

To the Editor: We present a case of pleuroperitoneal and lymph node tuberculosis (TB) whose clinical, radiological, and laboratory data could have been easily mistaken for advanced ovarian carcinoma, and then subjected to unnecessary laparotomy and surgical resections with severe consequences. Our case, a 45-year-old female, had ascites, extensive lymph adenopathy, bilateral ovarian cysts, and pleural effusion (Figures 1, 2). Biopsy of an accessible cervical lymph node revealed caseous lymphadenitis (Figure 3). With antitubercular treatment, CA-125 levels of 531 mIU/L declined to 36 mIU/L in parallel with clinical and radiological improvement (Figure 4).
Figure 1.
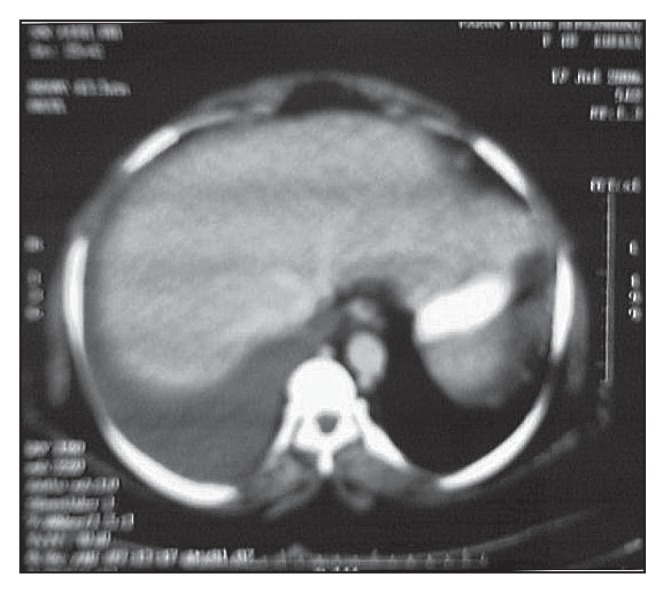
Abdominal CT scan showing ascites.
Figure 2.
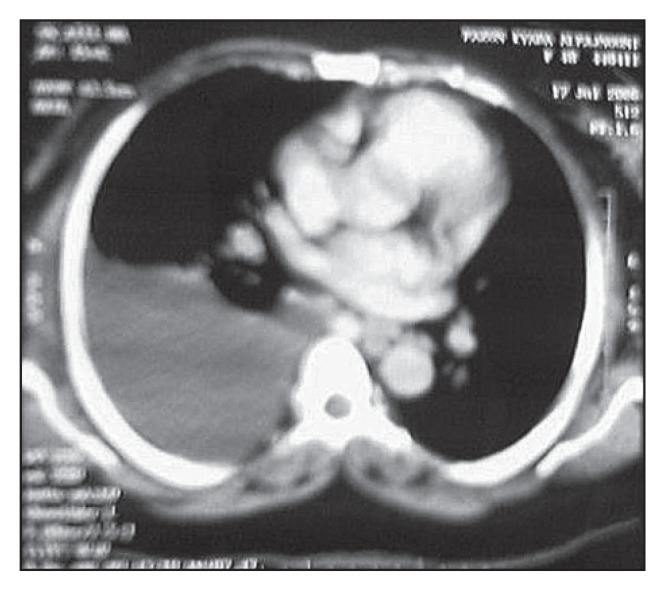
CT scan showing tuberculous pleural effusion before treatment.
Figure 3.

Low-power photomicrograph showing tubercular lymphadenitis.
Figure 4.
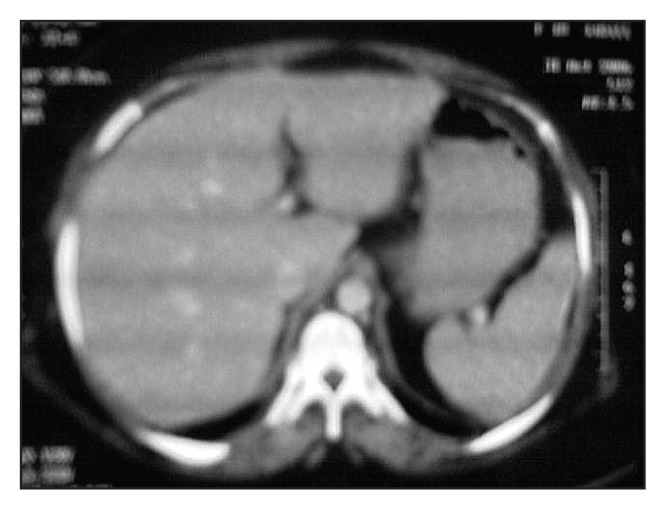
CT scan showing resolved ascites after treatment.
