
Fig 2.
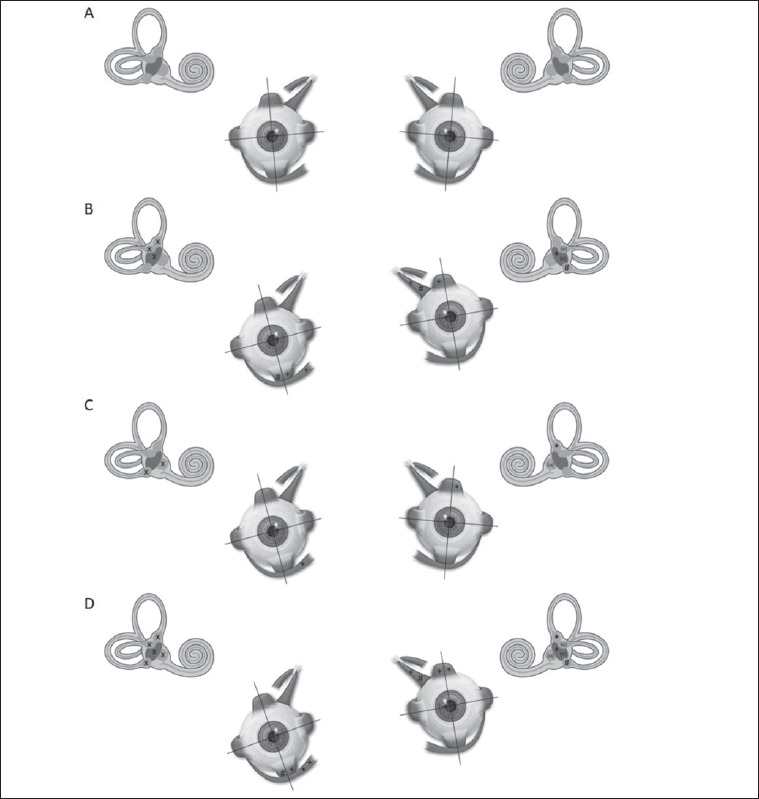
Expected changes from the normal (A) in binocular cyclotorsion and vertical alignment due to the asymmetrical tonic activation of vestibular receptors. B: Right superior vestibular neuritis (SVN). Deafferentation (x) of the right anterior semicircular canal (ASC) and of the right utricular macula (UM). The left posterior semicircular canal (PSC) exerts a tonic effect (#) on the left superior oblique muscle (SOM; incyclotorsion) and of the right inferior rectus muscle (IRM; hypotropia). The left medial part of UM exerts a tonic effect (+) on the left SOM, on the left superior rectus muscle (SRM; hypertropia), on the right inferior oblique muscle (IOM, excyclotorsion) and on the right IRM. The result will be a right hypotropia with an abnormal excyclotorsion, a left hypertropia with an incyclotorsion lower than the contralateral excyclotorsion. C: Right inferior vestibular neuritis (IVN). Deafferentation (x) of the right PSC and of the right saccular macula (SM). The left ASC exerts a tonic effect (*) on the left SRM and on the right IOM. The result will be an abnormal right excyclotorsion and a left hypertropia with a normal excyclotorsion. D: Right total vestibular neuritis. Deafferentation of all vestibular receptors (x). The tonic effect of the left PSC (#), of the left medial part of the UM (+) and of the left ASC (*) is equivalent to the sum of the previous two situations. The result will be a right hypotropia with an abnormal excyclotorsion more pronounced than in SVN and IVN and a more pronounced left hypertropia than in SVN and IVN with an incyclotorsion comparable to that of SVN. The tonic effect (°) of the left horizontal semicircular canal, of the left lateral part of the UM and of the SM is not reported given their null effect on SOB, IOM, SRM and IRM.