

Abstract
Nocturia is a complex condition that not only significantly affects quality of life, but may be an indicator of systemic disease. Initial assessment includes a detailed history and physical examination and completion of a frequency volume chart to help identify underlying causes, such as sleep disorders, bladder storage disorders, and polyuria. Treatment with alpha-blockers or antimuscarinic medications may help if the underlying cause is determined to be benign prostatic hyperplasia or overactive bladder, respectively. Treatment options for nocturnal polyuria have been limited to behavioral therapy and off-label use of timed diuretics and desmopressin. Desmopressin acetate nasal spray (Noctiva™, Avadel Pharmaceuticals, Chesterfield, MO) was approved by the US Food and Drug Administration in 2017 for the treatment of nocturia due to nocturnal polyuria in adults who awaken at least twice nightly and has shown efficacy in reducing nocturnal voids by ≥50% in up to 49% of patients in clinical trials.
Keywords: Nocturia, Benign prostatic hyperplasia, Overactive bladder, Nocturnal polyuria, Desmopressin
In 2002, the International Continence Society defined nocturia as the “complaint that an individual has to wake at night one or more times to void,” with night including the period of time between going to bed with the purpose of sleeping and awaking for the day.1 Additional definitions and parameters pertinent to a discussion about nocturia are included in Table 1. The prevalence of nocturia increases with age with up to 59% of men and 62% of women awakening at least twice per night by the age of 70 years. However, younger adults can also be impacted with 11% to 44% of men and women aged 20 to 40 years reporting nocturia at least once per night.2 Moderate to severe degrees of bother have been reported at all nocturia frequencies; however, degree of bother increases with nocturia frequency with about 70% reporting at least a small degree of bother with ≥2 nocturia voids.3 Additionally, nocturia was independently associated with Patient Perception of Bladder Condition severity.4
Table 1.
Terminology Associated with Nocturia
| Term | Definition |
|---|---|
| Maximal voiding volume | Volume of urine in bladder prior to void; functional bladder capacity10 |
| Polyuria | 24-hour voided volume .2.8 L43 |
| Nocturnal urine volume | Total volume of urine passed during the night including the first morning void43 |
| Nocturnal polyuria | Nocturnal urine volume .20%-30% of total 24-hour urine volume (includes first morning void)43 |
| Nocturia index | Nocturnal urine volume/maximum voided volume10 |
| Nocturnal bladder capacity | Volume of urine prior to nocturia void |
| Nocturnal bladder capacity index | Corresponds to the actual number of voids minus the predicted number of voids,10 reflective of nocturnal bladder capacity |
| Nocturnal polyuria index | Nocturnal urine volume/24-hour urine volume44 |
Nocturia is more than a bother that influences quality of life—it may also be an indicator of underlying disease. Nocturia has been associated with depressive symptoms,5 an increased rate of falls,6,7 and a greater risk of all-cause mortality.8 The economic impact of nocturia on society is costly with direct costs related to treatment estimated to be ≥1.5 billion/year.9 The indirect costs of decreased work productivity, poor concentration, and increased time away from work are estimated to be up to ≥61 billion/year. Given the significant co-morbidity associated with nocturia and the societal costs, this symptom, often dismissed by patients and providers, deserves close and careful evaluation.
Etiology of Nocturia
The cause of nocturia is often multifactorial and can include behavioral or sleep problems, impaired bladder storage (eg, overactive bladder, reduced bladder capacity), urine volume factors (eg, 24-hour polyuria or nocturnal polyuria), or other factors such as medication or alcohol use.10,11 Behavioral influences, such as the amount and timing of fluid intake and primary sleep disturbances such as insomnia, will affect nocturia. It is important to try and distinguish if patients are awakening due to the need to void or if they decide to use the bathroom once awake (nocturnal convenience void). Bladder storage symptoms such as urinary frequency and urgency may co-exist with nocturia. Reduced bladder capacity can be anatomic or functional and may be associated with retention of urine from bladder outlet obstruction (BOO) secondary to benign prostatic hyperplasia (BPH). Urine volume factors are often a result of underlying systemic disease such as congestive heart failure, obstructive sleep apnea (OSA), or poorly controlled diabetes. Patients with untreated OSA have chronic hypoxia and pulmonary vasoconstriction resulting in increased atrial natriuretic peptide levels, which leads to increased renal sodium and water excretion. States of fluid overload, as seen with congestive heart failure or advanced kidney disease, can causes significant fluid redistribution in the supine position, leading to increased urine production. Certain medications, such as lithium, cause a drug-induced nephrogenic diabetes insipidus. It is also possible that an individual patient has multiple contributing factors to the etiology of nocturia.
