

Abstract
Background
Bipolar disorder (BD), a type of psychiatric mood disorder, is manifested by chronic and recurrent mood fluctuations. This study aims to determine whether hepatitis B virus (HBV) or hepatitis C virus (HCV) infection is a risk factor for BD.
Methods
A total of 48,215 patients with newly diagnosed viral hepatitis from 2000 to 2010 were identified and frequency-matched with 192,860 people without hepatitis. Both groups were followed until diagnosis with BD, withdrawal from the national health insurance program, or the end of 2011. Patients with viral hepatitis were grouped into 3 cohorts: HBV infection, HCV infection, and HBV/HCV coinfection. The association between viral hepatitis and BD were examined using Cox proportional hazards regression models.
Results
The incidence of BD was higher in HBV/HCV coinfection than in the control group, with an adjusted hazard ratio of 2.16 (95% confidence interval 1.06–4.41) when adjusted for sex, age, and comorbidity. After further adjustment, we noted that an age more than 65 years and female may be associated with an increased risk of BD in patients with chronic hepatitis B and C.
Conclusion
Viral hepatitis may be associated with increased risk of subsequent BD.
Electronic supplementary material
The online version of this article (10.1186/s12967-018-1542-3) contains supplementary material, which is available to authorized users.
Keywords: HBV, HCV, Bipolar disorder, NHIRD
Background
Viral hepatitis is the major cause of hepatitis [1]. Among all types of viral hepatitis, hepatitis B virus (HBV) and hepatitis C virus (HCV) entail infections that are known for engendering chronic liver inflammation and hepatic malignancy [2]. In addition to HBV or HCV monoinfection, HBV/HCV coinfection has been shown to be associated with an increased risk of disease progression and malignancy [3]. Moreover, it has been reported that hepatic inflammation plays a major role in HBV- or HCV-induced liver damage, and immune cells including CD8(+)T lymphocytes as well as proinflammatory cytokines are also involved in this damage [4]. Although hepatic inflammation is a symptom of HBV and HCV infection, the inflammatory response could be systemic, because of the immune reaction induced by the translocation of microbial products. [5]. Research has shown that HBV can replicate in neuronal cells, which may account for the neuropathy associated HBV infection [6]. Furthermore, HCV-infected microglia cells and astrocyte are detected in the brain, indicating biological basis of neurocognitive abnormalities in HCV infection [7]. Recently, four independent studies indicate that viral hepatitis is associated with subsequent Parkinson disease [8–11]. These papers raised a specific aspect of viral hepatitis, but whether this reflects shared disease mechanisms in genetic or environmental susceptibility, or sequelae of viral hepatitis per se, or a consequence of treatment remains to be determined. It is of great interest to note that the association between viral hepatitis and psychiatric diseases has not been explored yet. We therefore aimed to investigate the association between viral hepatitis and bipolar disorder.
Bipolar disorder (BD), a type of psychiatric mood disorder, is manifested by chronic and recurrent mood fluctuations and involves a spectrum of symptoms including depressive, hypomanic, and manic manifestations [12]. In the BD population, all-cause and suicide mortality rates are substantially approximately 2-fold and 10-fold higher, respectively, than those in the general population [13]. Osby et al. further reported that the increased death rate in patients with BD is partly attributable to various potentially life-threatening medical comorbidities, particularly cardiovascular diseases [14]. In a review of the evidence, Rege and Hopkinson suggest that systemic inflammation and neuroinflammation may be involved in the pathogenesis of BD [15]. Inflammatory cytokines such as tumor necrosis factor-α (TNF-α) and soluble tumor necrosis factor receptor type 1 have been reported to be involved in the inflammatory state [16]. Another hypothesis of the association between medical conditions and subsequent BD was through inflammatory process, such as rheumatoid arthritis [17], peptic ulcer disease [18], and gastro-esophageal reflux disease [19]. As there is a high prevalence of HBV or HCV infection in Taiwan, we are therefore interested in investigating whether chronic HBV or HCV infection is a risk factor for the development of BD.
In treatment of hepatitis, interferon-α, one of the treatment of HBV and HCV, was reported having neuropsychiatric side-effects [20]. Also, in the treatment of chronic HCV infection, combination of interferon and ribavirin was reported having psychiatric adverse events, including major depression [21]. Additionally, a study conducted by Quarantini and colleagues demonstrated that patients with HCV infection exhibit cognitive impairment, especially over visuo-spatial memory performance, which may be specific to HCV infection rather than secondary psychiatric comorbidities [22]. Even though a case report demonstrated interferon therapy could induce mania [23], limited evidence investigated the association between HBV/HCV and subsequent BD. To test these hypothesis that HBV or HCV infection is associated with subsequent BD, we conducted a nationwide, population-based cohort study to investigate whether HBV or HCV infection increases the risk of BD.
Methods
Data source
The study was conducted using data from the Longitudinal Health Insurance Database (LHID), a data set comprising the claims data of people enrolled in the Taiwan National Health Insurance (NHI) program. The National Health Research Institutes (NHRI) randomly selected 1 million insured people from 1996 to 2000 and followed them. According to the NHRI report, the demographic characteristics showed no difference between the people in the LHID and those enrolled in the NHI program. The claims data in the LHID include a beneficiary registry, inpatient and outpatient files, and other medical services. All patient histories were collected from inpatient and outpatient files and recorded according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). The NHRI released the database with anonymous patient identification numbers to protect the privacy of the insured people.
