
Figure 3.
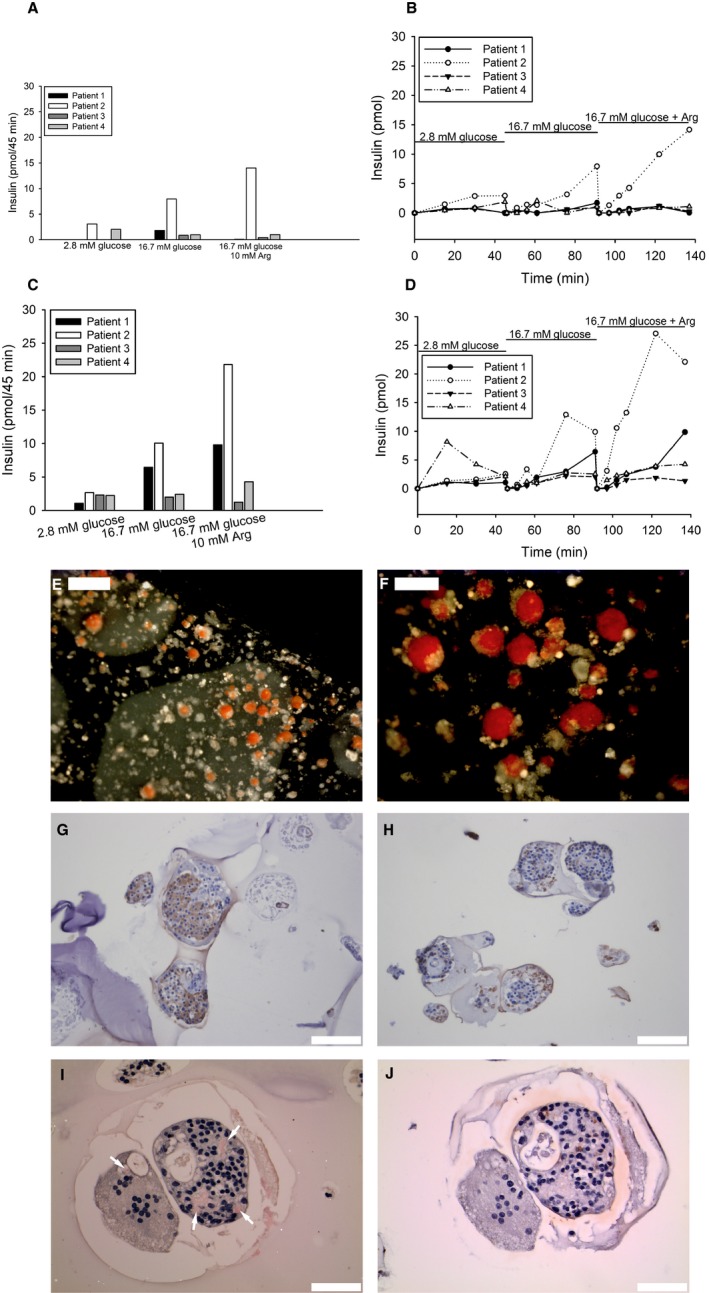
Recovered device (A‐B) and device containing slabs (C‐D) were evaluated ex vivo with respect to insulin secretion upon glucose and arginine stimulation. Insulin release was measured in 4 patients for 45 minutes at each condition (A). The dynamic insulin secretion was observed up to 135 minutes after continuous stimulation of device with low (2.8 mmol/L), high (16.7 mmol/L), and finally high glucose supplemented arginine solution (B). Insulin release was measured in slabs, recovered from the device, when stimulated with low, respectively, high glucose (2.8 vs 16.7 mmol/L) with or without arginine for 45 min (C). One slab from each patient was monitored for dynamic insulin secretion when stimulated with different concentrations of glucose (2.8 vs 16.7 mmol/L) with or without arginine (D). Separate slabs were stained with dithizone (red), and islets could easily be detected (E, scale bar 500 μm) and (F, scale bar 200 μm). Islet‐containing slabs were also further processed for immunohistochemistry and stained for insulin (brown). Insulin‐positive cells could be found in slabs from all patients (G), but also areas with fragmented islets and cellular debris were observed (H, scale bar 100 μm). Sections stained with Congo red identified amyloid‐containing islets (I, scale bar 50 μm; amyloid [red] indicated by arrows), and insulin‐positive cells (brown) were verified in consecutive sections (J, scale bar 50 μm). The left islet in (I), where a single deposit occurs, has a markedly reduced number of nucleated cells. The islet to the right contains multiple inclusions occupying almost 20% of the islet area, and the amyloid is surrounded by nucleated cells. The result suggests that amyloid formation proceeded for a long time, which requires functioning beta cells. Sections were counterstained with hematoxylin