Assessment of Nocturia
The evaluation of nocturia is complex given all the potential contributing factors but begins with a thorough history including assessment of other lower urinary tract symptoms (LUTS), such as daytime frequency, urgency, and incontinence, fluid intake, and associated diseases. Use of validated questionnaires, such as the International Prostate Symptom Score (IPSS) and American Urological Association Symptom Index (AUA-SI),12 at the initial evaluation may be helpful to elucidate symptoms and to follow treatment progress. On physical examination, attention should be given to the presence of peripheral edema, bladder distention, orthostatic hypotension, and obesity as clues to the underlying etiology.
Completion of a frequencyvolume chart (FVC) over 2 to 3 days is recommended by the AUA Guidelines in patients with ≥2 nocturia episodes.13 The FVC will help identify 24-hour polyuria and nocturnal polyuria as causes of nocturia. If the nocturnal urine volume exceeds the maximum voided volume (nocturia index) or is greater than the nocturnal bladder capacity (nocturnal bladder capacity index), then nocturia will occur. The nocturnal bladder capacity index will be >0 if the nocturnal bladder capacity is less than the maximal voiding volume, indicating that the functional bladder capacity is lower at night than during the day. Figure 1 displays the potential causes of nocturia based on findings from the FVC.
Figure 1.
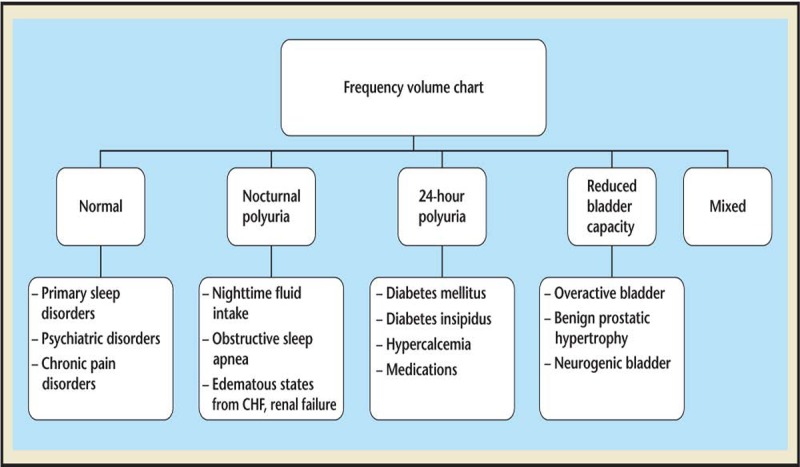
Diagnosing the cause of nocturia based on the frequency volume chart. CHF, congestive heart failure.
Management of Nocturia
Behavioral Interventions
Treatment of nocturia of any cause should begin with conservative measures such as education about the normal physiology of the bladder and behavioral interventions that can improve nocturnal voids.14,15 Decreasing overall fluid intake, limiting nighttime fluids, and avoidance of caffeine and alcohol can provide benefit.13,16 If appropriate, altering the timing of diuretic medication administration, use of compressive stockings, and leg elevation in the early evening may decrease nocturnal urine volume. Treatment of OSA with continuous positive airway pressure has been shown to decrease nocturia.17 Importantly, consideration of environmental conditions to prevent complications related to nocturia include use of a bedside urinal or commode and a clear, lighted path to the bathroom to reduce the risk of falls.