Study population
This was a retrospective, population-based cohort study, and we included a cohort of hepatitis patients and a comparison cohort to observe the occurrence of BD. The hepatitis cohort comprised patients with new onset HBV (ICD-9-CM 070.20 Viral hepatitis B with hepatic coma, acute or unspecified, without mention of hepatitis delta; 070.22 Viral hepatitis B with hepatic coma, chronic, without mention of hepatitis delta; 070.30 Viral hepatitis B without mention of hepatic coma, acute or unspecified, without mention of hepatitis delta; 070.32 Viral hepatitis B without mention of hepatic coma, chronic, without mention of hepatitis delta, and V02.61 Hepatitis B carrier) or HCV (ICD-9-CM 070.41 Acute hepatitis C with hepatic coma; 070.44 Chronic hepatitis C with hepatic coma; 070.51 Acute hepatitis C without mention of hepatic coma; 070.54 Chronic hepatitis C without mention of hepatic coma, and V02.62 Hepatitis B carrier) from January 1, 2000 to December 31, 2010. The date of first diagnosis of hepatitis was defined as the index date. The comparison cohort contained patients in the LHID without a diagnosis of hepatitis. Each patient in the hepatitis cohort was randomly frequency-matched with 4 controls according to various criteria including age (per 5 years) and sex. For the index date of the comparison cohort, patients were assigned the same date as those of the matched cases. Both cohorts excluded patients without complete characteristic data and aged younger than 20 years or those with a history of BD before the index date. In addition, considering the undiagnosed mood symptoms, we also excluded the patients having depression (ICD-9-CM 296.2 Major depressive disorder, single episode; 296.3 Major depressive disorder, recurrent episode; 311 Depressive disorder, not elsewhere classified) before the index date. Moreover, HBV/HCV can be contracted during sex [24] and unsafe drug use [25]. Hence, before the index date, we excluded patients having the diagnosis of borderline personality disorder (ICD-9-CM 301.83 Borderline personality disorder), which has been associated with risky sexual behaviors (no using condoms with changed partners) and substance use problems [26], and we also excluded the patients having opioid dependence (ICD-9-CM 305.5 opioid abuse; 304.0 opioid type dependence). It has been suggested that the exclusion of these patients could decrease the selection bias. We followed these 2 cohorts until withdrawal from the insurance program, BD occurrence (ICD-9-CM 296 Episodic mood disorders), or December 31, 2011. The confounding factors in this study were age, sex, and BD-associated comorbidities. Sex difference was noted among hepatitis infection and may influence the outcome [27]. Patients with comorbidities were defined as those with a history of comorbidities before the index date. The BD-associated comorbidities in this study included cirrhosis (ICD-9-CM 571.2 571.2 Alcoholic cirrhosis of liver; 571.5 Cirrhosis of liver without mention of alcohol; 571.6 Biliary cirrhosis), hypertension (ICD-9-CM 401-405 Hypertensive disease), hyperlipidemia (ICD-9-CM 272 Disorders of lipoid metabolism), asthma (ICD-9-CM 493 Asthma), coronary artery disease (CAD, ICD-9-CM 410-414 Ischemic heart disease), alcohol-related disorder (ALD, ICD-9-CM 291 Alcohol-induced mental disorders; 303 Alcohol dependence syndrome; 305.0 Alcohol abuse; 571.0 Alcoholic fatty liver; 571.1 Acute alcoholic hepatitis; 571.3 Alcoholic liver damage, unspecified; 790.3 Excessive blood level of alcohol; A215, and V11.3 Alcoholism), anxiety [28] (ICD-9-CM 300.00 Anxiety state, unspecified). Additionally, we listed major depressive disorder (ICD-9-CM 296.20 Major depressive disorder, single episode; 296.30 Major depressive disorder, recurrent episode; 311 Depressive disorder, not elsewhere classified) for further adjustment because there were overlapping symptoms between unipolar depression and bipolar depression [29].
Statistical analyses
In this study, the demographic characteristics and medical records in LHID included continuous data (such as age) and binary variables (such as sex, treatment status and comorbidity). They were all in reasonable range. The characteristics of the study population, which were represented by their age, sex, and comorbidities, were described using mean and percentage values. To examine the difference between the hepatitis and comparison cohorts, we used a t test to analyze age and a Chi square test to analyze sex and comorbidities. Furthermore, we calculated the incidence density of subsequent BD in both cohorts. The cumulative incidence curves for the 2 cohorts were evaluated using the Kaplan–Meier method. The log-rank test was used to test the difference between the incidence curves. To measure the risk of BD in the hepatitis cohort compared with the comparison cohort, we transformed all categorical variables into dummy variables and evaluated crude and adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) by using Cox proportional hazard models. We also analyzed the risk of BD stratified by age, sex, and comorbidities. We used SAS Version 9.4 software (SAS Institute, Cary, NC, USA) to manage the data and conduct the statistical analyses. The incidence curves were plotted using R software (R Foundation for Statistical computing, Vienna, Austria). A 2-sided p < .05 reached the level of significance.
Results
We selected a total of 48,215 patients with hepatitis in this study. As shown in Table 1, the types of hepatitis were HBV infection (71.5%), HCV infection (20.5%), and HBV/HCV coinfection (8.0%). The mean age of the hepatitis and comparison cohorts was approximately 46 years (SD: 15), and the male patients constituted the highest proportion (57.1%) of the patients in these cohorts. The proportions of comorbidities in the hepatitis cohort were significantly greater than those in the comparison cohort (all p < .001) (Table 1).
Table 1.
Distribution of age, gender, and comorbidity between hepatitis infection and comparison cohort
| Hepatitis infection | Comparison N = 192,860 | p value† | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (n = 48,215) | HBV (n = 34,459, 71.5%) | HCV (n = 9893, 20.5%) | Both (n = 3863, 8.0%) | ||||||||
| N | % | N | % | N | % | N | % | N | % | ||
| Age, year | 0.99 | ||||||||||
| 20–34 | 12,799 | 26.6 | 11,028 | 32.0 | 1121 | 11.3 | 650 | 16.8 | 51,196 | 26.6 | |
| 35–49 | 16,568 | 34.4 | 13,023 | 37.8 | 2347 | 23.7 | 1198 | 31.0 | 66,272 | 34.4 | |
| 50–64 | 12,013 | 24.9 | 7447 | 21.6 | 3319 | 33.6 | 1247 | 32.3 | 48,052 | 24.9 | |
| 65+ | 6835 | 14.2 | 2961 | 8.59 | 3106 | 31.4 | 768 | 19.9 | 27,340 | 14.2 | |
| Mean (SD) | 46.5 | (15.4) | 43.4 | (14.2) | 55.8 | (15.6) | 51.0 | (15.0) | 46.3 | (15.8) | 0.001 |
| Gender | 0.99 | ||||||||||
| Women | 20,699 | 42.9 | 14,134 | 41.0 | 4863 | 49.2 | 1702 | 44.1 | 82,796 | 42.9 | |
| Men | 27,516 | 57.1 | 20,325 | 59.0 | 5030 | 50.8 | 2161 | 55.9 | 110,064 | 57.1 | |
| Comorbidity | |||||||||||
| Cirrhosis | 28,450 | 59.0 | 18,803 | 54.6 | 6905 | 69.8 | 2742 | 71.0 | 23,111 | 12.0 | < 0.001 |
| Hypertension | 12,542 | 26.0 | 6876 | 20.0 | 4331 | 43.8 | 1335 | 34.6 | 41,379 | 21.5 | < 0.001 |
| Hyperlipidemia | 9671 | 20.1 | 6276 | 18.2 | 2501 | 25.3 | 894 | 23.1 | 27,681 | 14.4 | < 0.001 |
| Asthma | 3026 | 6.28 | 1800 | 5.22 | 926 | 9.36 | 300 | 7.77 | 9114 | 4.73 | < 0.001 |
| CAD | 6016 | 12.5 | 3107 | 9.02 | 2253 | 22.8 | 656 | 17.0 | 18,875 | 9.79 | < 0.001 |
| ALD | 3216 | 6.67 | 1956 | 5.68 | 926 | 9.36 | 334 | 8.65 | 5304 | 2.75 | < 0.001 |
| Anxiety | 3400 | 7.05 | 2081 | 6.04 | 976 | 9.87 | 343 | 8.88 | 8407 | 4.36 | < 0.001 |
| MDD | 1615 | 3.35 | 967 | 2.81 | 464 | 4.69 | 184 | 4.76 | 3917 | 2.03 | < 0.001 |
Chi square test
CAD coronary artery disease, ALD alcohol-related disorder, MDD major depressive disorders, SD standard deviation
†Total hepatitis infection versus comparison
We observed 136 and 58 BD occurrences in the comparison and hepatitis cohorts, respectively (Table 2). The incidence of BD in the comparison cohort was 1.14 per 10,000 person-years, whereas that in the hepatitis cohort was 2.04 per 10,000 person-years. Moreover, the incidence rates of BD were 1.79, 2.23, and 3.62 per 10,000 person-years in the HBV, HCV, and coinfection groups, respectively (Table 2). Figure 1 shows that the incidence curves for BD in the hepatitis cohort were significantly higher than those in the comparison cohort (log-rank test p < .001). After adjustment for BD-associated risk factors, patients with coinfection of HBV and HCV exhibited a significantly increased risk of BD compared with those in the comparison group (adjusted HR 2.16, 95% CI 1.06–4.41; p < .001) (Table 2). The results revealed a significantly higher risk for BD inpatients younger than 65 years old, female patients, and patients with the comorbidities of anxiety and major depressive disorder. We noted significantly lower risk for subsequent BD was the comorbidity of hyperlipidemia. In addition, we noted a study, conducted by Ayano et al. [27], showing sex difference among hepatitis infection, and having influence on the outcome. Hence, sex was a confounding factor in our study and we adjusted it in our study.
