

Abstract
Objectives:
To analyze optic nerve head images of pseudoexfoliative glaucoma (PXG) patients and healthy volunteers obtained with enhanced depth imaging spectral domain-optical coherence tomography (SD-OCT).
Materials and Methods:
Seventy patients with PXG and 68 age- and gender-matched healthy subjects were included in this prospective study. The prelaminar tissue and lamina cribrosa were imaged using spectralis OCT with the enhanced depth imaging technique. PXG disease stage was determined with visual field to evaluate relationships between prelaminar tissue thickness (PTT), lamina cribrosa thickness (LT) and disease severity.
Results:
There was no significant difference between the PXG group and control group with regard to age, gender, central corneal thickness, or axial length. The mean PTT (93.1±44.5 μm, p<0.05) and LT (206.3±33.6 μm p<0.05) values of the PXG group were significantly lower compared to the control group in enhanced depth imaging OCT measurements. The PXG patients were divided into stages according to visual field defect severity. While a significant difference was not detected in PTT based on disease stage (p>0.05), a statistically significant difference was detected between stages for LT (p<0.05).
Conclusion:
A thinner PTT was correlated with the presence of PXG but not with the severity of glaucoma. In addition, LT has a stronger relationship with disease severity and progression compared to PTT.
Keywords: Enhanced depth imaging, lamina cribrosa, optical coherence tomography, prelaminar tissue, pseudoexfoliation glaucoma
Introduction
Pseudoexfoliation syndrome (PEX) is an age-related generalized basal membrane disease. It is characterized by the excessive and progressive accumulation of fibrillary material in various ocular and extraocular tissues.1 Pseudoexfoliative glaucoma (PXG) develops in the vast majority of patients with PEX.2 PXG is the most common form of secondary open angle glaucoma types.3 It is characterized by high intraocular pressure (IOP), severe fluctuation of IOP, rapid progression, poor prognosis.4 The structural changes in lamina cribrosa (LC) beside elevated IOP and severe fluctuation were suggested to be associated with poor prognosis.5,6,7 Elastotic changes were detected in the LC of eyes with PXG.7 In a study conducted with atomic force microscopy, the stiffness of the LC was reported to decrease in pseudoexfoliative eyes.8 In addition, LC deformation may lead to ischemia through the compressive effect on the laminar capillary.9,10 Since laminar region has been considered the primary site of axonal injury in glaucoma, these alterations may contribute to the rapid progression of PXG.3 The prelaminar region which covers the LC is composed of retinal ganglion cells, axon bundles, astrocytes, capillaries and extraocular material. Its thickness may reduce as the result of ischemia.11 Prelaminar tissue thickness (PTT) was also shown to decrease as a response to acute12 and chronic13 IOP elevation.
Although optical coherence tomography (OCT) can visualize the anterior margins of LC and prelaminar tissue, it cannot visualize the posterior margins of the LC. It is possible to safely visualize the posterior margins of the LC and optic nerve head (ONH) with enhanced depth imaging (EDI), which is present in spectral domain (SD)-OCT.14,15,16,17
In our study, we analyzed ONH images of PXG patients and healthy volunteers obtained with EDI SD-OCT. We aimed to investigate the presence of a significant difference between the PXG group and control group with regard to PTT and LC thickness (LT). We also planned to investigate the relationship between PTT, LC and PXG disease stage determined with visual field, retinal nerve fiber layer (RNFL) thickness and vertical cup/disc ratio.
Materials and Methods
This prospective study was approved by the Medical Ethics Committee of İzmir Tepecik Training and Research Hospital. The study was carried out in adherence to the tenets of the Declaration of Helsinki and written informed consent was obtained from all participants. Seventy patients with PXG and 68 age- and gender-matched healthy subjects were recruited from October 2014 to May 2015. Medical histories and demographic data of all participants were noted. All subjects underwent ophthalmic examination including best-corrected visual acuity, central corneal thickness with non-contact specular microscope (sp-2000p, Topcon, Japan), axial length (Lenstar LS900, Haag-Streit AG, Koeniz, Switzerland), Goldmann applanation tonometry, slit-lamp biomicroscopy, gonioscopy, dilated fundus photography, visual field test with Octopus 101 automated perimetry (Interzeag AG, Schlieren, Switzerland) using G2 program (central 30-2 threshold strategy) and SD-OCT scanning (Spectralis OCT, Heidelberg Engineering, Heidelberg, Germany). The vertical cup/disc ratio was noted on dilated fundus examination.
