
Figure 1. Six representative examples of activity‐dependent spinal cord plasticity. A–C, three examples illustrating spinal cord plasticity in pathological situations or in reduced preparations; D–F, three examples illustrating spinal cord plasticity in normal life.
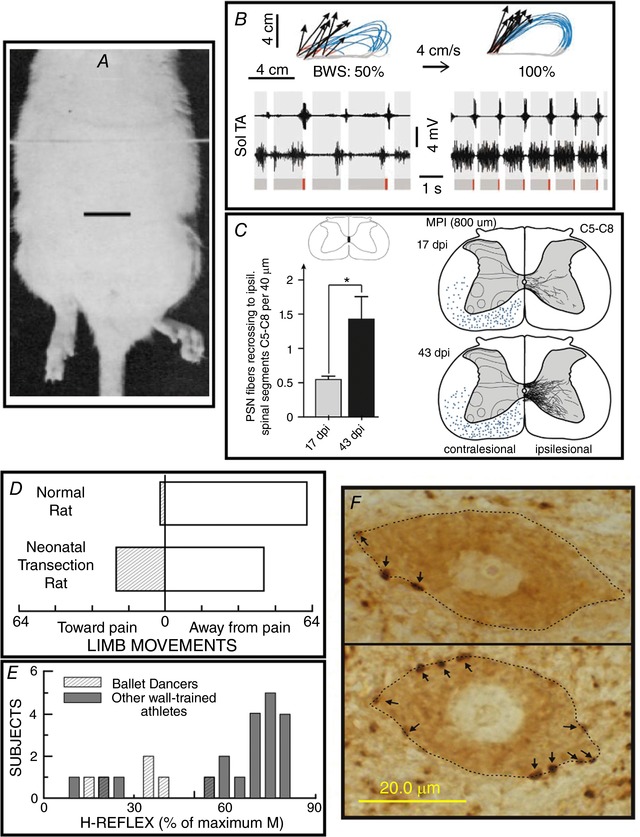
A, a hindlimb postural asymmetry produced by a unilateral cerebellar lesion persists after complete transection of the thoracic spinal cord. The cerebellar lesion occurred 60 min prior to the spinal cord transection. Scale bar, 2 cm. Modified from Chamberlain et al. (1963). B, impact of a combined treatment of serotonergic agonists, epidural electrical stimulation and locomotor training on treadmill locomotion (i.e. at 4 cm s−1) in spinal cord‐transected rats. Data from an untreated and a treated rat are shown on the left and right, respectively. Top: limb end‐point trajectories (with red indicating the initial drag phase of swing) and vectors representing the direction and magnitude of limb end‐point velocity at swing onset. The rat's percentage of body weight support (BWS) is indicated. Bottom: sequences of EMG activity from tibialis anterior (TA) and soleus (Sol) muscles. Grey and red bars indicate the stance and drag phases, respectively. Locomotion is far more normal, effective and consistent in the treated rat. Modified from Courtine et al. (2009), Nature Publishing Group, with permission. C, in the weeks following a C4 spinal hemisection in a rat, ipsilateral propriospinal neurons located above the lesion send axons into the contralateral spinal cord that descend to below the lesion and recross the midline at C5–8 to make functional connections. Left: the number of recrossing fibres increases greatly from 17 to 43 days post‐injury (dpi). Right: illustration of the marked increase in labelled recrossing fibres from 17 to 43 dpi. From Filli et al. (2014), Society for Neuroscience, with permission. D, the direction of flexion withdrawal responses to painful stimuli in normal adult rats and in adult rats in which the spinal cord was transected just after birth. In normal adults, the direction of the response is almost always correct (i.e. the limb moves away from the painful stimulus), while in transected adults it is often incorrect (i.e. the limb moves towards the stimulus). Neonatal spinal cord transection abolishes the descending input that gradually shapes normal (i.e. correct) flexion withdrawal responses. Modified from Levinsson et al. (1999), Society for Neuroscience, with permission. E, soleus H‐reflexes are much smaller in professional ballet dancers than in other well‐trained athletes (e.g. runners, swimmers and cyclists). (H‐reflexes of sedentary subjects fall in between.) The dancers’ smaller reflexes appear to be an important component of their skill acquisition. Modified from Nielsen et al. (1993), Springer Publishing, with permission. F, soleus motoneurons (dotted lines) from a control rat (top) and a rat in which the soleus H‐reflex was reduced by an operant down‐conditioning protocol (bottom). Arrows point to GABAergic terminals on the somatic membrane. The terminals are identified by glutamic acid decarboxylase (GAD67) immunoreactivity. After down‐conditioning, soleus motoneurons have many more GABAergic terminals, and these terminals are more densely labelled and cover more of the somatic membrane. The increase in GABAergic terminals is likely to be a component of the spinal cord plasticity that produces the smaller H‐reflex. Scale bar, 20 µm. From Wang et al. (2006), Wiley, with permission.