Table 2.
Estimation of bipolar Incidence and hazard ratio by Cox proportional hazard models
| Event no | PY | % | HR (95% CI) | ||
|---|---|---|---|---|---|
| Crude | Adjusted | ||||
| Hepatitis infection | |||||
| None | 136 | 1,188,037 | 1.14 | 1.00 | 1.00 |
| All | 58 | 284,895 | 2.04 | 1.78 (1.31, 2.41)*** | 1.38 (0.96, 1.98) |
| HBV | 37 | 206,332 | 1.79 | 1.56 (1.09, 2.25)* | 1.27 (0.85, 1.90) |
| HCV | 12 | 53,706 | 2.23 | 1.93 (1.07, 3.48)* | 1.38 (0.73, 2.60) |
| Both | 9 | 24,857 | 3.62 | 3.22 (1.64, 6.32)*** | 2.16 (1.06, 4.41)* |
| Age, year | |||||
| 20–49 | 125 | 951,575 | 1.31 | 1.85 (1.04, 3.27)* | 2.54 (1.34, 4.82)** |
| 50–64 | 56 | 346,885 | 1.61 | 2.22 (1.21, 4.06)** | 2.51 (1.35, 4.67)** |
| 65+ | 13 | 174,472 | 0.75 | 1.00 | 1.00 |
| Gender | |||||
| Women | 104 | 635,836 | 1.64 | 1.53 (1.15, 2.02)** | 1.37 (1.03, 1.83)* |
| Men | 90 | 837,096 | 1.08 | 1.00 | 1.00 |
| Comorbidity | |||||
| Cirrhosis | |||||
| No | 135 | 1,168,092 | 1.16 | 1.00 | 1.00 |
| Yes | 59 | 304,840 | 1.94 | 1.66 (1.22, 2.26)** | 1.23 (0.84, 1.80) |
| Hypertension | |||||
| No | 151 | 1,177,342 | 1.28 | 1.00 | 1.00 |
| Yes | 43 | 295,590 | 1.45 | 1.10 (0.79, 1.55) | 1.05 (0.69,1 .60) |
| Hyperlipidemia | |||||
| No | 171 | 1,265,096 | 1.35 | 1.00 | 1.00 |
| Yes | 23 | 207,837 | 1.11 | 0.80 (0.52, 1.23) | 0.54 (0.33, 0.87)* |
| Asthma | |||||
| No | 181 | 1,410,513 | 1.28 | 1.00 | 1.00 |
| Yes | 13 | 62,419 | 2.08 | 1.55 (0.88, 2.72) | 1.24 (0.69, 2.22) |
| CAD | |||||
| No | 170 | 1,337,581 | 1.27 | 1.00 | 1.00 |
| Yes | 24 | 135,352 | 1.77 | 1.36 (0.89, 2.08) | 1.13 (0.68, 1.88) |
| ALD | |||||
| No | 185 | 1,434,621 | 1.29 | 1.00 | 1.00 |
| Yes | 9 | 38,311 | 2.35 | 1.71 (0.87, 3.34) | 1.11 (0.56, 2.21) |
| Anxiety | |||||
| No | 165 | 1,415,652 | 1.17 | 1.00 | 1.00 |
| Yes | 29 | 57,280 | 5.06 | 4.08 (2.75, 6.06)*** | 1.80 (1.15, 2.83)* |
| Major depressive disorders | |||||
| No | 147 | 1,445,019 | 1.02 | 1.00 | 1.00 |
| Yes | 47 | 27,913 | 16.8 | 15.8 (11.4, 22.0)*** | 12.9 (8.85, 18.7)*** |
Multivariable analysis including age, sex, and comorbidities of cirrhosis, hypertension, hyperlipidemia, asthma, CAD, ALD, anxiety and major depressive disorders
PY person-years, % Rate, per 10,000 person-years, CAD coronary artery disease, ALD alcohol-related disorder
* p < 0.05, ** p < 0.01, *** p < 0.001
Fig. 1.