PXG was diagnosed when baseline IOP >21 mmHg, open anterior chamber, glaucomatous optic neuropathy, visual field defects typical of glaucoma and pseudoexfoliation material on the anterior lens capsule, pupillary margin, or both. The Hodapp-Anderson-Parrish system modified for Octopus perimetry was used to classify patients with glaucoma.18 PXG patients were stratified into five groups according to the severity of visual field defects. Stage 1 (early) glaucoma was characterized by a mean deviation score (MDS) of -0.7 to +4.4 dB; stage 2 (moderate) glaucoma by an MDS of +4.5 to +9.4 dB; stage 3 (advanced) glaucoma by an MDS of +9.5 to +15.3 dB; stage 4 (severe) glaucoma by an MDS of +15.4 to +23.1 dB and stage 5 (end-stage) glaucoma by an MDS of ≥ +23.2.
The inclusion criteria for eyes were a best-corrected visual acuity of 20/40 or better, spherical refraction within ±5.0 diopters and cylinder correction within ±3 diopters. At least two visual field tests were performed to minimize the learning effect. Only reliable (false positive/negative under 15% and reliability factor under 15) and compatible visual field results were included. The control group participants had normal eye exam and perimetry. The exclusion criteria included cardiovascular disease, diabetes, head trauma, Alzheimer’s disease, history of stroke, claustrophobia, ocular trauma and other ocular disease affecting visual field and RNFL. Patients whose IOP could not be controlled with medical treatment and end-stage patients were excluded. If both eyes had PXG, one eye was randomly selected for inclusion in the study.
Peripapillary RNFL Measurement with Spectral Domain-Optical Coherence Tomography
All OCT assessments involved in the study were performed by the same experienced ophthalmologist. For OCT examination, the RNFL thicknesses were assessed by scanning a peripapillary circle with a diameter of 3.4 mm and 768 A-scans. Only well-centered images with a signal strength of >20 dB were used. The RNFL thicknesses were automatically segmented and measured using Spectralis software version 5.3.3.0.
Measurement of Prelaminar Tissue Thickness and Lamina Cribrosa Thickness by Spectral Domain-Optical Coherence Tomography Enhanced Depth Imaging
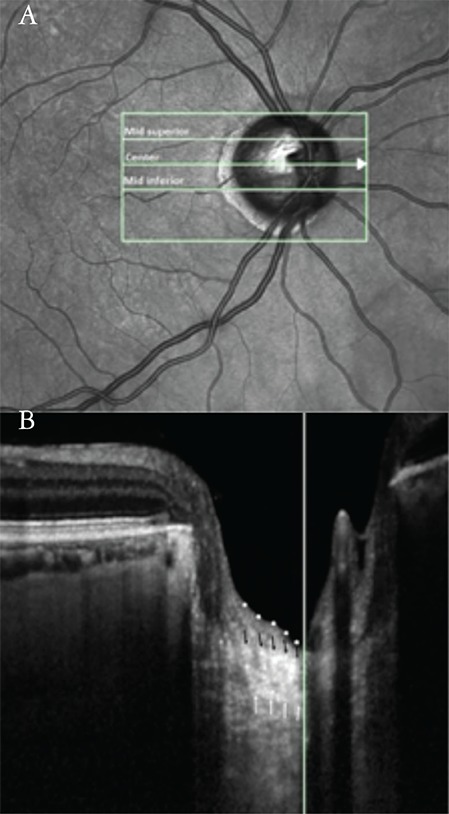
The prelaminar tissue and LC were imaged using the Spectralis OCT with the EDI technique. An internal nasal fixation light was used to center the disc in the 10´15° rectangle. This rectangle was scanned with 97 sections (384 A-scans) with an interval of 30 µm. An average of 45 frames was produced for each cross-sectional B-scan. Thickness measurements were done using Spectralis software version 5.3.3.0. LT and PTT were measured at the vertical center of ONH of 3 B-scans (mid-superior, center, mid-inferior). The center of the ONH was identified as the point where central retinal vessels originate from the ONH. Mid-superior and mid-inferior locations were determined as the midpoints between the center and the margins of the optic disc (Figure 1A). LT was defined as the distance between the anterior and posterior borders of the LC. The borders of the LC were considered to be where the highly reflective region started and finished. Prelaminar tissue was defined as the reflective field on the anterior margin of the LC (Figure 1B). For each patient, the mean of the measurements at the mid-superior, center and mid-inferior locations were regarded as the average PTT and LT. The average PTT and LT were used for statistical analyses. The relationship between PTT, LC and PXG disease stage was determined with visual field, RNFL thickness and vertical cup/disc ratio.
