

Abstract
Background:
Endometriosis is one of the common causes of infertility with very diverse etiology. In modern lifestyle, humans are exposed to several endocrine-disrupting chemicals (EDCs) which may lead to reproductive disturbances. Diethyl hexyl phthalate (DEHP) is one of the common EDCs to which women are exposed by the use of cosmetics, perfumes, food packaging, medicine, and insecticides.
Aim:
The aim of this study was to measure the levels of DEHP in women diagnosed with endometriosis and healthy females and to compare these levels among different stages of endometriosis.
Setting and Design:
This descriptive study was conducted at a tertiary care hospital.
Subjects and Methods:
This study comprised of fifty women diagnosed with endometriosis, aged 20–40 years, and fifty age-matched healthy, fertile women without endometriosis. Females on any medication/comorbid conditions were excluded from the study. Serum DEHP concentrations were measured by high-performance liquid chromatography (HPLC). The results were expressed as means ± standard deviation (SD) (ng/ml of DEHP).
Statistical Analysis:
Data were analyzed using IBM-SPSS version 20. Two-sample Student's t-test and one-way ANOVA were applied for the analysis.
Results:
The mean ± SD value of DEHP in cases was 65.29 ± 21.69 ng/ml; however, the mean ± SD value of DEHP in controls was undetectable. Comparison of DEHP among stages of endometriosis revealed an increasing trend with advanced stages (III and IV). The values were not different between the two age groups of women with endometriosis (20–30 and 31–40 years).
Conclusion:
High levels of DEHP in women diagnosed with endometriosis suggest a role of phthalates in the etiology of endometriosis and permit careful use of such compounds.
KEYWORDS: Diethyl hexyl phthalate, endometriosis, infertility, phthalates
INTRODUCTION
Endometriosis is defined as the presence of ectopic endometrial tissue.[1] It is a disease of reproductive age group associated with poor quality of life[2] and higher incidence of subfertility/infertility.[3] Approximately 15% of industrialized world population is affected by infertility.[4] Endometriosis is one of the common causes of infertility.[5] Frequency of the disease has been reported to be 16.8% in primary infertility cases.[6] This is in congruous with findings of other studies done on different populations.[7,8] Apart from infertility, endometriosis is also associated with severe pelvic discomfort, stress, disruption of social activities, and possible adverse outcomes of assisted reproduction.[9] Emerging evidence suggests a possible role of ubiquitous environmental contaminants in the physiopathology of endometriosis.[10,11,12] In particular, phthalates, a class of widespread environmental contaminants, have been postulated to be linked to endometriosis[10,13] and infertility in animal models.[14]
Phthalate esters, commonly known as plasticizers, are used to increase flexibility, durability, transparency, and longevity of different substances. They are used in many consumer products including household furnishing, cosmetics, perfumes, food packaging, medicine, and insecticides. They also possess endocrine-disrupting properties.[11] Long-term exposure to these esters, especially diethyl hexyl phthalate (DEHP), which is widely spread, has shown to induce reproductive problems in humans, both in males and females.[12] Human exposure to DEHP is primarily through processed food, contaminated from food processing machines and packaging materials and dermal application of personal care and cosmetic products.[15]
Studies revealed that the plasma and urinary levels of DEHP and its metabolites are significantly elevated in women with endometriosis compared with controls, suggesting a possible role for phthalate esters in the pathogenesis of endometriosis.[16,17]
Levels of phthalate metabolites are considered to vary according to sociodemographic status. Easy and widespread availability of processed and packaged products and their lower cost is one of the main reasons of exposure. Emerging trends to routinely used cosmetic products and synthetic health-care products also has increased the risk of exposure to phthalates.
The toxicity of phthalates has come into the limelight from the past few decades now and the quest is to find out how these harmful chemicals may be involved in the pathophysiology of different diseases. In this context, we conducted this study in women diagnosed with endometriosis to measure the levels of DEHP in serum and to see if they differ from the healthy women.