CA-125 is a glycoprotein of high molecular weight, which is detected by the monoclonal antibody OC125, first described by Bast et al in 1981.1 CA-125 is elevated in a variety of malignant and benign conditions,2,3 but its main clinical application is limited to diagnosis and follow-up of ovarian cancer in which only 50% of stage 1 but 80% to 85% of advanced stages have elevated CA-125.4 The titer has been used to differentiate between benign and malignant conditions,5 but very high levels (>1000 mIU/L) have been reported in benign conditions such as massive pleural effusion, ascites, and chronic liver disease.6 Elevation of CA-125 in peritoneal tuberculosis (TB) has been reported and misinterpreted as disseminated ovarian malignancy. 7 A decline of CA-125 with antitubercular drug therapy has paralleled clinical improvement, and has been advocated as a marker in the follow-up of response to treatment. 8,9
Although false positivity with CA-125 is high and specificity and sensitivity are poor,10 elevated levels in a clinical setting of ovarian carcinoma must be taken with caution to avoid unnecessary laparotomies and even extensive surgical resection of pelvic masses.11,12 Thus, it is evident from our case that not only can an elevated CA-125 level be useful in considering the presence of a non-malignant condition like TB, especially in our part of the world, but can also be used as a marker for response to treatment and an indicator of the activity of a disease like TB.11
REFERENCES
- 1.Bast RC, Feeney M, Lazarus H, Nadler LM, Colvin RC, Knapp RC. Reactivity of a monoclonal antibody with human ovarian carcinoma. J Clin Invest. 1981;68:1331–7. doi: 10.1172/JCI110380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tingulstad S, Hagen B, Skjeldestad FE, Onsrud M, Kiserud T, Halvorsen T, Nustad K. Evaluation of a risk of malignancy index based on serum CA125, ultrasound findings and menopausal status in the pre-operative diagnosis of pelvic masses. Br J Obstet Gynaecol. 1996;103:826–31. doi: 10.1111/j.1471-0528.1996.tb09882.x. [DOI] [PubMed] [Google Scholar]
- 3.Meden H, Fattahi-Meibodi A. CA125 in benign gynecological conditions. Int J Biol Markers. 1998;13:231–7. doi: 10.1177/172460089801300411. [DOI] [PubMed] [Google Scholar]
- 4.Duffy MJ, Bornberer JM, Kulpa J, et al. CA125 in ovarian cancer. European group on tumor markers (EGTM) guideline for clinical use. Int J Gynecoloncol. 2005 doi: 10.1111/j.1525-1438.2005.00130.x. [AUTHOR: Complete authors and volume and page nos.] [DOI] [PubMed] [Google Scholar]
- 5.Le Thi Huong D, Mohattane H, Piette JC, Bogdan A, Auzeby A, Touitou Y, Godeau P. [Specificity of CA-125 tumor marker. A study of 328 cases of internal medicine]. Presse Med. 1988;17:2287–91. Article in French 3. [PubMed] [Google Scholar]
- 6.Hussain SF, Grayez J, Grigorian A, Green JT. Massive pleural effusion and marked increase of CA125. Postgrad Med J. 2004;80:300–1. doi: 10.1136/pgmj.2003.012377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Straugon JM, Robertson MW, Partridge EE. A patient with a pelvic mass, elevated CA-125 and fever. Gynecol Oncol. 2000;77:471–2. doi: 10.1006/gyno.2000.5756. [DOI] [PubMed] [Google Scholar]
- 8.Mansour M, Linden ER, Colby S, Posner G, Marsh F., Jr Elevation of carcinoembryonic antigen and CA-125 in a patient with multivisceral tuberculosis. J Natl Med Assoc. 1997;89:142–3. [PMC free article] [PubMed] [Google Scholar]
- 9.Thakur V, Mukerjee U, Kumar K. Elevated serum cancer antigen levels in advanced abdominal tuberculosis. Med Oncol. 2001;18:289–91. doi: 10.1385/MO:18:4:289. [DOI] [PubMed] [Google Scholar]
- 10.Lantheaume S, Soler S, Issartel B, Isch JF, Lacassin F, Rougier Y, Tabaste JL. [Peritoneal tuberculosis simulating advanced ovarian carcinoma: a case report]. Gynecol Obstet Fertil. 2003;31:624–6. doi: 10.1016/s1297-9589(03)00179-6. Article in French. [DOI] [PubMed] [Google Scholar]
- 11.Yilmaz A, Ece F, Bayramgürler B, Akkaya E, Baran R. The value of CA-125 in the evaluation of tuberculosis activity. Respir Med. 2001;95:666–9. doi: 10.1053/rmed.2001.1121. [DOI] [PubMed] [Google Scholar]
- 12.Piura B, Rabinovich A, Leron E, Yanai-Inbar I, Mazor M. Peritoneal tuberculosis-an uncommon disease that may deceive the gynecologist. Eur J Obestet Gynecol Reprod Biol. 2003;110(2):230–4. doi: 10.1016/s0301-2115(03)00101-5. [DOI] [PubMed] [Google Scholar]