Figure 1. Simultaneous images of a pseudoexfoliation glaucoma patient. a) The measurement of prelaminar tissue thickness and laminar thickness (LT) were performed at the presumed vertical center of each of the 3 B-scans (mid-superior, center, mid-inferior). The short vertical line crossing the center horizontal line corresponds to the long white vertical line in the next image. B) The image shows a horizontal cross-sectional B-scan of the optic nerve head at the center line. The vertical white line marks the vertical center of the optic nerve head. The borders of the highly reflective region were accepted as the borders of the lamina cribrosa (LC); white arrows indicate the posterior borders and black arrows indicate the anterior borders of the LC. LT was defined as the distance between the anterior and posterior LC borders. Prelaminar tissue was defined as the reflective field on the anterior margin of the LC. White dots delineate the anterior borders of the prelaminar tissue.
Statistical Analysis
All statistical analyses were performed with Statistical Packages for the Social Sciences (SPSS, version 22, IBM corp., Armonk, New York, USA). A p value <0.05 was considered statistically significant. For comparison of groups, independent t test was used for continuous variables and chi-square test was used for categorical data. Comparison of the patients in different disease stages in the PXG group was done with Kruskal-Wallis test. Pearson correlation analysis was used for correlation analysis.
Results
ONH EDI OCT images of 70 PXG patients and 68 healthy volunteers were analyzed. Two patients in the PXG group and 3 patients in the control group were excluded from the study because the posterior margins of the LC were not visualized clearly. Sixty-eight patients in the PXG group and 65 patients in the control group were included in the statistical analysis.
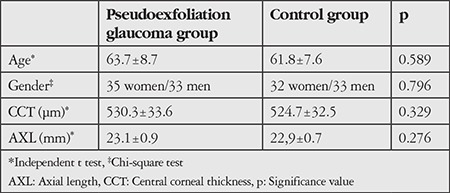
There was no significant difference between PXG group and control group with regard to age, gender, central corneal thickness, or axial length. Baseline characteristics of the participants are shown in Table 1.
Table 1. Baseline characteristics of the pseudoexfoliation glaucoma and control groups.
Mean PTT (p<0.05) and LT (p<0.05) values of the PXG group were seen to be statistically significantly lower compared to the control group in EDI OCT measurements. While mean PTT was 93.1±44.5 µm in the PXG group, it was 213.9±141.1 µm in the control group. Mean LT was calculated as 206.3±33.6 µm in the PXG group and 269.1±24.1 µm in the control group.
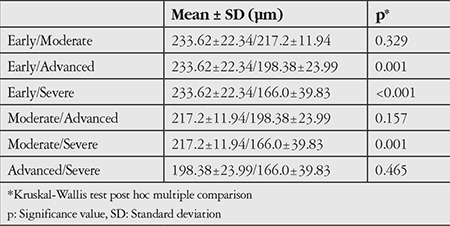
The PXG patients were divided into stages according to visual field defect severity. There were 16 patients (23.5%) in early stage, 21 patients (30.9%) in moderate stage, 18 patients (26.5%) in advanced stage and 13 patients (19.1%) in severe stage. While a significant difference was not detected in PTT in comparison of disease stages (p>0.05), a statistically significant difference was detected between stages for LT (p<0.05). Post hoc multiple comparison results for LT are shown in Table 2.
Table 2. Multiple comparison of lamina cribrosa thickness of each group.