SUBJECTS AND METHODS
A descriptive comparative study was carried out after approval by ethical review board of university. All participants gave written informed consent to participate in the study. The study population consisted of fifty diagnosed cases of endometriosis and fifty normal fertile females aged 20–40 years. Only those cases were included who were infertile and had been declared positive for endometriosis after laparoscopy by expert surgeons according to the criteria set by the American Society for Reproductive Medicine (ASRM, 2012). ASRM guidelines classify endometriosis into four stages (I – minimal, II – mild, III – moderate, and IV – severe) depending on the location, extent, and depth of endometriosis implants; presence and severity of adhesions; and presence and size of ovarian endometriomas. For controls due to ethical consideration, laparoscopy was not done. However, they were included based on certain criteria, i.e., proven fertile females who had delivered a baby in the last two years, screened negative for endometriosis by ultrasonography after detailed clinical assessment by specialized doctors, and were not on any medication, comorbid conditions, or polycystic ovarian syndrome. Relevant information (name, age, address, etc.) was obtained and a detailed medical history with general physical and systemic examination was done.
Blood samples from cases were collected after laparoscopy when the patients were declared positive for endometriosis. Venous blood was drawn from cases and controls and was treated similar way for serum separation, storage, and analysis both in cases and controls. Glass vacutainer tubes and vials were used instead of plastic tubes to prevent possible contamination. A 10-ml sample of blood was collected under aseptic measures. Serum was separated, aliquoted, and stored at −80°C for subsequent analysis. High-performance liquid chromatography (HPLC) (Perkin Elmer Life and Analytical Sciences, Shelton, CT, USA) was used to determine DEHP concentrations. Stock solution of 99.99% DEHP, HPLC grade, was purchased from Merck chemicals, Germany, and its internal standards were prepared in acetonitrile (HPLC grade, Sigma Aldrich, USA) purchased from Fisher scientific, Germany, and stored at −20°C to test linearity. Calibrators were prepared in serum 10, 50, 100, 250, 500, and 1000 ng/ml by adding suitable quantities of DEHP stock solutions. 200 μL of serum was added with 50 μL of internal standard, 400 μL of 1 mol/L NaOH (HPLC grade, Sigma Aldrich, USA), 100 μL of 50% H3 PO4 (HPLC grade; Sigma Aldrich USA), and 600 μL of 50% acetonitrile (Fisher Scientific GmbH, Schwerte, Germany).
After centrifugation for 10 min at 1500 rmp, the supernatant was separated and 10 μL of the supernatant was injected into the liquid chromatography glass vials through a syringe filter (25 mm/0.22 μm) and placed into an autosampler (Perkin Elmer series 200).
To prevent possible contamination, all glass vials were washed with methanol, acetone, and acetonitrile. HPLC was carried out using Perkin Elmer series 200 UV pump attached to a Diode Array UV/visible Perkin Elmer series 200 detector. A Perkin Elmer 250 mm × 4.6 mm (internal diameter) Brownlee analytical C18 (5-μm particle size) column (Hanover Park, IL, USA) was used. Results were analyzed on Total chrome Navigator 3.1.5 software (Perkin Elmer Life and Analytical Sciences, Shelton, CT, USA). The mobile phase consisted of a mixture of 1 ml/L acetic acid (Sigma Aldrich, USA) in water and 1 ml/L acetic acid in acetonitrile (10/90, vol/vol).
Elution was performed with the use of an isocratic mode at 0.5 ml/min. Total chromatographic run time was 10 min. Peak for DEHP was obtained at 6.08 min (retention time). Concentration of DEHP was calculated using straight line equation.
Statistical analysis
Data were analyzed using IBM-SPSS version 20 (Armonk, NY, USA). The variables were analyzed and described as means (±standard deviation [SD]). Two-sample Student's t-test was applied to compare the concentrations of phthalate esters in both groups (cases and controls). P ≤ 0.05 was considered statistically significant. One-way ANOVA was applied to compare the different stages of endometriosis.
RESULTS
Calculation of mean values of diethyl hexyl phthalate
Individual values for DEHP were calculated using straight line equation between peak area of standard and concentration of standard and placing individual peak areas for cases and controls in straight line equation, as shown in Figure 1.
Figure 1.