Behavioral Interventions
Approximately 30% of patients with nocturia also report OAB symptoms. 18 Antimuscarinics, including solifenacin,19 fesoterodine,20 tolterodine, 21 and mirabegron22 have been compared with placebo and in general have demonstrated about a 30% reduction in nighttime voids (versus placebo), despite improvement in LUTS. One study suggests that patients with more severe urgency in the absence of nocturnal polyuria may derive more benefit from treatment of OAB.21 Similarly, onabotulinum toxin injection into the bladder has shown limited improvements with a decrease of 0.5 nocturia episodes versus 0.25 with placebo.23,24 Sacral neuromodulation has demonstrated reductions in nocturnal voids across all ages groups,25 but also may be most beneficial in improving nocturia in those patients with more severe OAB symptoms.
Benign Prostatic Hyperplasia
Treatment of bladder outlet obstruction secondary to BPH, either medically or surgically, is thought to improve nocturia by lowering postvoid residual volume and increasing functional bladder capacity. alpha- Blocker therapy has been shown to have modest benefit in decreasing nocturia episodes. In a pooled analysis of three double-blinded placebo-controlled studies, alfuzosin, 10mg, demonstrated a significant improvement in the nocturia component of IPSS questionnaire.26 In a cohort study of tamsulosin, 18% of men had a significant reduction in the number of nocturia episodes.27 Addition of zolpidem28 and antimuscarinics29 to alpha-blockers may provide additional benefits in men with sleep disorders and OAB, respectively. Reductions in nocturnal voids following surgical treatment of BPH (prostatectomy or transurethral resection of the prostate) were like those reported with alpha-blocker therapy.30,31 Overall, surgical treatment of BPH demonstrated limited improvements in nocturia despite improved overall LUTS.
Other Medications
Use of timed loop diuretics, specifically bumetanide and furosemide, has also been trialed to reduce nocturia, functionally reducing nocturia episodes by shifting nighttime urine volume to daytime voids. In men with nocturnal polyuria randomized to furosemide 6 hours prior to bedtime, there were improvements in nighttime voids and nocturnal urine volume, but no differences on the IPSS were noted.32 Given the risks associated with longterm diuretic use, including azotemia, hearing loss, tinnitus, and electrolyte abnormalities (hypokalemia) and the unknown long-term efficacy on nocturia, these medications are not recommended for the primary treatment of nocturia.
Melatonin has been studied in a population of men with nocturia and BOO and was not found to have significant improvement in reducing nocturia.33 Patients with nocturia resulting from a primary sleep disorder may derive benefit from melatonin, but it is unlikely an adequate treatment option for most patients.
Nonsteroidal anti-inflammatory drugs (NSAIDs) have also been examined for possible improvements in nocturia due to a theoretical effect of reduced inflammation as well as decreased urine output due to lower glomerular filtration rate (GFR). In randomized studies of diclofenac and celecoxib, there were statistically significant improvements in nocturnal urine volume and nocturnal voids. Specifically, diclofenac reduced nocturia episodes from a baseline of 2.8 to 2.3 (vs to 2.7 with placebo) and mean nocturnal urine volume from a baseline of 836 mL to 745 mL (vs 802 mL with placebo). With celecoxib, there was a reduction in nocturia episodes from 5.2 to 2.5 in the treatment arm compared with 5.3 to 5.1 in the placebo arm. Despite these improvement, the side-effect profile of NSAIDs, including serious cardiovascular, renal, and gastrointestinal events, has prevented widespread use.