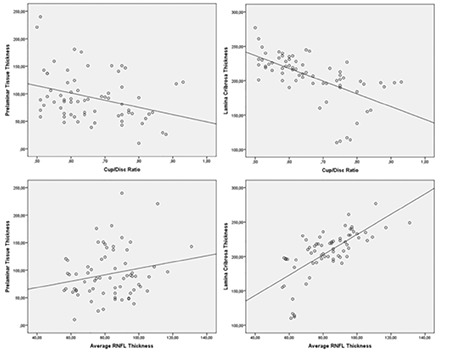
While a weak correlation was detected with vertical cup/disc ratio in correlation analysis done for PTT, a correlation was not detected with average of RNFL thicknesses (RNFLav). LT was found to be negatively correlated with vertical cup/disc ratio, positively correlated with RNFLav (Table 3, Figure 2).
Table 3. Correlation between enhanced depth imaging optical coherence tomography measurements vs. vertical cup/disc ratio and average retina nerve fiber layer thickness.
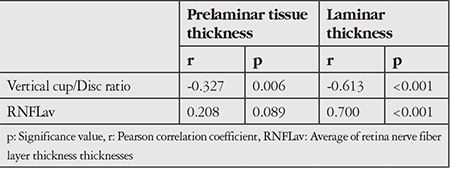
Figure 2. Scatter plots to exhibit correlations between enhanced depth imaging optical coherence tomography measurements vs. vertical cup/disc ratio and average retinal nerve fiber layer (RNFL) thickness.
Discussion
The development of EDI in SD-OCT enabled clear visualization of prelaminar and laminar tissues and accelerated investigation of the relationships between these structures and glaucoma.14,15,16,17,19 Park et al.16 pointed out a limitation; with EDI OCT, the deeper portion and posterior border of the LC lack the clarity required for precise characterization of the structure. Recently, high-penetration OCT, also known as swept-source-OCT, which uses a center wavelength of approximately 1,050 nm instead of 840 nm (the wavelength used by current SD-OCT instruments), allows the imaging of deeper ocular layers, including the choroid and LC. It has been promised to enable more accurate characterization of the LC.20,21 In our study, patients whose posterior LC margins were not visualized clearly were excluded from the study. In the studies done using EDI, PTT was shown to decrease with the elevation of IOP and increased again following treatment.12,13,22,23,24 In addition, Jung et al.13 reported that prelaminar tissue is thinner in primary open angle glaucoma (POAG) patients compared to normotensive glaucoma patients (NTG). Chung et al.25 found PTT and LT low in progressing glaucoma patients compared to glaucoma patients who do not show progression. In the study of Chung et al.25, PTT and LT were found to be related to glaucoma progression; however, only LT was seen to be related to glaucoma progression in multivariate analysis.
To the best of our knowledge, this is the first study to investigate the relationship between PTT and PXG. In our study, PTT was significantly thinner in PXG patients whose IOP was within normal ranges with medical therapy compared to the control group. However, there was no significant difference between stages in the PXG group. In addition, PTT was poorly correlated with vertical cup/disc ratio and a correlation was not found with RNFLav. The standard deviation of PTT is high, which indicates that PTT values are distributed over a wide range in this patient group. The PTT values are also widely distributed in the population and are not homogeneously distributed. Therefore, there is no need to evaluate PTT in follow-up. The results of our study showed that a thinner PTT was correlated with the presence of PXG but not with the severity of glaucoma.
LC is one of the ocular structures where pathologic changes are seen in PEX syndrome.5,6,7,26,27,28 Insufficient LOXL1 tissue levels may lead to elastotic changes in affected tissues like LC.29 Braunsmann et al.8 reported that LC stiffness significantly decreased in their study done with cadaver eyes with PXG. Since the LC is the primary site of axonal injury in glaucoma, elastotic alteration and decreased LC stiffness may predispose to glaucoma development in patients with PEX.3 In a study performed with an SD-OCT EDI system, Park et al.14 found LT was significantly thinner in POAG and NTG patients compared to a control group. In addition, they showed that LT decreased as disease stage increased in glaucoma patients.14 Kim et al.30 reported that LC was thinner in PXG patients in similar disease stages compared to POAG patients. In our study, LT was lower in PXG patients compared to the control group. Mean LT was reported to decrease with the increase in disease stage. Park and Park31 determined that the diagnostic ability of LT is similar to peripapillary RNLF thickness and better than peripapillary RNFL thickness in early stage patients. Lee et al.32 reported that thin LC was associated with progressive RNLF thinning. In our study, LT was seen to be negatively correlated with vertical cup/disc ratio and positively correlated with RNFLav. In light of these data, it was concluded that LT may be a risk factor for the development of PXG. In addition, the laminar region could be one of the targets of glaucomatous injury. Long-term studies with more patients are needed to support this conclusion.