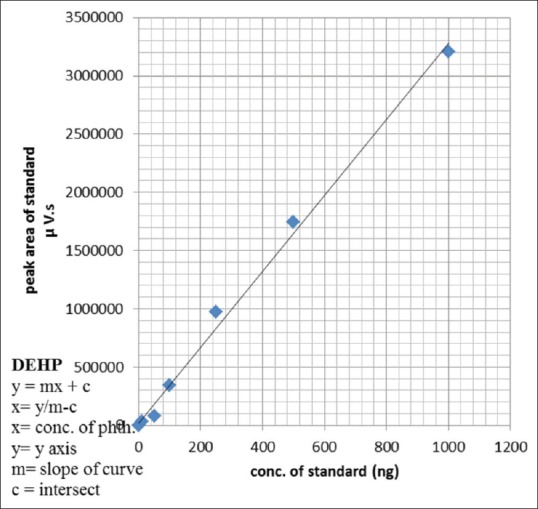
Straight line equation of diethyl hexyl phthalate according to least square method for calculating values in both cases and controls
Real-time high-performance liquid chromatography chromatographs
Figures 2a, b and 3a, b represent DEHP chromatographs obtained through HPLC in cases and controls, respectively. The X-axis represents the retention time and Y-axis represents absorbance (mau). The retention time for DEHP was found to be 6.07 min. Figure 2a is the real-time chromatograph, showing the peaks of DEHP, while Figure 3a depicts no peak of DEHP on its respective retention time. Figures 2b and 3b are reprocess results obtained from Total chrome navigator 3.1.5 software, Figure 2b shows DEHP peak area recorded at 6.07 min in cases, whereas 3b depicts no DEHP peak area in control group at respective retention time.
Figure 2.
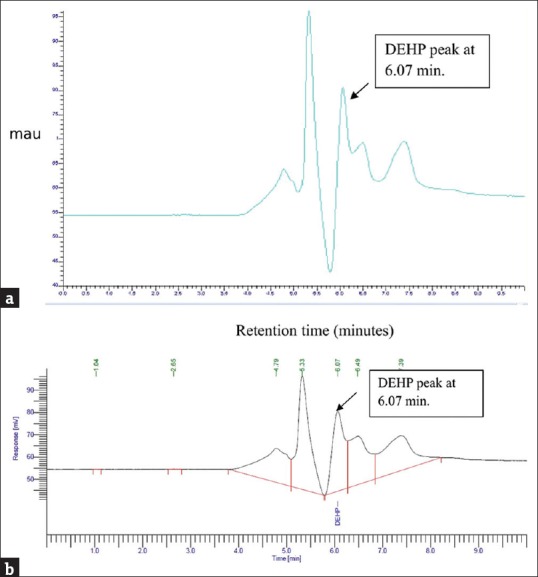
(a) Real-time chromatograph of high-performance liquid chromatography of cases showing diethyl hexyl phthalate peaks. Generated from Total Chrome Navigator 3.1.5 software. (b) Reprocess chromatograph of high-performance liquid chromatography of cases showing diethyl hexyl phthalate peak. Generated from Total Chrome Navigator 3.1.5 software
Figure 3.
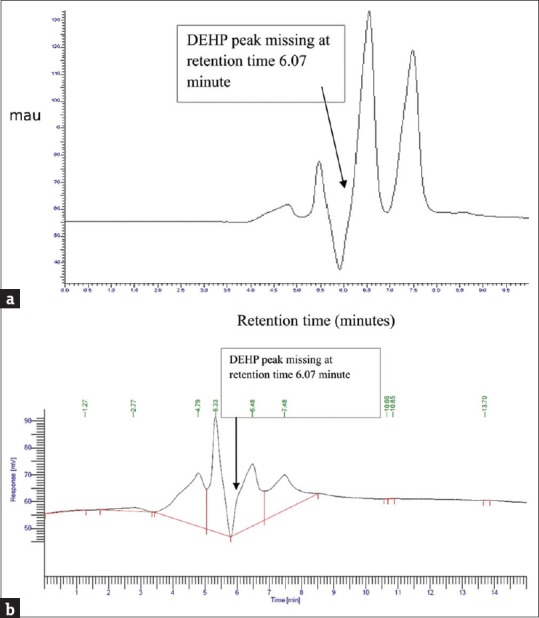
(a) Real-time chromatograph of high-performance liquid chromatography of controls depicting the absence of diethyl hexyl phthalate peak at respective retention time. Generated from Total Chrome Navigator 3.1.5 software. (b) Reprocess chromatograph of high-performance liquid chromatography depicting the absence of diethyl hexyl phthalate peak at respective retention time. Generated from Total Chrome Navigator 3.1.5 software
Mean diethyl hexyl phthalate values
The overall mean (±SD) levels of DEHP in cases and controls are summarized in Table 1. Comparison of DEHP means among different stages of endometriosis is summarized in Table 2. Age-specific DEHP mean values are represented in Figure 4.
