
Fig. 4. High P-eIF2α expression in human prostate tumors with loss of PTEN function is associated with increased risk of metastasis or death after surgery.
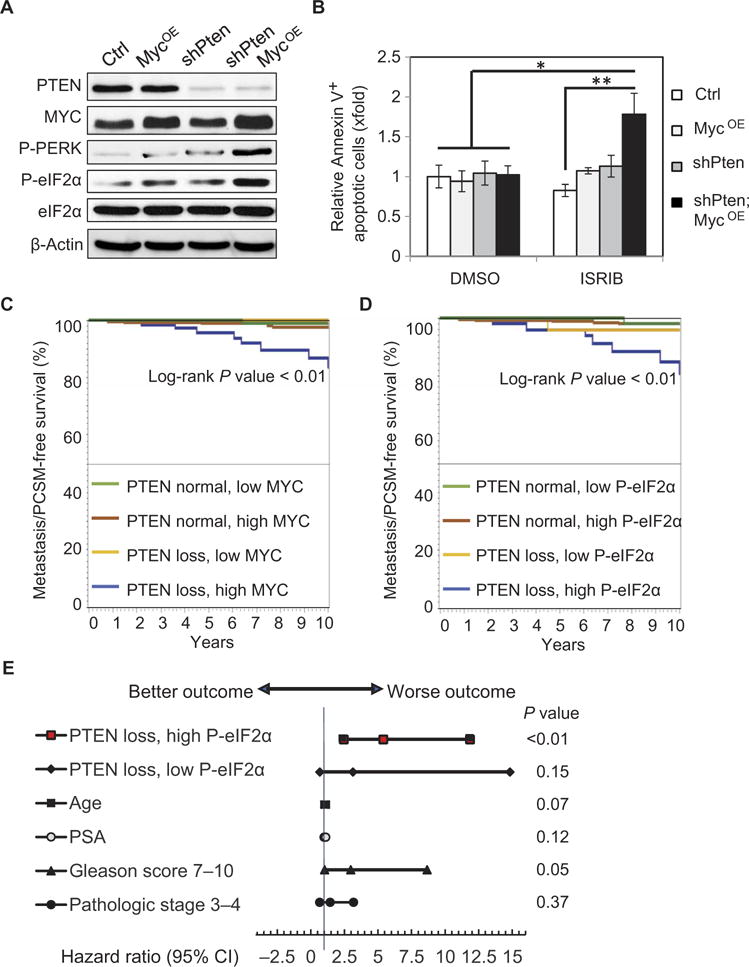
(A) Representative Western blot showing PTEN, MYC, P-PERK, P-eIF2α, and total eIF2α expression with β-actin loading control (Ctrl) in human prostatic RWPE-1 cell lines. (B) Quantification of annexin V–positive cells analyzed by flow cytometry relative to control cells after treatment with DMSO or 500 nM ISRIB for 9 hours (n = 3, mean ± SEM) *P < 0.05, t test. (C) Kaplan-Meier analysis of clinical progression–free survival [progression defined as visceral or bone metastasis or PCSM] for patients with normal PTEN expression versus PTEN loss and relative MYC expression identified by IF from the TMA. (D) Kaplan-Meier analysis of MET/PCSM for patients with normal PTEN expression versus PTEN loss grouped by eIF2α phosphorylation. (E) Cox proportional hazards regression results are shown in a Forest plot of hazard ratios and 95% CI for factors associated with risk of clinical progression after surgery. Independent factors are tumor with PTEN loss/low P-eIF2α or PTEN loss/high P-eIF2α versus a reference group with normal PTEN expression; age in years; PSA in nanograms per milliliter; Gleason score > 7 versus 6; and pathological stage T3-T4 versus T2 at the time of prostatectomy.