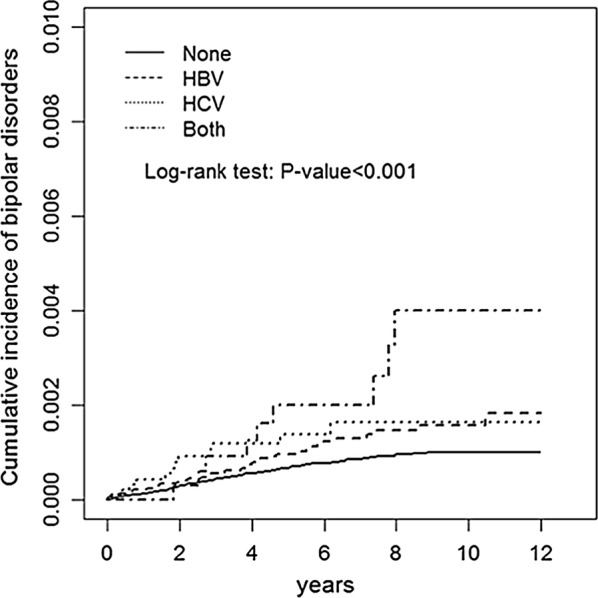
Cumulative incidence of bipolar disorders in patients with different hepatitis infection
Table 3 presents the risk for BD stratified by age, sex, comorbidity, and types of hepatitis. Comparing the hepatitis cohort with the comparison cohort revealed that the HRs of BD significantly increased in patients aged more than 65 years (HR 4.49, 95% CI 1.25–16.2). Compared with the control group, a significantly increased risk for BD was observed in the female (HR 1.70, 95% CI 1.06–2.75) patients in the hepatitis group. In the HBV group, an increased risk of subsequent BD was noted among female patients (HR 1.87, 95% CI 1.13–3.10). In the HCV group, no association with the increased risk of subsequent BD was shown regardless of age, gender, and comorbidity. In both the HBV and HCV groups, an increased risk of subsequent BD was noted among patients aged more than 65 years (HR 16.3, 95% CI 2.83–93.5), and patients having any comorbidity (HR 2.28, 95% CI 1.09–4.76). In Table 2, crude HRs were the results of simple Cox regression, and adjusted HRs were the results of multiple Cox regression with fully adjustment. Table 3 shows the results of stratified analysis. We stratified by sub groups of each covariate, and calculated the HRs. Table 3 shows the results of stratified analysis. We stratified by sub groups of each covariate, and calculated the HRs. We have further modified Table 3. The adjusted HRs in total subjects (n = 48,215), HBV (n = 34,459), HCV (n = 9893) and Both HBV/HCV (n = 3863) compared with Comparison group (n = 192,860).
Table 3.
Incidence and hazard ratio for bipolar disorders stratified by age, gender and comorbidity
| Comparison N = 192,860 |
Hepatitis infection | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (n = 48,215) | HBV (n = 34,459) | HCV (n = 9893) | Both (n = 3863) | |||||||||||
| Event no | % | Event no | % | HR† (95% CI) | Event no | % | HR† (95% CI) | Event no | % | HR† (95% CI) | Event no | % | HR† (95% CI) | |
| Age, year | ||||||||||||||
| 20–49 | 87 | 1.14 | 38 | 2.01 | 1.35 (0.86, 2.11) | 28 | 1.81 | 1.30 (0.80, 2.10) | 5 | 2.28 | 1.17 (0.45, 3.03) | 5 | 3.83 | 2.19 (0.85, 5.62) |
| 50–64 | 41 | 1.45 | 15 | 2.30 | 1.04 (0.53, 2.05) | 8 | 2.05 | 0.98 (0.43, 2.21) | 5 | 2.72 | 1.19 (0.44, 3.21) | 2 | 2.58 | 1.02 (0.24, 4.46) |
| 65+ | 8 | 0.56 | 5 | 1.64 | 4.49 (1.25, 16.2)* | 1 | 0.77 | 2.12 (0.25, 17.7) | 2 | 1.49 | 4.58 (0.83, 25.4) | 2 | 4.95 | 16.3 (2.83, 93.5)** |
| Gender | ||||||||||||||
| Women | 73 | 1.43 | 31 | 2.49 | 1.70 (1.06, 2.75)* | 24 | 2.80 | 1.87 (1.13, 3.10)* | 4 | 1.47 | 1.02 (0.35, 2.92) | 3 | 2.63 | 1.80 (0.54, 5.94) |
| Men | 63 | 0.93 | 27 | 1.68 | 1.09 (0.65, 1.85) | 13 | 1.08 | 0.76 (0.39, 1.46) | 8 | 3.02 | 1.71 (0.77, 3.79) | 6 | 4.46 | 2.42 (0.99, 5.96) |
| Comorbidity | ||||||||||||||
| None | 69 | 0.88 | 13 | 1.62 | 1.74 (0.96, 3.15) | 11 | 1.63 | 1.74 (0.92, 3.31) | 1 | 1.22 | 1.29 (0.18, 9.30) | 1 | 2.38 | 2.54 (0.35, 18.3) |
| With any one | 67 | 1.66 | 45 | 2.20 | 1.19 (0.81, 1.76) | 26 | 1.87 | 0.95 (0.59, 1.52) | 11 | 2.42 | 1.46 (0.77, 2.77) | 8 | 3.87 | 2.28 (1.09, 4.76)* |
%: Rate, per 10,000 person-years
* p < 0.05, ** p < 0.01, *** p < 0.001
† Multivariable analysis including age, sex, and comorbidities of cirrhosis, hypertension, hyperlipidemia, asthma, coronary artery disease, alcohol-related illness, anxiety, and major depressive disorders
In Table 4, we demonstrated the association between antiviral drugs for hepatitis and the incidence of BD, revealing no association between antiviral drugs and increased risk of subsequent BD. We demonstrated the association between antiviral drugs for hepatitis and the incidence of BD, revealing no association between antiviral drugs and increased risk of subsequent BD. In Table 3, it shows incidence, and hazard ratio of bipolar disorders between patients with hepatitis infection with and without treatment (with propensity score matching). Table 4 shows estimation of bipolar hazard ratio by simple and multiple Cox proportional hazard models (with propensity score matching).
Table 4.
Incidence, and hazard ratio of bipolar disorders between patients with hepatitis infection with and without treatment
| Variables | N | Event | PY | % | Crude HR (95% CI) | Adjusted HR† (95% CI) |
|---|---|---|---|---|---|---|
| Hepatitis infection | ||||||
| Without treatment | 44,461 | 54 | 262,819 | 2.05 | 1.00 | 1.00 |
| Only HBV treatment | ||||||
| Lamivudine, telbivudine, adefovir, tenofovir, and entecavir | 2151 | 2 | 11,820 | 1.69 | 0.82 (0.20, 3.36) | 0.85 (0.21, 3.53) |
| Only HCV treatment | ||||||
| Ribavirin, interferon | 1081 | 2 | 6623 | 3.02 | 1.48 (0.36, 6.05) | 1.29 (0.31, 5.37) |
| Both HBV&HCV treatment | 522 | 0 | 3634 | 0.00 | – | – |
PY Person-years, % rate, per 10,000 person-years
† Multivariable analysis including age, sex, and comorbidities of cirrhosis, hypertension, hyperlipidemia, asthma, coronary artery disease, alcohol-related illness, anxiety, and major depressive disorders
Discussion
Key findings
In this study, we demonstrated that HBV or HCV infection may be associated with subsequent BD, and, to the best of our knowledge, we demonstrated their correlation for the first time by using a matched population-based cohort and 10-year follow-up period. The major findings of our study suggest a higher incidence of subsequent BD among patients with HBV/HCV coinfection. Also, we demonstrated the comorbidities related to the subsequent occurrence of BD, including hyperlipidemia, anxiety, and major depressive disorder. Anxiety was frequently comorbid with BD [28]. Patients with major depression may have unrecognized BD [30], and depressive symptoms were noted among the course of BD [31]. On the other hand, evidence showed patients with chronic hepatitis B and C had psychosocially impaired their mental health and daily life [32]. As a result, those conditions were associated with subsequent occurrence of BD. In addition, we noted hyperlipidemia had decreased risk for subsequent BD. We considered this may be associated with selection bias in our study. Mood stabilizer and atypical antipsychotics were used for the treatment of BD [33]. The metabolic syndrome, including hyperlipidemia, was reported as the adverse effect of the treatment [34]. As a result, patients with BD under those drugs treatment may have improved clinical condition but have the adverse effect of hyperlipidemia.