Desmopressin
Desmopressin is a synthetic analog of vasopressin, which is secreted by the posterior pituitary to increase water permeability by acting on renal collecting ducts via V2 receptors, leading to water reabsorption and decreased urine volume. Since the 1980s, several formulations (intranasal spray, oral tablets, and orally disintegrating tablets [ODT]) of desmopressin have been studied in patients with nocturnal polyuria. Desmopressin ODT (NOCDURNA®, Ferring Pharmaceuticals, Saint-Prez, Switzerland) is approved for use in Europe, Canada, and Australia for the treatment of nocturia voids in men and women.34 Desmopressin sublingual wafer (MINIRIN Melt®, Ferring Pharmaceuticals) is approved for nocturia in 80 countries for symptomatic nocturia.35 MINIRIN® is also available as an injectable solution and tablet. In tworandomized studies,45,46 desmopressin was found to be effective with 34–46% of subjects having a greater than 50% reduction in nocturnal voids versus 3-7% in the placebo group. The FDA advisory committee voted against approval of desmopressin to reduce nocturia in adults citing benefits did not outweigh the risk.47
Intranasal desmopressin has been available in the United States since the 1970s and has shown efficacy for the treatment of nocturnal polyuria in men with BPH but use for the treatment of nocturia was offlabel. 36 Desmopressin acetate nasal spray (DANS) (Noctiva™, Avadel Pharmaceuticals, Chesterfield, MO) is a novel formulation of intranasal desmopressin with the proposed benefit of more consistent efficacy and greater safety compared with oral formulations. It was approved by the US Food and Drug Administration in March 2017 and is indicated for the treatment of nocturia in adults who awaken ≥2 times per night to void.37 The active ingredient in DANS is a slight modification of desmopressin with the addition of cyclopentadecanolide, which is designed to enhance the absorption of the drug across nasal mucosa. It is available in strengths of 0.83 mcg and 1.66 mcg desmopressin acetate per 0.1 mL spray, equivalent to 0.75 mcg and 1.5 mcg desmopressin, respectively.37 Two proposed advantages of DANS include greater bioavailability (8% vs 0.3% with desmopressin ODT) that translates to decreased excess drug and potentially more consistent dosing. Rapid absorption and elimination may result in more rapid onset of efficacy, more predictable plasma levels, and should decrease the likelihood of prolonged drug activity.38
Two phase III clinical studies including 1542 patients have demonstrated the efficacy of DANS.38 The studied populations were predominantly male (57.8%) and over the age of 65 years (54.7%) and 80.5% had nocturnal polyuria.39 Co-primary endpoints, which in both studies reached statistical significance in both treatment arms compared with placebo, were (1) reduction in mean nocturia episodes and (2) percentage of subjects with a ≥50% reduction in mean nocturia episodes. In a pooled analysis, the average decrease in mean nocturia episodes was 20.3 (1.5 mcg) and 20.2 (0.75 mcg) compared with placebo. A ≥50% reduction in mean nocturia episodes was achieved by 48.5% and 37.9% of patients in the 1.5 mcg and 0.75 mcg arms, respectively, compared with 30% in the placebo group (Integrated Summary of Efficacy of the two phase III trials). Additionally, the treatment groups demonstrated clinically meaningful improvements in patient-reported impacts of nocturia on activities of daily living. Treatment efficacy was maintained at a follow-up of up to 2 years.
The safety of DANS was evaluated in four randomized trials and three-open label, long-term studies and overall was found to be well tolerated, although it was associated with an increase in adverse events compared with placebo. Discontinuation rates were 4.0%, 4.4%, and 2.3% in the 0.75 mcg, 1.5 mcg, and placebo groups, respectively. The most common reason for discontinuation was hyponatremia, defined as serum sodium #125 mmol/L with or without symptoms or serum sodium level between 126 and 129 mmol/L with symptoms and was reported in 1.2%, 0.9%, and 0.3% of the groups, respectively.38 Nearly half of the incidences of serum sodium #129 mmol/L occurred within the first 2 weeks of initiating treatment. Patients over the age of 65 years had a modestly increased rate of serum sodium,135 mmol/L (19%) compared with the overall population (14%). Overall, rates of hyponatremia were like those observed in clinical trials of desmopressin ODT.40 For the desmopressin melt, there was a reported 4%-6% incidence of hyponatremia in the treatment groups.45,46 Other reported adverse events included nasal discomfort, nasal congestion, nasopharyngitis, epistaxis, and bronchitis. DANS is contraindicated in patients with hyponatremia or a history of hyponatremia, polydipsia, primary nocturnal enuresis, concomitant use of loop diuretics or systemic or inhaled glucocorticoids, GFR, <50 mL/min/1.73 m2, syndrome of inappropriate antidiuretic hormone secretion, congestive heart failure, and uncontrolled hypertension.37
Although the risk is low, given the serious consequences of unrecognized hyponatremia monitoring is imperative. Serum sodium level should be obtained prior to initiation of treatment and then again within 7 days to 4 weeks of treatment start. Periodic monitoring should then be performed as appropriate with more frequent checks in patients over the age of 65 years and patients taking medications that may cause fluid retention, such as tricyclic antidepressants, selective serotonin re-uptake inhibitors, NSADs, and opiates.37 Additionally, in these higher risk patients (age ≥65 years or at risk for hyponatremia), treatment should be initiated at a dose of 0.83 mcg and increased to one spray of 1.66 mcg nightly after 7 days if the serum sodium is stable.
