
Figure 2.
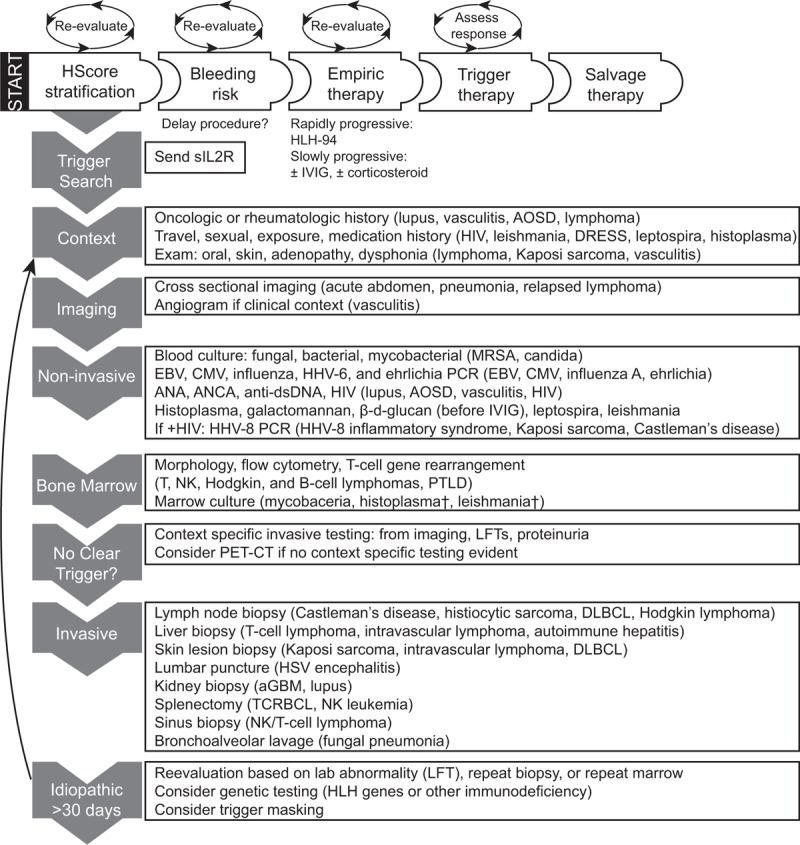
Evidence-based diagnostic and therapeutic strategies for adult HLH. Evaluation begins with HScore stratification. Assessment for bleeding risk, empiric therapy, and triggers occur simultaneously. Periodic reassessment of each factor is warranted as clinical course develops, as indicated by circular arrows. Trigger search proceeds through high-yield, low risk interventions to interventions with lower utility and increased risk of bleeding (grey arrows on left sidebar). Contributory findings are listed with triggers from our cohort (63 cases by HLH-2004 criteria, 13 cases by HScore). If no trigger is found, reassessment is warranted with consideration of expanded testing and repeat biopsy (black arrow). Note that IVIG leads to false positive β-d-glucan testing that may lead to prolonged antifungal therapy if misinterpreted. †Subsequently detected by non-invasive testing. aGBM = anti-glomerular basement membrane disease, AOSD = adult onset Still disease, CMV = cytomegalovirus, DLBCL = diffuse large B-cell lymphoma, DRESS = drug reaction with eosinophilia and systemic symptoms, EBV = Epstein–Barr virus, HHV = human herpes virus, HIV = human immunodeficiency virus, HSV = herpes simplex virus, IVIG = intravenous gamma globulin, LFT = liver function tests, MRSA = methicillin resistant staphylococcus aureus, NK = natural killer cell, PCR = polymerase chain reaction, PTLD = post-transplant lymphoproliferative disease, sIL2R = soluble interleukin-2 receptor, TCRBCL = T-cell rich large B-cell lymphoma.