Table 1.
Comparison of mean diethyl hexyl phthalate between cases and controls

Table 2.
Comparison of mean±standard deviation diethyl hexyl phthalate values in all the four stages of endometriosis (mean±standard deviation)
![]()
Figure 4.
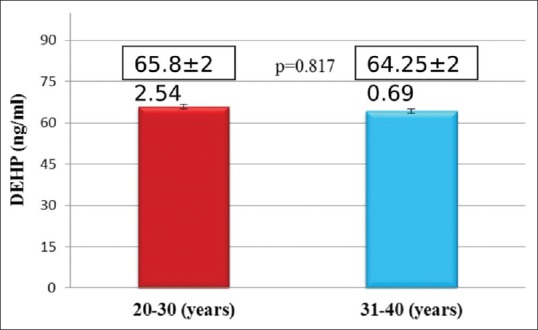
Age-specific mean diethyl hexyl phthalate values in females with endometriosis
DISCUSSION
Endometriosis is a common gynecological disease that causes intractable pelvic pain and infertility in millions of women in their reproductive years. DEHP, which is the most commonly used plasticizer, has been relatively more thoroughly researched than the other phthalates.
Our HPLC analysis of DEHP revealed a mean value of 65.29 ± 21.69 ng/ml in cases. However, the DEHP levels in controls were not detected. Higher levels of DEHP (179.7 ± 32.5 ng/ml, 2.15 ± 1.99 μg/ml, and 0.57 μg/ml) in endometriotic females have been reported by several other researchers.[16,17,18] We were able to detect DEHP levels in all cases of endometriosis (100%), while previous authors report detection of DEHP in 91.4% of cases.[17]
Similarly, Upson et al.[18] detected DEHP levels in majority of the studied population but not in all patients. In the present study, the undetectable levels of DEHP in controls raise a question of either error in extraction or cleaning of serum. The chances of error are excluded because the serum samples of cases as well as controls were run at the same time and in the same batch, by one operator. Therefore, this possibility is ruled out because the machine was able to detect the levels of DEHP in cases. The other likelihood may be that the levels of DEHP in controls were below the sensitivity of the method employed (Food and Drug Administration, 2012). Contrary to our results, Rozati et al.[19] detected DEHP levels in all controls. However, they report very low levels (0.11 μg/ml) of DEHP in controls compared to 2.15 μg/ml in cases, which shows a 20-time lower concentration of DEHP in controls. Another reason for this discrepancy could be the retention time. The retention time for DEHP in Rozati et al's.[19] study was 20.2 min which is much higher than ours (6.07 min). The column used in the study by Rozati et al.[19] was 4 mm × 220 mm Partisil 5 silica column as compared to ours, which was 250 mm × 4.6 mm (internal diameter) Brownlee analytical C18 (5-μm particle size) column. Specification of HPLC machine used in that study was Shimadzu SCL-6A system controller (Nakagyo-ku, Kyoto, Japan) and Shimadzu SPD-6AV UV-Vis spectrophotometric detector equipped with a C-R6A Chromatopac as compared to ours, which was Perkin Elmer series 200 UV pump attached to a Diode Array UV/visible Perkin Elmer series 200 detector; the likelihood of difference in results may be due to the difference in HPLC machine and detector specifications. Another possible reason may be the levels, activity, or polymorphism of glutathione-S-transferase enzyme, which is the major detoxification enzyme for phthalates, especially DEHP, in patients with endometriosis.[20] DEHP is a parent compound which is metabolized in body into its metabolites such as monoethyl hexyl phthalate by glutathione S-transferase and P450 enzyme system.[21] Therefore, in controls, this enzyme was working properly degrading the DEHP into other metabolites, which were not targeted in the present study. On the other hand, it is speculated that in endometriotic cases, the function of glutathione S-transferase and P450 enzyme system was compromised or its half-life is increased; therefore, DEHP was not further metabolized and was easily detected. If confirmed, it can be speculated that the levels of DEHP may be used in the screening of endometriosis. However, before drawing any tangible conclusions, these points warrant further detailed investigations.