Ongoing Developments in Treatment of Nocturia
Fedovapagon is a potent vasopressin V2 receptor agonist that has demonstrated reductions in nocturnal urine volume in preliminary studies. A randomized, double-blind, placebo-controlled trial assessing efficacy of fedovapagon for the treatment of nocturia in men with BPH has been completed, but results are not yet available.41 A phase II study of SK-1404 (Sanwa Kagaku Kenkyusho Co., Ltd.) is a randomized trial underway in Japan with primary outcome of change from baseline of mean number of nocturnal voids assessed by voiding diary in men and women with nocturia. 42 The mechanism of SK-1404 is not widely available.
Main Points.
Nocturia is a complicated condition that requires identifying the underlying etiology for effective treatment.
With the aging population, the prevalence of nocturia will continue to increase.
Use of frequency volume charts can help elucidate the cause and guide treatment. Behavioral therapy and treatment with overactive bladder or benign prostatic hyperplasia medications may provide some benefit, although is generally inadequate in making significant improvements in nocturia.
Desmopressin acetate nasal spray (Noctiva™) is a novel formulation of intranasal desmopressin that has been shown to reduce nocturia episodes in patients awakening ≥2 times per night. Patient selection and attention to contraindications and monitoring recommendations regarding serum sodium are critical to maximize patient benefit and minimize risk using this safe and effective treatment for nocturia.
Conclusions
Nocturia is a complicated condition that requires identifying the underlying etiology for effective treatment. With the aging population, the prevalence of nocturia will continue to increase. Use of frequency volume charts can help elucidate the cause and guide treatment. Behavioral therapy and treatment with OAB or BPH medications may provide some benefit, although is generally inadequate in making significant improvements in nocturia. DANS (Noctiva™) is a novel formulation of intranasal desmopressin that has been shown to reduce nocturia episodes in patients awakening ≥2 times per night. Patient selection and attention to contraindications and monitoring recommendations regarding serum sodium are critical to maximize patient benefit and minimize risk using this safe and effective treatment for nocturia.
References
- 1.Van Kerrebroeck P, Abrams P, Chaikin D. The standardization of terminology in nocturia: report from the standardization subcommittee of the International Continence Society. BJU Int. 2002;90(3):11–15. doi: 10.1046/j.1464-410x.90.s3.3.x. [DOI] [PubMed] [Google Scholar]
- 2.Bosch JLHR, Weiss JP. The prevalence and causes of nocturia. J Urol. 2013;189:S86–S92. doi: 10.1016/j.juro.2012.11.033. [DOI] [PubMed] [Google Scholar]
- 3.Tikkinen KAO, Johnson TM II, Tammela TLJ. Nocturia frequency, bother, and quality of life: how often is too often? A population-based study in Finland. Eur Urol. 2010;57:488–498. doi: 10.1016/j.eururo.2009.03.080. [DOI] [PubMed] [Google Scholar]
- 4.Coyne KS, Wein AJ, Tubaro A. The burden of lower urinary tract symptoms: evaluating the effect of LUTS on health-related quality of life, anxiety and depression: EpiLUTS. BJU Int. 2009;103(3):4–11. doi: 10.1111/j.1464-410X.2009.08371.x. [DOI] [PubMed] [Google Scholar]
