: 10.2307/1126611. [DOI] [Google Scholar]
- 9.Baumrind D. Patterns of parental authority and adolescent autonomy. New directions for child and adolescent development. 2005;2005(108):61–69. doi: 10.1002/cd.128. [DOI] [PubMed] [Google Scholar]
- 10.Berlin LJ, Brooks-Gunn J, McCarton C, McCormick MC. The effectiveness of early intervention: examining risk factors and pathways to enhanced development. Preventive medicine. 1998;27:238–245. doi: 10.1006/pmed.1998.0282. [DOI] [PubMed] [Google Scholar]
- 11.Berlin LJ, Brooks-Gunn J, Spiker D, Zaslow MJ. Examining observational measures of emotional support and cognitive stimulation in black and white mothers of pre-schoolers. Journal of Family Issues. 1995;16:664–686. doi: 10.1177/019251395016005008. [DOI] [Google Scholar]
- 12.Bhutta AT, Cleves MA, Casey PH, Cradock MM, Anand KJS. Cognitive and behavioral outcomes of school-aged children who were born preterm: a meta-analysis. Jama. 2002;288(6):728–737. doi: 10.1001/jama.288.6.728. [DOI] [PubMed] [Google Scholar]
- 13.Blair C, Peters R, Lawrence F. Family dynamics and child outcomes in early intervention: The role of developmental theory in the specification of effects. Early Childhood Research Quarterly. 2003;18:446–467. doi: 10.1016/j.ecresq.2003.09.005. [DOI] [Google Scholar]
- 14.Bradley RH, Whiteside L, Mundfrom DJ, Casey PH, Kelleher KJ, Pope SK. Early indications of resilience and their relation to experiences in the home environments of low birthweight, premature children living in poverty. Child development. 1994;65:346–360. doi: 10.1111/j.1467-8624.1994.tb00755.x. [DOI] [PubMed] [Google Scholar]
- 15.Brown HK, Speechley KN, Macnab J, Natale R, Campbell MK. Mild prematurity, proximal social processes, and development. Pediatrics. 2014;134:e814–e824. doi: 10.1542/peds.2013-4092. [DOI] [PubMed] [Google Scholar]
- 16.Carter AS, Briggs-Gowan MJ, Jones SM, Little TD. The Infant–Toddler Social and Emotional Assessment (ITSEA) Boston, MA: University of Massachusetts Boston Department of Psychology, Boston, MA. Yale University; 2000. [Google Scholar]
- 17.Carter AS, Briggs-Gowan MJ. Manual of the Infant-Toddler Social-Emotional Assessment. New Haven, CT: Yale University; 2000. [Google Scholar]
- 18.Chyi LJ, Lee HC, Hintz SR, Gould JB, Sutcliffe TL. School outcomes of late preterm infants: special needs and challenges for infants born at 32 to 36 weeks gestation. The Journal of pediatrics. 2008;153(1):25–31. doi: 10.1016/j.jpeds.2008.01.027. [DOI] [PubMed] [Google Scholar]
- 19.Davis-Kean PE. The influence of parent education and family income on child achievement: the indirect role of parental expectations and the home environment. Journal of family psychology. 2005;19:294–304. doi: 10.1037/0893-3200.19.2.294. [DOI] [PubMed] [Google Scholar]
- 20.Dijkers M. Introducing GRADE: a systematic approach to rating evidence in systematic reviews and to guideline development. KT Update. 2013;1:1–9. [Google Scholar]
- 21.Dilworth-Bart JE, Miller KE, Hane A. Maternal play behaviors, child negativity, and preterm or low birthweight toddlers’ visual–spatial outcomes: Testing a differential susceptibility hypothesis. Infant Behavior and Development. 2012;35:312–322. doi: 10.1016/j.infbeh.2011.11.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Dunn LM, Dunn LM. Manual for the peabody picture vocabulary test-revised. Circle Pines, MN: American Guidance Service; 1981. [Google Scholar]
- 23.Dwairy M, Achoui M. Parental control: A second cross-cultural research on parenting and psychological adjustment of children. Journal of Child and Family Studies. 2010;19:16–22. doi: 10.1007/s10826-009-9334-2. [DOI] [Google Scholar]
