
Fig. 1.
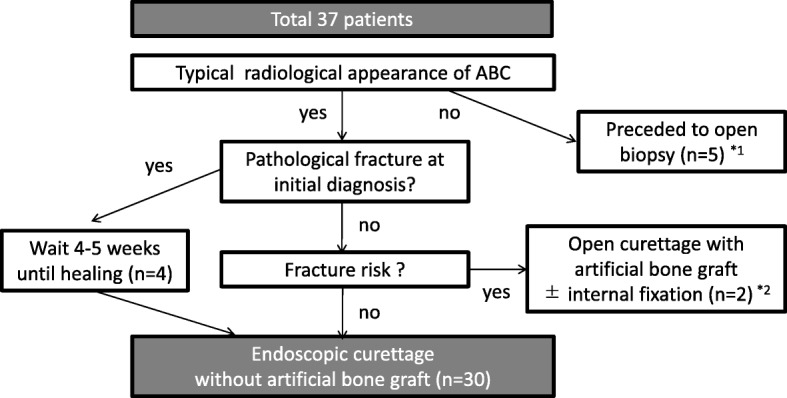
Flow diagram of patient selection for ESC treatment for ABC. For cases of atypical radiological appearance of an ABC, we proceeded with open biopsy to exclude the presence of a giant cell tumor, telangiectatic osteosarcoma, or other malignant bone tumor with a cyst. Moreover, to prevent femoral fracture after ESC, we proceeded with open curettage and artificial bone grafting, with or without internal fixation, for cases of large cystic lesions (lesion/cortex ratio > 2/3) located in the femoral trochanter (details provided in the Discussion). For ABCs at all other locations where a pathological fracture was visible at the time of the initial diagnosis, ESC was performed after bone union. Ultimately, 30 patients underwent ESC without an artificial bone graft. *1. In 5 cases, curettage with βTCP (OSferion; Olympus Co., Tokyo, Japan) was performed after intraoperative open biopsy for confirmation of ABC. This was because giant cell tumors were first suspected in 4 cases, and a cystic lesion that arose in an unusual location (clavicle) was not regarded as ABC according to the diagnosis indicated by preoperative imaging. *2: An ABC with a large cystic lesion (lesion/cortex ratio > 2/3) located in the femoral trochanter was regarded as a contraindication for ESC