- 5.Kupelian V, Wei JT, O’Leary MP. Nocturia and quality of life: results from the Boston area community health survey. Eur Urol. 2012;61:78–84. doi: 10.1016/j.eururo.2011.05.065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Vaughan CP, Brown CJ, Goode PS. The association of nocturia with incident falls in an elderly community- dwelling cohort. Int J Clin Pract. 2010;64:577–583. doi: 10.1111/j.1742-1241.2009.02326.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Parsons JK, Mougey J, Lambert L. Lower urinary tract symptoms increase the risk of falls in older men. BJU Int. 2009;104:63–68. doi: 10.1111/j.1464-410X.2008.08317.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Endeshaw YW, Schwartz AV, Stone K. Nocturia, insomnia symptoms and mortality among older men: The Health, Aging and Body Composition Study. JCSM. 2016;12:789–796. doi: 10.5664/jcsm.5870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Holm-Larsen T. The economic impact of nocturia. Neurourol Urodyn. 2014;33:S10–S14. doi: 10.1002/nau.22593. [DOI] [PubMed] [Google Scholar]
- 10.Cornu J-N, Abrams P, Chapple CR. A contemporary assessment of nocturia: definition, epidemiology, pathophysiology, and management—a systematic review and meta-analysis. Eur Urol. 2012;62:877–890. doi: 10.1016/j.eururo.2012.07.004. [DOI] [PubMed] [Google Scholar]
- 11.Weiss JP, Blaivas JG, Bliwise DL. The evaluation and treatment of nocturia: a consensus statement. BJU Int. 2011;108:6–21. doi: 10.1111/j.1464-410X.2011.10175.x. [DOI] [PubMed] [Google Scholar]
- 12.Barry MJ, Fowler FJ, O’Leary MP. The American Urological Association Symptom Index for benign prostatic hyperplasia. J Urol. 1992;148:1549–1557. doi: 10.1016/s0022-5347(17)36966-5. [DOI] [PubMed] [Google Scholar]
- 13.McVary KT, Roehrborn CG, Alvins AL. Update on AUA guideline on the management of benign prostatic hyperplasia. J Urol. 2011;185:1793–1803. doi: 10.1016/j.juro.2011.01.074. [DOI] [PubMed] [Google Scholar]
- 14.Cho SY, Lee SL, Kim IS. Short-term effects of systematized behavioral modification program for nocturia: a prospective study. Neurourol Urodyn. 2012;31:64–68. doi: 10.1002/nau.21186. [DOI] [PubMed] [Google Scholar]
- 15.Soda T, Masui K, Okuno H. Efficacy of non-drug lifestyle measures for the treatment of nocturia. J Urol. 2010;184:1000–1004. doi: 10.1016/j.juro.2010.05.038. [DOI] [PubMed] [Google Scholar]
- 16.Hashim H, Abrams P. How should patients with an overactive bladder manipulate their fluid intake? BJU Int. 2008;102:62–66. doi: 10.1111/j.1464-410X.2008.07463.x. [DOI] [PubMed] [Google Scholar]
- 17.Margel D, Shochat T, Getzler O. Continuous positive airway pressure reduces nocturia in patients with obstructive sleep apnea. Urology. 2006;67:974–977. doi: 10.1016/j.urology.2005.11.054. [DOI] [PubMed] [Google Scholar]
- 18.Tikkinen KAO, Tammela TLJ, Rissanen AM. Is the prevalence of overactive bladder overestimated? A population-based study in Finland. PLoS ONE. 2007;2:e195. doi: 10.1371/journal.pone.0000195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Toglia MR, Ostergard DR, Appell RA. Solifenacin for overactive bladder: secondary analysis of data from VENUS based on baseline continence status. Int Urogynecol J. 2010;21:847–854. doi: 10.1007/s00192-010-1120-6. [DOI] [PubMed] [Google Scholar]
- 20.Dmochowski RR, Peters KM, Morrow JD. Randomized, double-blind, placebo-controlled trial of flexible-dose fesoterodine in subjects with overactive bladder. Urology. 2010;75:62–68. doi: 10.1016/j.urology.2009.09.018. [DOI] [PubMed] [Google Scholar]