- 24.Eyberg SM, Pincus D. Eyberg child behavior inventory and sutter-eyberg student behavior inventory-revised: Professional manual. Lutz, FL: Psychological Assessment Resources; 1999. [Google Scholar]
- 25.Feldman R, Eidelman AI, Sirota L, Weller A. Comparison of skin-to-skin (kangaroo) and traditional care: parenting outcomes and preterm infant development. Pediatrics. 2002;110:16–26. doi: 10.1542/peds.110.1.16. [DOI] [PubMed] [Google Scholar]
- 26.Foster-Cohen SH, Friesen MD, Champion PR, Woodward LJ. High prevalence/low severity language delay in preschool children born very preterm. Journal of Developmental & Behavioral Pediatrics. 2010;31:658–667. doi: 10.1097/DBP.0b013e3181e5ab7e. [DOI] [PubMed] [Google Scholar]
- 27.Goodman R. The Strengths and Difficulties Questionnaire: a research note. Journal of child psychology and psychiatry. 1997;38:581–586. doi: 10.1111/j.1469-7610.1997.tb01545.x. [DOI] [PubMed] [Google Scholar]
- 28.Hall RAS, Hoffenkamp HN, Tooten A, Braeken J, Vingerhoets AJJM, van Bakel HJA. Longitudinal associations between maternal disrupted representations, maternal interactive behavior and infant attachment: a comparison between full-term and preterm dyads. Child Psychiatry & Human Development. 2015;46:320–331. doi: 10.1007/s10578-014-0473-3. doi: 10.1007%2Fs10578-014-0473-3. [DOI] [PubMed] [Google Scholar]
- 29.Hall RA, Hoffenkamp HN, Tooten A, Braeken J, Vingerhoets AJ, van Bakel HJ. The Quality of Parent–Infant Interaction in the First 2 Years After Full-Term and Preterm Birth. Parenting. 2015;15:247–268. doi: 10.1080/15295192.2015.1053333. [DOI] [Google Scholar]
- 30.Hartling L, Hamm MP, Milne A, Vandermeer B, Santaguida PL, Ansari M, Dryden DM. Testing the risk of bias tool showed low reliability between individual reviewers and across consensus assessments of reviewer pairs. Journal of Clinical Epidemiology. 2013;66:973–981. doi: 10.1016/j.jclinepi.2012.07.005. [DOI] [PubMed] [Google Scholar]
- 31.Hebert HM. Unpublished doctoral dissertation. University of Houston; Houston, TX: 2002. The relationships among play, language development and parenting in children born prematurely with medical complications. [Google Scholar]
- 32.Hedrick DL, Prather EM, Tobin AR. Sequenced inventory of communication development: Instruction manual. Seattle, WA: University of Washington Press; 1984. [Google Scholar]
- 33.Herd M, Whittingham K, Sanders M, Colditz P, Boyd RN. Efficacy of preventative parenting interventions for parents of preterm infants on later child behavior: a systematic review and meta-analysis. Infant mental health journal. 2014;35:630–641. doi: 10.1002/imhj.21480. [DOI] [PubMed] [Google Scholar]
- 34.Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, Sterne JA. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Bmj. 2011;343:d5928. doi: 10.1136/bmj.d5928.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Hofstra MB, Van Der Ende J, Verhulst FC. Child and adolescent problems predict DSM-IV disorders in adulthood: a 14-year follow-up of a Dutch epidemiological sample. Journal of the American Academy of Child & Adolescent Psychiatry. 2002;41:182–189. doi: 10.1097/00004583-200202000-00012. [DOI] [PubMed] [Google Scholar]
- 36.Indredavik MS, Vik T, Heyerdahl S, Kulseng S, Fayers P, Brubakk AM. Psychiatric symptoms and disorders in adolescents with low birth weight. Archives of Disease in Childhood-Fetal and Neonatal Edition. 2004;89:F445–F450. doi: 10.1136/adc.2003.038943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Johnson S, Whitelaw A, Glazebrook C, Israel C, Turner R, White IR, Marlow N. Randomized trial of a parenting intervention for very preterm infants: outcome at 2 years. The Journal of paediatrics. 2009;155:488–494. doi: 10.1016/j.jpeds.2009.04.013. [DOI] [PubMed] [Google Scholar]