Study Limitation
A limitation of our study is that patients with PEX were not included; we only compared PXG patients and healthy subjects.
Conclusion
In conclusion, thinning in PTT and LT parameters in SD-OCT EDI systems was correlated with the presence of PXG. In addition, LT has a stronger relationship with disease severity and progression compared to PTT. SD-OCT EDI mode is a recently developed technology and is not available in many centers and LT is not routinely assessed in glaucoma clinics. With advances in OCT systems, LT may be used for diagnosis and follow-up.
Footnotes
Ethics
Ethics Committee Approval: This prospective study was approved by the Medical Ethics Committee of İzmir Tepecik Training and Research Hospital (decision number: 21/12).
Informed Consent: Available.
Peer-review: Externally peer-reviewed.
Authorship Contributions
Surgical and Medical Practices: Mehmet Giray Ersöz, Duygu Kunak Mart, Emre Ayıntap, İrfan Botan Güneş, Hakkı Özgür Konya, Concept: Mehmet Giray Ersöz, Leyla Hazar, Design: Mehmet Giray Ersöz, Leyla Hazar, Data Collection or Processing: Mehmet Giray Ersöz, Duygu Kunak Mart, Leyla Hazar, Emre Ayıntap, İrfan Botan Güneş, Hakkı Özgür Konya, Analysis or Interpretation: Mehmet Giray Ersöz, Leyla Hazar, Literature Search: Mehmet Giray Ersöz, Leyla Hazar, Writing: Mehmet Giray Ersöz.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study received no financial support.
References
- 1.Lindberg JG. Clinical investigations on depigmentation of the pupillary border and translucency of the iris in cases of senile cataract and in normal eyes in elderly persons. Acta Ophthalmol Suppl. 1989;190:1–96. [PubMed] [Google Scholar]
- 2.Ritch R, Schlotzer-Schrehardt U. Exfoliation syndrome. Surv Ophthalmol. 2001;45:265–315. doi: 10.1016/s0039-6257(00)00196-x. [DOI] [PubMed] [Google Scholar]
- 3.Anastasopoulos E, Founti P, Topouzis F. Update on pseudoexfoliation syndrome pathogenesis and associations with intraocular pressure, glaucoma and systemic diseases. Curr Opin Ophthalmol. 2015;26:82–89. doi: 10.1097/ICU.0000000000000132. [DOI] [PubMed] [Google Scholar]
- 4.Heijl A, Bengtsson B, Hyman L, Leske MC Early Manifest Glaucoma Trial Group. Natural history of open-angle glaucoma. Ophthalmology. 2009;116:2271–2276. doi: 10.1016/j.ophtha.2009.06.042. [DOI] [PubMed] [Google Scholar]
- 5.Netland PA, Ye H, Streeten BW, Hernandez MR. Elastosis of the lamina cribrosa in pseudoexfoliation syndrome with glaucoma. Ophthalmology. 1995;102:878–886. doi: 10.1016/s0161-6420(95)30939-6. [DOI] [PubMed] [Google Scholar]
- 6.Pena JD, Netland PA, Vidal I, Dorr DA, Rasky A, Hernandez MR. Elastosis of the lamina cribrosa in glaucomatous optic neuropathy. Exp Eye Res. 1998;67:517–524. doi: 10.1006/exer.1998.0539. [DOI] [PubMed] [Google Scholar]
- 7.Schlötzer-Schrehardt U, Hammer CM, Krysta AW, Hofmann-Rummelt C, Pasutto F, Sasaki T, Kruse FE, Zenkel M. LOXL1 deficiency in the lamina cribrosa as candidate susceptibility factor for a pseudoexfoliation-specific risk of glaucoma. Ophthalmology. 2012;119:1832–1843. doi: 10.1016/j.ophtha.2012.03.015. [DOI] [PubMed] [Google Scholar]
- 8.Braunsmann C, Hammer CM, Rheinlaender J, Kruse FE, Schäffer TE, Schlötzer-Schrehardt U. Evaluation of lamina cribrosa and peripapillary sclera stiffness in pseudoexfoliation and normal eyes by atomic force microscopy. Invest Ophthalmol Vis Sci. 2012;53:2960–2967. doi: 10.1167/iovs.11-8409. [DOI] [PubMed] [Google Scholar]