- 21.Rackley R, Weiss JP, Rovner ES. Nighttime dosing with tolterodine reduces overactive bladderrelated nocturnal micturitions in patients with overactive bladder and nocturia. Urology. 2006;67:731–736. doi: 10.1016/j.urology.2005.10.061. [DOI] [PubMed] [Google Scholar]
- 22.Chapple CR, Cardozo L, Nitti VW. Mirabegron in overactive bladder: a review of efficacy, safety, and tolerability. Neurourol Urodyn. 2013;33:17–30. doi: 10.1002/nau.22505. [DOI] [PubMed] [Google Scholar]
- 23.Nitti VW, Dmochowski R, Herschorn S. OnabotulinumtoxinA for the treatment of patients with overactive bladder and urinary incontinence: results of a phase 3, randomized, placebo controlled trial. J Urol. 2017;197(2S):S216–S223. doi: 10.1016/j.juro.2016.10.109. [DOI] [PubMed] [Google Scholar]
- 24.Chapple C, Sievert K-D, MacDiarmid S. OnabotulinumtoxinA 100 U significantly improves all idiopathic overactive bladder symptoms and quality of life in patients with overactive bladder and urinary incontinence: a randomised, double-blind, placebocontrolled trial. Eur Urol. 2013;64:249–256. doi: 10.1016/j.eururo.2013.04.001. [DOI] [PubMed] [Google Scholar]
- 25.Peters KM, Killinger KA, Gilleran J. Does patient age impact outcomes of neuromodulation? Neurourol Urodyn. 2013;32:30–36. doi: 10.1002/nau.22268. [DOI] [PubMed] [Google Scholar]
- 26.Roehrborn CG, Van Kerrebroeck P, Nordling J. Safety and efficacy of alfuzosin 10 mg once-daily in the treatment of lower urinary tract symptoms and clinical benign prostatic hyperplasia: a pooled analysis of three double-blind, placebo-controlled studies. BJU Int. 2003;92:257–261. doi: 10.1046/j.1464-410x.2003.04309.x. [DOI] [PubMed] [Google Scholar]
- 27.Yoshimura K, Ohara H, Ichioka K. Nocturia and benign prostatic hyperplasia. Urology. 2003;61:786–790. doi: 10.1016/s0090-4295(02)02444-5. [DOI] [PubMed] [Google Scholar]
- 28.Miwa K, Nishino Y, Kikuchi M. Efficacy of combination therapy with tamsulosin and zolpidem on nocturia in patients with benign prostatic hyperplasia. Cent European J Urol. 2011;64:232–235. doi: 10.5173/ceju.2011.04.art9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kaplan SA, Roehrborn CG, Rovner ES. Tolterodine and tamsulosin for treatment of men with lower urinary tract symptoms and overactive bladder: a randomized controlled trial. JAMA. 2006;296:2319–2328. doi: 10.1001/jama.296.19.2319. [DOI] [PubMed] [Google Scholar]
- 30.Margel D, Lifshitz D, Brown N. Predictors of nocturia quality of life before and shortly after prostatectomy. Urology. 2007;70:493–497. doi: 10.1016/j.urology.2007.05.001. [DOI] [PubMed] [Google Scholar]
- 31.Simaioforidis V, Papatsoris AG, Chrisofos M. Tamsulosin versus transurethral resection of the prostate: effect on nocturia as a result of benign prostatic hyperplasia. Int J Urol. 2011;18:243–248. doi: 10.1111/j.1442-2042.2010.02704.x. [DOI] [PubMed] [Google Scholar]
- 32.Reynard JM, Cannon A, Yang Q. A novel therapy for nocturnal polyuria: a double-blind randomized trial of frusemide against placebo. Br J Urol. 1998;81:215–218. doi: 10.1046/j.1464-410x.1998.00511.x. [DOI] [PubMed] [Google Scholar]
- 33.Drake MJ, Mills IW, Noble JG. Melatonin pharmacotherapy for nocturia in men with benign prostatic enlargement. J Urol. 2004;171:1199–1202. doi: 10.1097/01.ju.0000110442.47593.ea. [DOI] [PubMed] [Google Scholar]
- 34. NOCDURNA® sublingual wafer Product information. http://www.medicines.org.au/files/fppnocdw.pdf. Accessed March 14, 2018.