- 38.Kinney HC. The near-term (late preterm) human brain and risk for periventricular leukomalacia: a review. Seminars in perinatology. 2006;30(2):81–88. doi: 10.1053/j.semperi.2006.02.006. [DOI] [PubMed] [Google Scholar]
- 39.Margulis AV, Pladevall M, Riera-Guardia N, Varas-Lorenzo C, Hazell L, Berkman ND, Perez-Gutthann S. Quality assessment of observational studies in a drug-safety systematic review, comparison of two tools: the Newcastle–Ottawa scale and the RTI item bank. Clinical epidemiology. 2014;6:359–368. doi: 10.2147/CLEP.S66677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Martin JA, Hamilton BE, Osterman MJK. Births in the United States, 2016. NCHS data brief. 2017;287:1–8. [PubMed] [Google Scholar]
- 41.Maupin AN, Fine JG. Differential effects of parenting in preterm and full-term children on developmental outcomes. Early human development. 2014;90:869–876. doi: 10.1016/j.earlhumdev.2014.08.014. [DOI] [PubMed] [Google Scholar]
- 42.Melnyk BM, Alpert-Gillis L, Feinstein NF, Fairbanks E, Schultz-Czarniak J, Hust D, Bender N. Improving cognitive development of low-birth-weight premature infants with the COPE program: A pilot study of the benefit of early NICU intervention with mothers. Research in nursing & health. 2001;24:373–389. doi: 10.1002/nur.1038. [DOI] [PubMed] [Google Scholar]
- 43.Melnyk BM, Feinstein NF, Alpert-Gillis L, Fairbanks E, Crean HF, Sinkin RA, Gross SJ. Reducing premature infants' length of stay and improving parents' mental health outcomes with the Creating Opportunities for Parent Empowerment (COPE) neonatal intensive care unit program: a randomized, controlled trial. Pediatrics. 2006;118:e1414–e1427. doi: 10.1542/peds.2005-2580. [DOI] [PubMed] [Google Scholar]
- 44.Novak I, Mcintyre S, Morgan C, Campbell L, Dark L, Morton N, Goldsmith S. A systematic review of interventions for children with cerebral palsy: state of the evidence. Developmental Medicine & Child Neurology. 2013;55:885–910. doi: 10.1111/dmcn.12246. [DOI] [PubMed] [Google Scholar]
- 45.Petrini JR, Dias T, McCormick MC, Massolo ML, Green NS, Escobar GJ. Increased risk of adverse neurological development for late preterm infants. The Journal of pediatrics. 2009;154(2):169–176. doi: 10.1016/j.jpeds.2008.08.020. [DOI] [PubMed] [Google Scholar]
- 46.Poehlmann J, Hane A, Burnson C, Maleck S, Hamburger E, Shah PE. Preterm infants who are prone to distress: differential effects of parenting on 36-month behavioral and cognitive outcomes. Journal of Child Psychology and Psychiatry. 2012;53:1018–1025. doi: 10.1111/j.1469-7610.2012.02564.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Poehlmann J, Schwichtenberg AJM, Shlafer RJ, Hahn E, Bianchi JP, Warner R. Emerging self-regulation in toddlers born preterm or low birth weight: Differential susceptibility to parenting? Development and psychopathology. 2011;23:177–193. doi: 10.1017/S0954579410000726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Roid GH. Stanford-Binet intelligence scales. Rolling Meadows, IL: Riverside Publishing; 2003. [Google Scholar]
- 49.Schappin R, Wijnroks L, Venema MU, Wijnberg-Williams B, Veenstra R, Koopman-Esseboom C, Jongmans M. Brief parenting intervention for parents of NICU graduates: a randomized, clinical trial of Primary Care Triple P. BMC paediatrics. 2013;13:69. doi: 10.1186/1471-2431-13-69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Semel E, Wiig EH, Secord WH. Clinical Evaluation of Language Fundamentals. San Antonio, TX: The Psychological Corporation; 2003. [Google Scholar]