We noted that female patient with HBV infection was associated with the subsequent occurrence of BD. To the best of our knowledge, we hypothesized that the mechanism was possibly related to the interaction between sex hormone and the disease activity of HBV infection. Evidence shows that HBV infection is characterized by its lifelong persistence and inflammation [35]. In addition, acute liver failure (ALF) was noted to be among the courses of chronic liver inflammation [36]. Moreover, proinflammatory cytokines such as TNF-α may affect the brain by impairing the permeability of the blood brain barrier and neuroinflammation, particularly under the condition of ALF [37, 38]. In addition, studies have revealed that inflammation in the brain was associated with developing mood disorders, including BD, and that TNF-α was a critical cytokine in pathophysiology [39–41]. On the other hand, one study showed that sex hormones were associated with the disease activity of HBV infections [42]. Although estrogen was reported to have a protective effect on the progression of HBV infection [43], estrogen receptor gene polymorphisms in a Chinese population may be associated with occurrences of ALF [44]. As a result, female patients with HBV demonstrate an increased risk of subsequent BD.
It has been shown elsewhere that the anti-HCV treatment (ribavirin and interferon) are related to the development of depression [21]. In our study, we demonstrated the association between HBV/HCV and subsequent BD. When we further control the effects of anti-viral treatments to HBV or HCV infections (anti-HBV treatment: lamivudine, telbivudine, adefovir, tenofovir, and entecavir or anti-HCV treatment: ribavirin, interferon), we found no association between HBV or HCV treatment and increased risk of subsequent BD (Table 4). Hence, we considered the association between HBV/HCV and subsequent BD may be attributed to the HBV/HCV infection/inflammation itself rather than the effect of treatment. However, future mechanistic studies are warranted.
In addition, our statistically matched study, including age, gender, and comorbidity, demonstrated increased risk of subsequent BD in patients having concurrent HBV and HCV infections. Our results reveal that this condition was associated with patients aged more than 65 years and having any comorbidity. HBV and HCV have been reported to be associated with CNS involvement through neuroinflammation [37, 45]. HBV/HCV coinfection is prone to involve more advanced and progressive liver damage than does monoinfection [46]. Although treatment for HCV dominance in HBV/HCV coinfection can achieve HCV clearance, HBV reactivation has been noted [3, 47]. The reactivation of HBV could induce immune-mediated inflammatory reactions [48, 49], which are superimposed with the underlying chronic inflammation associated with HBV and HCV conditions. Hence, the inflammatory process was augmented, consequently increasing the risk of BD. In addition, the aforementioned studies have indicated that the ALF of HBV infection could impair the integrity of the blood–brain barrier [37, 38], and HCV could infect brain endothelial cells [50], induce microglial activation [51], and adversely interact with brain astrocytes [52]. We suppose that the adverse influence of HBV and HCV cause the brain to be more vulnerable to neuroinflammation and HCV replication. Hence, the risk of BD increased more in HBV/HCV coinfection than in HBV or HCV infection. On the other hand, studies had shown the association between aging and neuroinflammation [53], and we considered this condition may make elder patients with HBV/HCV coinfection more vulnerable to subsequent BD [54]. Hence, we suppose that in patients with HBV/HCV coinfection, those aged more than 65 years may raise further concern about the increased risk of subsequent BD. Moreover, HCV was reported having comorbidities involving in systemic inflammation [55, 56] and may therefore increase the risk of subsequent BD.
Limitations
To the best of our knowledge, this is the first population-based study designed to investigate the association between viral hepatitis and BD. We employed a matched case–control design and a population-based cohort of patients with viral hepatitis and adequate controls as well as a sufficient number of comorbidities, thus further strengthening the study. However, limitations inherent to the use of claims databases were encountered. First, the diagnosis of hepatitis in the NHIRD was based on ICD-9-CM codes; therefore, the severity of hepatitis as a risk factor for developing BD was not explored. Also, we mark the temporal association by the chronological order, so we could not confirm the effect or the causal relationship between hepatitis infection and BD. Additionally, considering the possibility of reactivation, we included hepatitis carrier, ICD-9-CM codes of V02.61 and V02.62, in our study, and this management could affect the result revealed in our study. Nevertheless, in our study design, we conducted a 10-year follow-up to observe the long-term influence of HBV or HCV infection on the subsequent development of BD. Second, the association was evaluated according to the chronological order in which these two diseases were diagnosed. Whether the patients previously had BD-related symptoms without being diagnosed with BD was unknown. Third, information on numerous demographic variables, including socioeconomic status and family history, was unavailable; such information may provide useful data regarding factors associated with viral hepatitis and BD. Forth, BD was reported having early presentation in lifetime prevalence [57]. Excluding patients younger than 20 years old in this study may limit the application. However, studies had shown that attention deficit hyperactivity disorder was often comorbid and easily confused with BD in younger age [58]. Therefore, our study used more than 20 years old instead and demonstrated on the long-term relationship between HBV/HCV and BD. Furthermore, some immune-related diseases, such as rheumatoid arthritis [17], were reported having association with subsequent BD. Hence, those diseases could be confounding factors. On the other hand, exclusion of depression and anxiety may have influence on the diagnosis of BD, and therefore influence the generalizability of our study. Forth, although our study sample comprised an adequate number of patients in the HBV/HCV and control groups as well as an adequate number of comorbidities, our findings were demonstrated only in this studied population; we could not validate the generalizability of the results to other populations. Finally, although we also provided the propensity score matching for hepatitis versus no-hepatitis patients (Additional file 1: Tables S1 and S2), there is no significance for the casual relationship of viral hepatitis and BDs, it may be due to the reason that if we deliberately adjust the control cohort for hypertension, hyperlipidemia, asthma, CAD, ALD, anxiety and MDD, then we may overlook the true risk for BDs in HBV, HCV or HBV/HCV patients, because the new control cohort consists of subjects with relatively higher risk. Due to the association between viral hepatitis and BDs, and the significant role of neuronal dysfunction are strongly suggested in BDs, we also plan to confirm the causal relationship of viral hepatitis and BDs, and the underlying mechanisms by using the human induced pluripotent stem cells from HBV/HCV patients and differentiated the neurons that are responsible for the phenotype of BD [59].