- 35. MINIRIN® (desmopressin) Media Backgrounder. ferring.ca/Umbraco/Api/WebApi/GetMediaFile/478. Accessed March 14, 2018.
- 36.Chancellor MB, Atan A, Rivas DA. Beneficial effect of intranasal desmopressin for men with benign prostatic hyperplasia and nocturia: preliminary results. Tech Urol. 1999;5:191–194. [PubMed] [Google Scholar]
- 37. NOCTIVA (desmopressin acetate) nasal spray. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/201656lbl.pdf. Accessed March 14, 2018.
- 38. Serenity Pharmaceuticals, LLC SER120 Nasal Spray Advisory Committee Briefing Document: Bone, Reproductive and Urologic Drugs Advisory Committee. https://www.fda.gov/downloads/AdvisoryCommittees/ CommitteesMeetingMaterials/Drugs/Reproductive HealthDrugsAdvisoryCommittee/UCM525331.pdf. Created October 19, 2016. Accessed March 14, 2018.
- 39.Blaivas JG, Dmochowski RR, Kaminetsky J. My CME website. https://central.arraylearn .com/arraylearn/pdf?q=eyJlbWFpbCI6Impvc2h1YW NvaG5AZ21haWwuY29tIiwiYWN0aXZpdHlfaWQi OiIxNjM5IiwibW9kZWwiOiJcXEVtYWlsXFxOb3Rl In0=&filename=notepdf. Accessed March 14. 2018. Nocturia: casting light on an underrecognized and undertreated LUTS. [Google Scholar]
- 40.Cohn JA, Kowalik CG, Reynolds WS. Desmopressin acetate nasal spray for adults with nocturia. Expert Rev Clin Pharmacol. 2017;10:1281–1293. doi: 10.1080/17512433.2017.1394185. [DOI] [PubMed] [Google Scholar]
- 41. Efficacy study of fedovapagon for nocturia in men with benign prostatic hyperplasia ( NCT02637960). US National Library of Medicine website. https:// clinicaltrials.gov/ct2/show/ NCT02637960. Accessed March 14, 2018.
- 42. Trial of SK-1404 for nocturia due to nocturnal polyuria in Japanese subjects ( NCT03116191). US National Library of Medicine website. https://clinicaltrials.gov/ct2/ show/ NCT03116191. Accessed March 14, 2018.
- 43.Van Kerrebroeck P. Standardization of terminology in nocturia: commentary on the ICS report. BJU Int. 2002;90:16–17. doi: 10.1046/j.1464-410x.90.s3.4.x. [DOI] [PubMed] [Google Scholar]
- 44.Weiss JP, Blaivas JG, Stember DS. Evaluation of the etiology of nocturia in men: the nocturia and nocturnal bladder capacity indices. Neurourol Urodyn. 1999;18:559–565. doi: 10.1002/(sici)1520-6777(1999)18:6<559::aid-nau6>3.0.co;2-d. [DOI] [PubMed] [Google Scholar]
- 45.Lose G, Lalos O, Freeman RM, van Kerrebroeck P. Efficacy of desmopressin (Minirin) in the treatment of nocturia: a double-blind placebo-controlled study in women. Am J Obstet Gynecol. 2003;189:1106–1113. doi: 10.1067/s0002-9378(03)00593-3. [DOI] [PubMed] [Google Scholar]
- 46.Mattiasson A, Abrams P, van Kerrebroeck P. Efficacy of desmopressin (Minirin) in the treatment of nocturia: a double-blind, placebo-controlled study in men. BJU Int. 2002;89:855–862. doi: 10.1046/j.1464-410x.2002.02791.x. [DOI] [PubMed] [Google Scholar]
- 47. FDA advisers reject desmopressin fo rnocturia. Medscape website. www.medscape.com/viewarticle/838078. Posted January 12, 2015 Accessed March 30, 2018.