- 51.Shah PE, Robbins N, Coelho RB, Poehlmann J. The paradox of prematurity: The behavioral vulnerability of late preterm infants and the cognitive susceptibility of very preterm infants at 36 months post-term. Infant Behavior and Development. 2013;36:50–62. doi: 10.1016/j.infbeh.2012.11.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Shea BJ, Hamel C, Wells GA, Bouter LM, Kristjansson E, Grimshaw J, Boers M. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. Journal of clinical epidemiology. 2009;62:1013–1020. doi: 10.1016/j.jclinepi.2008.10.009. [DOI] [PubMed] [Google Scholar]
- 53.Skinner E, Johnson S, Snyder T. Six dimensions of parenting: A motivational model. Parenting: Science and Practice. 2005;5:175–235. doi: 10.1207/s15327922par0502_3. [DOI] [Google Scholar]
- 54.Smith JR, Brooks-Gunn J, Kohen D, McCarton C. Transitions on and off AFDC: Implications for parenting and children's cognitive development. Child development. 2001;72:1512–1533. doi: 10.1111/1467-8624.00363. [DOI] [PubMed] [Google Scholar]
- 55.Smith KE, Landry SH, Swank PR. The influence of early patterns of positive parenting on children's preschool outcomes. Early Education and Development. 2000;11:147–169. doi: 10.1207/s15566935eed1102_2. [DOI] [Google Scholar]
- 56.Smith KE, Landry SH, Swank PR. The role of early maternal responsiveness in supporting school-aged cognitive development for children who vary in birth status. Pediatrics. 2006;117:1608–1617. doi: 10.1542/peds.2005-1284. [DOI] [PubMed] [Google Scholar]
- 57.Smith KE, Swank PR, Denson SE, Landry SH, Baldwin CD, Wildin S. The relation of medical risk and maternal stimulation with preterm infants' development of cognitive, language and daily living skills. Journal of Child Psychology and Psychiatry. 1996;37:855–864. doi: 10.1111/j.1469-7610.1996.tb01481.x. [DOI] [PubMed] [Google Scholar]
- 58.Talge NM, Holzman C, Wang J, Lucia V, Gardiner J, Breslau N. Late-preterm birth and its association with cognitive and socioemotional outcomes at 6 years of age. Pediatrics. 2010;126(6):1124–1131. doi: 10.1542/peds.2010-1536. [DOI] [PubMed] [Google Scholar]
- 59.Treyvaud K, Anderson VA, Howard K, Bear M, Hunt RW, Doyle LW, Anderson PJ. Parenting behavior is associated with the early neurobehavioral development of very preterm children. Pediatrics. 2009;123:555–561. doi: 10.1542/peds.2008-0477. [DOI] [PubMed] [Google Scholar]
- 60.Treyvaud K, Doyle LW, Lee KJ, Ure A, Inder TE, Hunt RW, Anderson PJ. Parenting behavior at 2 years predicts school-age performance at 7 years in very preterm children. Journal of Child Psychology and Psychiatry. 2016;57:814–821. doi: 10.1111/jcpp.12489. [DOI] [PubMed] [Google Scholar]
- 61.Vinall J, Miller SP, Synnes AR, Grunau RE. Parent behaviors moderate the relationship between neonatal pain and internalizing behaviors at 18 months corrected age in children born very prematurely. PAIN®. 2013;154:1831–1839. doi: 10.1016/j.pain.2013.05.050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Viswanathan M, Berkman ND. Development of the RTI item bank on risk of bias and precision of observational studies. Journal of clinical epidemiology. 2012;65:163–178. doi: 10.1016/j.jclinepi.2011.05.008. [DOI] [PubMed] [Google Scholar]
- 63.Wechsler D. Wechsler abbreviated intelligence scale. San Antonio, TX: The Psychological Corporation; 1999. [Google Scholar]
- 64.Woythaler MA, McCormick MC, Smith VC. Late preterm infants have worse 24-month neurodevelopmental outcomes than term infants. Pediatrics. 2011;127(3):e622–e629. doi: 10.1542/peds.2009-3598. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.