- 9.Emery JM, Landis D, Paton D, Boniuk M, Craig JM. The lamina cribrosa in normal and glaucomatous human eyes. Trans Am Acad Ophthalmol Otolaryngol. 1974;78:290–297. [PubMed] [Google Scholar]
- 10.Burgoyne CF, Downs JC, Bellezza AJ, Suh JK, Hart RT. The optic nevre head as a biomechanical structure: a new paradigm for understanding the role of IOP-related stress and strain in the pathophysiology of glaucomatous optic nerve head damage. Prog Retin Eye Res. 2005;24:39–73. doi: 10.1016/j.preteyeres.2004.06.001. [DOI] [PubMed] [Google Scholar]
- 11.Hernandez MR, Igoe F, Neufeld AH. Extracellular matrix of the human optic nerve head. Am J Ophthalmol. 1986;102:139–148. doi: 10.1016/0002-9394(86)90134-0. [DOI] [PubMed] [Google Scholar]
- 12.Agoumi Y, Sharpe GP, Hutchison DM, Nicolela MT, Artes PH, Chauhan BC. Laminar and prelaminar tissue displacement during intraocular pressure elevation in glaucoma patients and healthy controls. Ophthalmology. 2011;118:52–59. doi: 10.1016/j.ophtha.2010.05.016. [DOI] [PubMed] [Google Scholar]
- 13.Jung YH, Park HY, Jung KI, Park CK. Comparison of prelaminar thickness between primary open angle glaucoma and normal tension glaucoma patients. PLoS One. 2015;10:e0120634. doi: 10.1371/journal.pone.0120634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Park HY, Jeon SH, Park CK. Enhanced depth imaging detects lamina cribrosa thickness differences in normal tension glaucoma and primary open-angle glaucoma. Ophthalmology. 2012;119:10–20. doi: 10.1016/j.ophtha.2011.07.033. [DOI] [PubMed] [Google Scholar]
- 15.Lee EJ, Kim TW, Weinreb RN, Park KH, Kim SH, Kim DM. Visualization of the lamina cribrosa using enhanced depth imaging spectral-domain optical coherence tomography. Am J Ophthalmol. 2011;152:87–95. doi: 10.1016/j.ajo.2011.01.024. [DOI] [PubMed] [Google Scholar]
- 16.Park SC, De Moraes CG, Teng CC, Tello C, Liebmann JM, Ritch R. Enhanced depth imaging optical coherence tomography of deep optic nevre complex structures in glaucoma. Ophthalmology. 2012;119:3–9. doi: 10.1016/j.ophtha.2011.07.012. [DOI] [PubMed] [Google Scholar]
- 17.Ersoz MG, Mart DK, Ayintap E, Hazar L, Gunes IB, Adiyeke SK, Dogan B. The factors influencing peripapillary choroidal thickness in primary open-angle glaucoma. Int Ophthalmol. 2017;37:827–833. doi: 10.1007/s10792-016-0346-9. [DOI] [PubMed] [Google Scholar]
- 18.Mills RP, Budenz DL, Lee PP, Noecker RJ, Walt JG, Siegartel LR, Evans SJ, Doyle JJ. Categorizing the stage of glaucoma from pre-diagnosis to end-stage disease. Am J Ophthalmol. 2006;141:24–30. doi: 10.1016/j.ajo.2005.07.044. [DOI] [PubMed] [Google Scholar]
- 19.Yang H, Qi J, Hardin C, Gardiner SK, Strouthidis NG, Fortune B, Burgoyne CF. Spectral-domain optical coherence tomography enhanced depth imaging of the normal and glaucomatous nonhuman primate optic nerve head. Invest Ophthalmol Vis Sci. 2012;53:394–405. doi: 10.1167/iovs.11-8244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Nuyen B, Mansouri K, N Weinreb R. Imaging of the Lamina Cribrosa using Swept-Source Optical Coherence Tomography. J Curr Glaucoma Pract. 2012;6:113–119. doi: 10.5005/jp-journals-10008-1117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Loureiro MM, Vianna JR, Danthurebandara VM, Sharpe GP, Hutchison DM, Nicolela MT, Chauhan BC. Visibility of Optic Nerve Head Structures With Spectral-domain and Swept-source Optical Coherence Tomography. J Glaucoma. 2017;26:792–797. doi: 10.1097/IJG.0000000000000740. [DOI] [PubMed] [Google Scholar]