Conclusions
The findings suggest that HBV/HCV infection may be associated with increased risk of subsequent BD. Additional prospective clinical and basic studies on the relationship between hepatitis and BD are warranted.
Additional file
Additional file 1: Table S1. Distribution of age, gender, and comorbidity between hepatitis infection and comparison cohort with propensity score matching. Table S2. Estimation of bipolar Incidence and hazard ratio by Cox proportional hazard models with propensity score matching.
Authors’ contributions
Conception/Design: YCH; Provision of study materials: KHC, YCH; Collection and/or assembly of data: all authors; Data analysis and interpretation: all authors; Manuscript writing: LWC, YCH. All authors read and approved the final manuscript.
Acknowledgements
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
Data are available from the NHIRD published by Taiwan National Health Insurance Bureau. Due to legal restrictions imposed by the Government of Taiwan in relation to the ‘Personal Information Protection Act’, data cannot be made publicly available. Requests for data can be sent as a formal proposal to the NHIRD (http://nhird.nhri.org.tw).
Consent for publication
Not applicable.
Ethics approval and consent to participate
This article does not contain any studies with human participants or animals performed by any of the authors. The NHIRD contains only encrypted patient information, it provides anonymous identification numbers and corresponding claims information, including gender, date of birth, administered medical services, and prescriptions given. Patient consent is not required to access the data stored in NHIRD. This study was approved by the Institutional Review Board (IRB) of China Medical University Hospital (CMUH104-REC2-115). The IRB waived the consent requirement.
Funding
This study was supported by Ministry of Science and Technology [Grant Number: MOST 103-2314-B-715- 001-MY2, MOST 104-2314-B-715-003-MY3, MOST 105-2320-B-039-059-MY3, and MOST 105-2634-F-039-001] and Mackay Medical College [Grant Number: RD1050179], Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence [Grant Number: MOHW105-TDU-B-212-133019], China Medical University Hospital, Academia Sinica Taiwan Biobank Stroke Biosignature Project [Grant Number: BM10501010037], NRPB Stroke Clinical Trial Consortium (MOHW107-TDU-B-212-123004), China Medical University Hospital, Academia Sinica Stroke Biosignature Project (BM10701010021), MOST Clinical Trial Consortium for Stroke (MOST 106-2321-B-039-005-), Tseng-Lien Lin Foundation, Taichung, Taiwan, and Katsuzo and Kiyo Aoshima Memorial Funds, Japan. The funders had no roles in study design, data collection and analysis, decision to publish, or preparation of the manuscript. No additional external funding was received for this study.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- ALF
Acute liver failure
- BD
Bipolar disorder
- CIs
Confidence intervals
- HRs
Hazard ratios
- HBV
Hepatitis B virus
- HCV
Hepatitis C virus
- ICD-9-CM
International Classification of Diseases, Ninth Revision, Clinical Modification
- IRB
Institutional Review Board
- LHID
Longitudinal Health Insurance Database
- NHI
National Health Insurance
- NHRI
National Health Research Institutes
Footnotes
Electronic supplementary material
The online version of this article (10.1186/s12967-018-1542-3) contains supplementary material, which is available to authorized users.
Lee-Won Chong, Chih-Chao Hsu and Chang-Yin Lee contributed equally to this work
Contributor Information
Lee-Won Chong, Email: leewonch@ms52.hinet.net.
Chih-Chao Hsu, Email: CTL2166Kimo@gmail.com.
Chang-Yin Lee, Email: mikeleefafa@gmail.com.
Ruey-Hwang Chou, Email: rhchou@gmail.com.
Cheng-Li Lin, Email: orangechengli@gmail.com.
Kuang-Hsi Chang, Email: kuanghsichang@gmail.com.
Yi-Chao Hsu, Email: hsuyc@mmc.edu.tw.
References
- 1.Alonso R, Aguilera A, Cordoba J, Fuertes A. Microbiological diagnosis of viral hepatitis. Enfermedades infecciosas y microbiologia clinica. 2015;33:e53–e62. doi: 10.1016/j.eimc.2014.08.002. [DOI] [PubMed] [Google Scholar]
- 2.Shlomai A, de Jong YP, Rice CM. Virus associated malignancies: the role of viral hepatitis in hepatocellular carcinoma. Semin Cancer Biol. 2014;26:78–88. doi: 10.1016/j.semcancer.2014.01.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Liu CJ, Chen PJ. Updates on the treatment and outcomes of dual chronic hepatitis C and B virus infection. World J Gastroenterol. 2014;20:2955–2961. doi: 10.3748/wjg.v20.i11.2955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Dinney CM, Zhao LD, Conrad CD, et al. Regulation of HBV-specific CD8(+) T cell-mediated inflammation is diversified in different clinical presentations of HBV infection. J Microbiol. 2015;53:718–724. doi: 10.1007/s12275-015-5314-y. [DOI] [PubMed] [Google Scholar]
- 5.Sandler NG, Koh C, Roque A, et al. Host response to translocated microbial products predicts outcomes of patients with HBV or HCV infection. Gastroenterology 2011;141:1220–30, 30 e1–3. [DOI] [PMC free article] [PubMed]
- 6.Mason A, Wick M, White H, Perrillo R. Hepatitis B virus replication in diverse cell types during chronic hepatitis B virus infection. Hepatology. 1993;18:781–789. doi: 10.1002/hep.1840180406. [DOI] [PubMed] [Google Scholar]
- 7.Wilkinson J, Radkowski M, Laskus T. Hepatitis C virus neuroinvasion: identification of infected cells. J Virol. 2009;83:1312–1319. doi: 10.1128/JVI.01890-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kim JM, Jang ES, Ok K, et al. Association between hepatitis C virus infection and Parkinson’s disease. Mov Disord. 2016;31:1584–1585. doi: 10.1002/mds.26755. [DOI] [PubMed] [Google Scholar]
- 9.Pakpoor J, Noyce A, Goldacre R, et al. Viral hepatitis and Parkinson disease: a national record-linkage study. Neurology. 2017;88:1630–1633. doi: 10.1212/WNL.0000000000003848. [DOI] [PubMed] [Google Scholar]
- 10.Tsai HH, Liou HH, Muo CH, Lee CZ, Yen RF, Kao CH. Hepatitis C virus infection as a risk factor for Parkinson disease: a nationwide cohort study. Neurology. 2016;86:840–846. doi: 10.1212/WNL.0000000000002307. [DOI] [PubMed] [Google Scholar]