When interstage comparison of DEHP levels was drawn, no significant difference was observed between the stages of endometriosis [Table 2]. However, an increasing trend in mean DEHP values was observed with advancement of disease stage in this study. Others have reported the results of higher DEHP levels and severity of the disease. For example, higher concentrations (179.7 ± 32.5 ng/ml) of DEHP (P = 0.01) were found in 97 women with endometriosis compared to 169 controls (92.5 ± 31.1), and exposure to DEHP was correlated with the severity of endometriosis.[22] The likelihood may be that the number of cases was more as compared to the present study.
In the present study, the level of serum DEHP results in cases was supported by several previous studies from various places and carried out on serum, urine, and blood plasma in endometriotic patients compared to controls.[16,17,18,22] Furthermore, Durmaz et al.[23] reported that plasma DEHP and monoethylhexyl phthalate levels were higher in a group with pubertal gynecomastia and suggested that phthalate exposure might lead to abnormal reproductive development resulting from possible estrogenic and antiandrogenic activities of these compounds.[23]
CONCLUSION
Taken together, our results show positive association of phthalates with endometriosis in local population. Due to study limitations, we could not expand our experiments to detect the metabolites of DEHP which may give more detailed insight about the possible role of these compounds in the pathophysiology of endometriosis. We are planning to conduct larger studies in the future to overcome the limitations of the study.
Financial support and sponsorship
This study was financially supported by the University of Health Sciences, Lahore, Pakistan.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors extend their sincere thanks to all the team members and women who participated in the study.
REFERENCES
- 1.Diamanti-Kandarakis E, Bourguignon JP, Giudice LC, Hauser R, Prins GS, Soto AM, et al. Endocrine-disrupting chemicals: An endocrine society scientific statement. Endocr Rev. 2009;30:293–342. doi: 10.1210/er.2009-0002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nnoaham KE, Hummelshoj L, Webster P, d'Hooghe T, de Cicco Nardone F, de Cicco Nardone C, et al. Impact of endometriosis on quality of life and work productivity: A multicenter study across ten countries. Fertil Steril. 2011;96:366–73.e8. doi: 10.1016/j.fertnstert.2011.05.090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Strathy JH, Molgaard CA, Coulam CB, Melton LJ., 3rd Endometriosis and infertility: A laparoscopic study of endometriosis among fertile and infertile women. Fertil Steril. 1982;38:667–72. doi: 10.1016/s0015-0282(16)46691-4. [DOI] [PubMed] [Google Scholar]
- 4.Cramer DW, Missmer SA. The epidemiology of endometriosis. Ann N Y Acad Sci. 2002;955:11–22. doi: 10.1111/j.1749-6632.2002.tb02761.x. [DOI] [PubMed] [Google Scholar]
- 5.Crinnion WJ. Toxic effects of the easily avoidable phthalates and parabens. Altern Med Rev. 2010;15:190–6. [PubMed] [Google Scholar]
- 6.Drbohlav P, Jirsová S, Masata J, Jech L, Bencko V, Omelka M, et al. Relationship between the levels of toxic polychlorinated biphenyls in blood and follicular fluid of sterile women. Ceska Gynekol. 2005;70:377–83. [PubMed] [Google Scholar]
- 7.Evers JL. Female subfertility. Lancet. 2002;360:151–9. doi: 10.1016/S0140-6736(02)09417-5. [DOI] [PubMed] [Google Scholar]