- 22.Reis AS, O’Leary N, Stanfield MJ, Shuba LM, Nicolela MT, Chauhan BC. Laminar displacement and prelaminar tissue thickness change after glaucoma surgery imaged with optical coherence tomography. Invest Ophthalmol Vis Sci. 2012;53:5819–5826. doi: 10.1167/iovs.12-9924. [DOI] [PubMed] [Google Scholar]
- 23.Barrancos C, Rebolleda G, Oblanca N, Cabarga C, Muñoz-Negrete FJ. Changes in lamina cribrosa and prelaminar tissue after deep sclerectomy. Eye (Lond). 2014;28:58–65. doi: 10.1038/eye.2013.238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lee EJ, Kim TW, Weinreb RN. Reversal of lamina cribrosa displacement and thickness after trabeculectomy in glaucoma. Ophthalmology. 2012;119:1359–1366. doi: 10.1016/j.ophtha.2012.01.034. [DOI] [PubMed] [Google Scholar]
- 25.Chung HS, Sung KR, Lee JY, Na JH. Lamina Cribrosa-Related Parameters Assessed by Optical Coherence Tomography for Prediction of Future Glaucoma Progression. Curr Eye Res. 2016;41:806–813. doi: 10.3109/02713683.2015.1052519. [DOI] [PubMed] [Google Scholar]
- 26.Quigley HA, Hohman RM, Addicks EM, Massof RW, Green WR. Morphologic changes in the lamina cribrosa correlated with neural loss in open-angle glaucoma. Am J Ophthalmol. 1983;95:673–91. doi: 10.1016/0002-9394(83)90389-6. [DOI] [PubMed] [Google Scholar]
- 27.Jonas JB, Berenshtein E, Holbach L. Lamina cribrosa thickness and spatial relationships between intraocular space and cerebrospinal fluid space in highly myopic eyes. Invest Ophthalmol Vis Sci. 2004;45:2660–2665. doi: 10.1167/iovs.03-1363. [DOI] [PubMed] [Google Scholar]
- 28.Hammer T, Schlötzer-Schrehardt U, Naumann GO. Unilateral or asymmetric pseudoexfoliation syndrome? An ultrastructural study. Arch Ophthalmol. 2001;119:1023–1031. doi: 10.1001/archopht.119.7.1023. [DOI] [PubMed] [Google Scholar]
- 29.Thorleifsson G, Magnusson KP, Sulem P, Walters GB, Gudbjartsson DF, Stefansson H, Jonsson T, Jonasdottir A, Jonasdottir A, Stefansdottir G, Masson G, Hardarson GA, Petursson H, Arnarsson A, Motallebipour M, Wallerman O, Wadelius C, Gulcher JR, Thorsteinsdottir U, Kong A, Jonasson F, Stefansson K. Common sequence variants in the LOXL1 gene confer susceptibility to exfoliation glaucoma. Science. 2007;317:1397–1400. doi: 10.1126/science.1146554. [DOI] [PubMed] [Google Scholar]
- 30.Kim S, Sung KR, Lee JR, Lee KS. Evaluation of lamina cribrosa in pseudoexfoliation syndrome using spectral-domain optical coherence tomography enhanced depth imaging. Ophthalmology. 2013;120:1798–1803. doi: 10.1016/j.ophtha.2013.02.015. [DOI] [PubMed] [Google Scholar]
- 31.Park HY, Park CK. Diagnostic capability of lamina cribrosa thickness by enhanced depth imaging and factors affecting thickness in patients with glaucoma. Ophthalmology. 2013;120:745–752. doi: 10.1016/j.ophtha.2012.09.051. [DOI] [PubMed] [Google Scholar]
- 32.Lee EJ, Kim TW, Kim M, Kim H. Influence of lamina cribrosa thickness and depth on the rate of progressive retinal nerve fiber layer thinning. Ophthalmology. 2015;122:721–729. doi: 10.1016/j.ophtha.2014.10.007. [DOI] [PubMed] [Google Scholar]