
Figure 3.
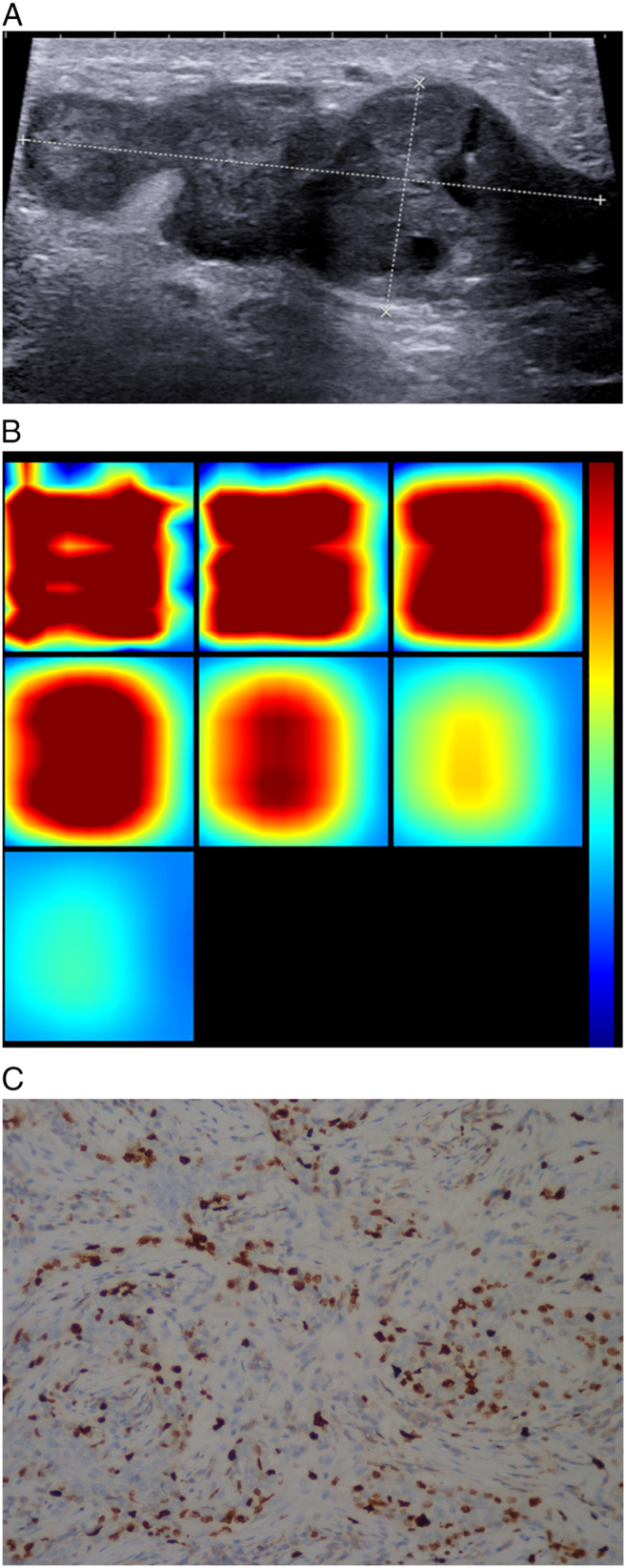
Patient age 44y, currently in the Luteal Phase, BMI22.4,pathology diagnosis of invasive ductal breast cancer, immunohistochemistry: ER-, PR-, HER -, Ki67 35%, LN -, LVI-.
(A). US 2-D imaging showing hypoechoic lesion, maximal diameter of 53 × 21 × 35 mm, irregular shape, with no circumscribed margin, heteroechoic, lesion edge-nipple distance 12 mm, lesion edge-skin surface distance 4 mm.
(B). A reconstructed optical absorption maps show that the lesion is resolved in slices from 1 to 3 (top row, left to right). THCmean was 296.1 μmol/L. The first section (slice 1, top left) is a 6 × 6 cm spatial x–y image (coronal plane of the body) obtained at a depth of 0.5 cm, as measured from the skin surface. The last section (slice 7, bottom left) is a 6 × 6 cm spatial x–y image (coronal plane of the body) obtained at a depth of 3.5 cm towards the chest wall. Spacing between sections is 0.5 cm in the direction of propagation. The vertical color scale from blue to red is the THC in micromoles per liter from low to high.
(C). Ki-67 nuclear staining (×200). The Ki-67 proliferation index is determined as 35%.