- 8.Farquhar CM. Extracts from the “clinical evidence”.Endometriosis. BMJ. 2000;320:1449–52. doi: 10.1136/bmj.320.7247.1449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Buck Louis GM, Peterson CM, Chen Z, Croughan M, Sundaram R, Stanford J, et al. Bisphenol A and phthalates and endometriosis: The endometriosis: Natural history, diagnosis and outcomes study. Fertil Steril. 2013;100:162–90. doi: 10.1016/j.fertnstert.2013.03.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rier S, Foster WG. Environmental dioxins and endometriosis. Toxicol Sci. 2002;70:161–70. doi: 10.1093/toxsci/70.2.161. [DOI] [PubMed] [Google Scholar]
- 11.Latini G. Monitoring phthalate exposure in humans. Clin Chim Acta. 2005;361:20–9. doi: 10.1016/j.cccn.2005.05.003. [DOI] [PubMed] [Google Scholar]
- 12.Lyche JL, Gutleb AC, Bergman A, Eriksen GS, Murk AJ, Ropstad E, et al. Reproductive and developmental toxicity of phthalates. J Toxicol Environ Health B Crit Rev. 2009;12:225–49. doi: 10.1080/10937400903094091. [DOI] [PubMed] [Google Scholar]
- 13.Pauwels A, Schepens PJ, D'Hooghe T, Delbeke L, Dhont M, Brouwer A, et al. The risk of endometriosis and exposure to dioxins and polychlorinated biphenyls: A case-control study of infertile women. Hum Reprod. 2001;16:2050–5. doi: 10.1093/humrep/16.10.2050. [DOI] [PubMed] [Google Scholar]
- 14.Schmidt JS, Schaedlich K, Fiandanese N, Pocar P, Fischer B. Effects of di(2-ethylhexyl) phthalate (DEHP) on female fertility and adipogenesis in C3H/N mice. Environ Health Perspect. 2012;120:1123–9. doi: 10.1289/ehp.1104016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kavlock R, Boekelheide K, Chapin R, Cunningham M, Faustman E, Foster P, et al. NTP center for the evaluation of risks to human reproduction: Phthalates expert panel report on the reproductive and developmental toxicity of di-n-butyl phthalate. Reprod Toxicol. 2002;16:489–527. doi: 10.1016/s0890-6238(02)00033-3. [DOI] [PubMed] [Google Scholar]
- 16.Reddy BS, Rozati R, Reddy BV, Raman NV. Association of phthalate esters with endometriosis in Indian women. BJOG. 2006;113:515–20. doi: 10.1111/j.1471-0528.2006.00925.x. [DOI] [PubMed] [Google Scholar]
- 17.Cobellis L, Latini G, De Felice C, Razzi S, Paris I, Ruggieri F, et al. High plasma concentrations of di-(2-ethylhexyl)-phthalate in women with endometriosis. Hum Reprod. 2003;18:1512–5. doi: 10.1093/humrep/deg254. [DOI] [PubMed] [Google Scholar]
- 18.Upson K, Sathyanarayana S, De Roos AJ, Thompson ML, Scholes D, Dills R, et al. Phthalates and risk of endometriosis. Environ Res. 2013;126:91–7. doi: 10.1016/j.envres.2013.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Rozati R, Simha B, Bendi N, Sekhar C. Evaluation of the phthalate esters in South Indian women with endometriosis. Int J Fertil Steril. 2008;1:165–70. [Google Scholar]
- 20.Huang PC, Tsai EM, Li WF, Liao PC, Chung MC, Wang YH, et al. Association between phthalate exposure and glutathione S-transferase M1 polymorphism in adenomyosis, leiomyoma and endometriosis. Hum Reprod. 2010;25:986–94. doi: 10.1093/humrep/deq015. [DOI] [PubMed] [Google Scholar]
- 21.Wang IJ, Karmaus WJ. Oxidative stress-related genetic variants may modify associations of phthalate exposures with asthma. Int J Environ Res Public Health. 2017;14 doi: 10.3390/ijerph14020162. pii: E162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kim SH, Chun S, Jang JY, Chae HD, Kim CH, Kang BM, et al. Increased plasma levels of phthalate esters in women with advanced-stage endometriosis: A prospective case-control study. Fertil Steril. 2011;95:357–9. doi: 10.1016/j.fertnstert.2010.07.1059. [DOI] [PubMed] [Google Scholar]
- 23.Durmaz E, Ozmert EN, Erkekoglu P, Giray B, Derman O, Hincal F, et al. Plasma phthalate levels in pubertal gynecomastia. Pediatrics. 2010;125:e122–9. doi: 10.1542/peds.2009-0724. [DOI] [PubMed] [Google Scholar]