- 11.Wu WY, Kang KH, Chen SL, et al. Hepatitis C virus infection: a risk factor for Parkinson’s disease. J Viral Hepat. 2015;22:784–791. doi: 10.1111/jvh.12392. [DOI] [PubMed] [Google Scholar]
- 12.Grande I, Berk M, Birmaher B, Vieta E. Bipolar disorder. Lancet. 2016;387:1561–1572. doi: 10.1016/S0140-6736(15)00241-X. [DOI] [PubMed] [Google Scholar]
- 13.Hayes JF, Miles J, Walters K, King M, Osborn DP. A systematic review and meta-analysis of premature mortality in bipolar affective disorder. Acta Psychiatr Scand. 2015;131:417–425. doi: 10.1111/acps.12408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Osby U, Brandt L, Correia N, Ekbom A, Sparen P. Excess mortality in bipolar and unipolar disorder in Sweden. Arch Gen Psychiatry. 2001;58:844–850. doi: 10.1001/archpsyc.58.9.844. [DOI] [PubMed] [Google Scholar]
- 15.Rege S, Hodgkinson SJ. Immune dysregulation and autoimmunity in bipolar disorder: synthesis of the evidence and its clinical application. Aust N Z J Psychiatry. 2013;47:1136–1151. doi: 10.1177/0004867413499077. [DOI] [PubMed] [Google Scholar]
- 16.Bai YM, Su TP, Tsai SJ, et al. Comparison of inflammatory cytokine levels among type I/type II and manic/hypomanic/euthymic/depressive states of bipolar disorder. J Affect Disord. 2014;166:187–192. doi: 10.1016/j.jad.2014.05.009. [DOI] [PubMed] [Google Scholar]
- 17.Hsu CC, Chen SC, Liu CJ, et al. Rheumatoid arthritis and the risk of bipolar disorder: a nationwide population-based study. PLoS ONE. 2014;9:e107512. doi: 10.1371/journal.pone.0107512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hsu YC, Hsu CC, Chang KH, et al. Increased subsequent risk of peptic ulcer diseases in patients with bipolar disorders. Medicine. 2015;94:e1203. doi: 10.1097/MD.0000000000001203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lin WS, Hu LY, Liu CJ, et al. Gastroesophageal reflux disease and risk for bipolar disorder: a nationwide population-based study. PLoS ONE. 2014;9:e107694. doi: 10.1371/journal.pone.0107694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Zahiu CD, Rimbas M. Neuropsychiatric side-effects of interferon-alpha treatment: pathophysiology and therapeutic options. Maedica. 2014;9:121–126. [PMC free article] [PubMed] [Google Scholar]
- 21.Qi M, Zhou B, Su M, Pan J, Zhang H. Escitalopram for intervention of psychiatric adverse events during peginterferon-alfa-2a and ribavirin treatment for chronic hepatitis C. J South Med Univ. 2013;33:1012–1016. [PubMed] [Google Scholar]
- 22.Quarantini LC, Miranda-Scippa A, Batista-Neves S, et al. A neuropsychological study comparing patients infected with HCV and HBV without psychiatric comorbidities. J Med Virol. 2009;81:1184–1188. doi: 10.1002/jmv.21508. [DOI] [PubMed] [Google Scholar]
- 23.Goh T, Dhillon R, Bastiampillai T. Manic induction with interferon alpha therapy. Aust N Z J Psychiatry. 2011;45:1004. doi: 10.3109/00048674.2011.615296. [DOI] [PubMed] [Google Scholar]
- 24.Gorgos L. Sexual transmission of viral hepatitis. Infect Dis Clin N Am. 2013;27:811–836. doi: 10.1016/j.idc.2013.08.002. [DOI] [PubMed] [Google Scholar]
- 25.Schreuder I, van der Sande MA, de Wit M, et al. Seroprevalence of HIV, hepatitis b, and hepatitis c among opioid drug users on methadone treatment in the netherlands. Harm Reduct J. 2010;7:25. doi: 10.1186/1477-7517-7-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tull MT, Gratz KL, Weiss NH. Exploring associations between borderline personality disorder, crack/cocaine dependence, gender, and risky sexual behavior among substance-dependent inpatients. Personal Disord. 2011;2:209–219. doi: 10.1037/a0021878. [DOI] [PubMed] [Google Scholar]
- 27.Ayano G, Tulu M, Haile K, et al. A systematic review and meta-analysis of gender difference in epidemiology of HIV, hepatitis B, and hepatitis C infections in people with severe mental illness. Ann Gen Psychiatry. 2018;17:16. doi: 10.1186/s12991-018-0186-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Nabavi B, Mitchell AJ, Nutt D. A lifetime prevalence of comorbidity between bipolar affective disorder and anxiety disorders: a meta-analysis of 52 interview-based studies of psychiatric population. EBioMedicine. 2015;2:1405–1419. doi: 10.1016/j.ebiom.2015.09.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Vohringer PA, Perlis RH. Discriminating between bipolar disorder and major depressive disorder. Psychiatr Clin N Am. 2016;39:1–10. doi: 10.1016/j.psc.2015.10.001. [DOI] [PubMed] [Google Scholar]
- 30.Angst J, Azorin JM, Bowden CL, et al. Prevalence and characteristics of undiagnosed bipolar disorders in patients with a major depressive episode: the BRIDGE study. Arch Gen Psychiatry. 2011;68:791–798. doi: 10.1001/archgenpsychiatry.2011.87. [DOI] [PubMed] [Google Scholar]
- 31.Garcia-Lopez A, Ezquiaga E, De Dios C, Agud JL. Depressive symptoms in early- and late-onset older bipolar patients compared with younger ones. Int J Geriatr Psychiatry. 2016;32:201–207. doi: 10.1002/gps.4465. [DOI] [PubMed] [Google Scholar]
- 32.Miranda-Pettersen K, Morais-de-Jesus M, Daltro-Oliveira R, et al. The fatigue impact scale for daily use in patients with hepatitis B virus and hepatitis C virus chronic infections. Ann Hepatol. 2015;14:310–316. [PubMed] [Google Scholar]
- 33.Chu CS, Chou PH, Chen YH, et al. Association between antipsychotic drug use and cataracts in patients with bipolar disorder: a population-based, nested case-control study. J Affect Disord. 2017;209:86–92. doi: 10.1016/j.jad.2016.11.019. [DOI] [PubMed] [Google Scholar]
- 34.Masi G, Liboni F. Management of schizophrenia in children and adolescents: focus on pharmacotherapy. Drugs. 2011;71:179–208. doi: 10.2165/11585350-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 35.Wu JF, Chang MH. Natural history of chronic hepatitis B virus infection from infancy to adult life -the mechanism of inflammation triggering and long-term impacts. J Biomed Sci. 2015;22:92. doi: 10.1186/s12929-015-0199-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Chen EQ, Zeng F, Zhou LY, Tang H. Early warning and clinical outcome prediction of acute-on-chronic hepatitis B liver failure. World J Gastroenterol. 2015;21:11964–11973. doi: 10.3748/wjg.v21.i42.11964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Butterworth RF. The concept of “the inflamed brain” in acute liver failure: mechanisms and new therapeutic opportunities. Metab Brain Dis. 2016;6:1283–1287. doi: 10.1007/s11011-015-9747-0. [DOI] [PubMed] [Google Scholar]
- 38.Bemeur C, Butterworth RF. Liver-brain proinflammatory signalling in acute liver failure: role in the pathogenesis of hepatic encephalopathy and brain edema. Metab Brain Dis. 2013;28:145–150. doi: 10.1007/s11011-012-9361-3. [DOI] [PubMed] [Google Scholar]
- 39.Dean B, Gibbons AS, Tawadros N, Brooks L, Everall IP, Scarr E. Different changes in cortical tumor necrosis factor-alpha-related pathways in schizophrenia and mood disorders. Mol Psychiatry. 2013;18:767–773. doi: 10.1038/mp.2012.95. [DOI] [PubMed] [Google Scholar]
- 40.Rosenblat JD, Cha DS, Mansur RB, McIntyre RS. Inflamed moods: a review of the interactions between inflammation and mood disorders. Prog Neuro-psychopharmacol Biol Psychiatry. 2014;53:23–34. doi: 10.1016/j.pnpbp.2014.01.013. [DOI] [PubMed] [Google Scholar]
- 41.Reus GZ, Fries GR, Stertz L, et al. The role of inflammation and microglial activation in the pathophysiology of psychiatric disorders. Neuroscience. 2015;300:141–154. doi: 10.1016/j.neuroscience.2015.05.018. [DOI] [PubMed] [Google Scholar]
- 42.Wang SH, Chen PJ, Yeh SH. Gender disparity in chronic hepatitis B: mechanisms of sex hormones. J Gastroenterol Hepatol. 2015;30:1237–1245. doi: 10.1111/jgh.12934. [DOI] [PubMed] [Google Scholar]
- 43.Montella M, D’Arena G, Crispo A, et al. Role of sex hormones in the development and progression of hepatitis B virus-associated hepatocellular carcinoma. Int J Endocrinol. 2015;2015:854530. doi: 10.1155/2015/854530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Yan Z, Tan W, Dan Y, et al. Estrogen receptor alpha gene polymorphisms and risk of HBV-related acute liver failure in the Chinese population. BMC Med Genet. 2012;13:49. doi: 10.1186/1471-2350-13-49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Adinolfi LE, Nevola R, Lus G, et al. Chronic hepatitis C virus infection and neurological and psychiatric disorders: an overview. World J Gastroenterol. 2015;21:2269–2280. doi: 10.3748/wjg.v21.i8.2269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Konstantinou D, Deutsch M. The spectrum of HBV/HCV coinfection: epidemiology, clinical characteristics, viralinteractions and management. Ann Gastroenterol. 2015;28:221–228. [PMC free article] [PubMed] [Google Scholar]
- 47.Liu CJ. Treatment of patients with dual hepatitis C virus and hepatitis B virus infection: resolved and unresolved issues. J Gastroenterol Hepatol. 2014;29:26–30. doi: 10.1111/jgh.12421. [DOI] [PubMed] [Google Scholar]
- 48.Chang ML, Liaw YF. Hepatitis B flares in chronic hepatitis B: pathogenesis, natural course, and management. J Hepatol. 2014;61:1407–1417. doi: 10.1016/j.jhep.2014.08.033. [DOI] [PubMed] [Google Scholar]
- 49.Sperl J. Reactivation of chronic hepatitis B. Vnitr Lek. 2013;59:591–596. [PubMed] [Google Scholar]
- 50.Fletcher NF, Wilson GK, Murray J, et al. Hepatitis C virus infects the endothelial cells of the blood-brain barrier. Gastroenterology. 2012;142(634–43):e6. doi: 10.1053/j.gastro.2011.11.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Grover VP, Pavese N, Koh SB, et al. Cerebral microglial activation in patients with hepatitis C: in vivo evidence of neuroinflammation. J Viral Hepat. 2012;19:e89–e96. doi: 10.1111/j.1365-2893.2011.01510.x. [DOI] [PubMed] [Google Scholar]
- 52.Liu Z, Zhao F, He JJ. Hepatitis C virus (HCV) interaction with astrocytes: nonproductive infection and induction of IL-18. J Neurovirol. 2014;20:278–293. doi: 10.1007/s13365-014-0245-7. [DOI] [PubMed] [Google Scholar]
- 53.Barrientos RM, Kitt MM, Watkins LR, Maier SF. Neuroinflammation in the normal aging hippocampus. Neuroscience. 2015;309:84–99. doi: 10.1016/j.neuroscience.2015.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Hung CH, Chen CH, Lee CM, et al. Role of viral genotypes and hepatitis B viral mutants in the risk of hepatocellular carcinoma associated with hepatitis B and C dual infection. Intervirology. 2013;56:316–324. doi: 10.1159/000350738. [DOI] [PubMed] [Google Scholar]
- 55.Negro F, Forton D, Craxi A, Sulkowski MS, Feld JJ, Manns MP. Extrahepatic morbidity and mortality of chronic hepatitis C. Gastroenterology. 2015;149:1345–1360. doi: 10.1053/j.gastro.2015.08.035. [DOI] [PubMed] [Google Scholar]
- 56.Rosenthal E, Cacoub P. Extrahepatic manifestations in chronic hepatitis C virus carriers. Lupus. 2015;24:469–482. doi: 10.1177/0961203314556140. [DOI] [PubMed] [Google Scholar]
- 57.Lecardeur L, Benarous X, Milhiet V, Consoli A, Cohen D. Management of bipolar 1 disorder in children and adolescents. Encephale. 2014;40:143–153. doi: 10.1016/j.encep.2014.02.006. [DOI] [PubMed] [Google Scholar]
- 58.Udal AH, Egeland J, Oygarden B, et al. Differentiating between comorbidity and symptom overlap in ADHD and early onset bipolar disorder. Dev Neuropsychol. 2014;39:249–261. doi: 10.1080/87565641.2014.886692. [DOI] [PubMed] [Google Scholar]
- 59.Hoffmann A, Sportelli V, Ziller M, Spengler D. From the psychiatrist’s couch to induced pluripotent stem cells: bipolar disease in a dish. Int J Mol Sci. 2018;19:770. doi: 10.3390/ijms19030770. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Table S1. Distribution of age, gender, and comorbidity between hepatitis infection and comparison cohort with propensity score matching. Table S2. Estimation of bipolar Incidence and hazard ratio by Cox proportional hazard models with propensity score matching.
Data Availability Statement
Data are available from the NHIRD published by Taiwan National Health Insurance Bureau. Due to legal restrictions imposed by the Government of Taiwan in relation to the ‘Personal Information Protection Act’, data cannot be made publicly available. Requests for data can be sent as a formal proposal to the NHIRD (http://nhird.nhri.org.tw).