

Abstract
Background:
Evidence of relationship between selenium and prostate cancer has been inconsistent. The present meta-analysis was conducted to determine relationship between selenium and prostate cancer.
Methods:
A systematic review and meta-analysis was carried out using preferred reporting items for systematic reviews and meta-analysis (PRISMA). We searched PubMed, Scopus, Web of Science, ScienceDirect, Embase, CINAHL, Cochrane Library, EBSCO and Google scholar search engines and the reference lists of the retrieved papers for relevant data, without any limitation regarding language or time until 2016. Heterogeneity among studies was evaluated using Q test and I2 Index. Finally, a random effects model was used for combining results using STATA software version 11.1. P<0.05 was considered significant.
Results:
Thirty-eight studies including 36,419 cases and 105,293 controls were included in the final analysis. The pooled relative risk (RR) of relation between selenium and prostate cancer was 0.86 (95% Confidence Interval [CI]:0.78-0.94). Sub-group analyses based on case-control, cohort, and RCT studies gave values of 0.89 (95% CI: 0.80-1.00), 0.77 (95% CI: 0.52-1.14) and 0.90 (95% CI: 0.74-1.09), respectively. RRs based on serum, plasma and nail samples were 0.69 (95% CI: 0.51-0.95), 0.85 (95% CI: 0.61-1.17), 0.66 (95% CI: 0.41-1.05), respectively. According to 10 studies, investigated the relation between advanced prostate cancer and selenium in which the RR was 0.67 (95% CI: 0.52-0.87).
Conclusions:
This meta-analysis indicated that selenium most probably has a protective role against development of prostate cancer and its progression to advanced stages. Therefore, selenium supplementation can be proposed for prevention of prostate cancer.
Keywords: Selenium, prostate cancer, meta-analysis
Introduction
Prostate cancer is the most common type of cancer worldwide. The estimates by World Health Organization (WHO) show the yearly incident cases and death cases of prostate cancer in worldwide are 1,100,000 and 307,000, respectively (Humphrey and Schuz, 2014). These estimations for the United States are 181,000 incident cases and 26,100 death cases (Siegel et al., 2016). The lifetime risk of this cancer for American men is 1 in 6 men (Siegel et al., 2011).
Given the importance of prostate cancer in terms of morbidity and mortality, many studies tried to identify risk factors for developing prostate cancer in order to prevent and control it. Several risk factors have been identified for prostate cancer such as age, race, nationality, family history of prostate cancer and insulin growth factor (Grönberg, 2003) and there is a significant difference in predisposition to prostate cancer in different countries (Miller, 2012). Intense changes in lifestyle may influence the progression of low grade and early prostate cancer (Ornish et al., 2005). One of the factors investigated by the studies is selenium. Although many studies investigated the relation between selenium and prostate cancer, there is no consensus on it, and results obtained by these studies show inconsistency. When there is the inconsistency, one of the best strategies to understand and find the conclusion is to conduct a systematic review and meta-analysis (Sayehmiri et al., 2015; Azami et al., 2017; Moher et al., 2009).
Virtamo (1987) study found no association between serum level of selenium and the prospective risk of cancer. A study by Lippman et al., (2009) show that selenium alone or in combination with vitamin E doesn’t prevent prostate cancer. A cohort study using toenail sample confirmed the protective role of selenium in prostate cancer (Van den Brandt et al., 2003). Study of Chan et al., (2009) showed a slight increase by presenting with aggressive disease in higher plasma level of selenium. In a cohort study on cancer mortality in northern Italy in an area with unusually high selenium content tap water, we did not find strong results to support the protective role of selenium supplements on cancer mortality (Vinceti et al., 1995). Meta-analysis is one of the best strategies to find the consensus between studies and is a statistical technique for combining the results of two or more different studies to find a single result (Sayehmiri et al., 2015; Azami et al., 2017; Moher et al., 2009).
Considering the importance of prostate cancer and several studies investigating the relationship between prostate cancer and selenium and lack of consensus between their results, we conducted a study based on systematic review and meta-analysis to find this association by combing related studies and presenting a final result.
Materials and Methods
This systematic review and meta-analysis study was conducted using preferred reporting items for systematic reviews and meta-analysis (PRISMA) (Moher et al., 2009). All steps of study were conducted by two independent researchers, and the issue was resolved by a third author in cases of disagreement.
Inclusion and exclusion criteria
The Inclusion criteria were the studies about the relation between selenium and prostate cancer were published in English without time limitation. The exclusion criteria included animal studies, exposure/intervention except for selenium, results other than prostate cancer, non-related articles, review studies, case reports, and letters to the editor.
Search strategy
We searched databases such as PubMed, Scopus, Web of Science (ISI), Science Direct, Embase, CINAHL, Cochrane Library, EBSCO and Google scholar search engine using search strategies, developed for each database using MeSH keywords of “selenium”, “prostate cancer”, and “trace elements”. Moreover, we searched reference list of the retrieved papers for finding more papers. The systematic search has been conducted without any time limitation until 2016.
Study selection
Reading the title and abstract of papers, we conducted the primary screening for selecting relevant papers. Afterwards, we read the full text of the papers for study selection. The retrieved papers were collected and stored in Endnote software. The duplicated papers were excluded in this step.
Data extraction
Information on the final selected studies in the previous step, including author(s) name, country of study, year, name of journal, samples characteristics (e.g. gender, mean age and size), diagnostic criteria, relative (RR) or odds ratio (OR), confidence interval (CI), were extracted and stored in Excel program.
Statistical analysis
Pooled RRs or ORs and 95% CIs were estimated for the associations between selenium exposure and the risk of prostate cancer using a random effects model. To evaluate the heterogeneity of the studies, index were used (Deeks et al, 2011; Harbord et al., 2009). Cumulative meta-analysis was used to show the trend of effect size and effects of new studies of effect size. Subgroup analysis was done according to the country, samples (nail, blood and etc.), methods, and year. Egger’s test and funnel plot were used to check publication bias. Data were analyzed using the STATA software version 11.1. P<0.05 was considered significant.
Results
At first, 660 articles were retrieved. In the next step, 330 articles with the same title and author were excluded. Of 330 remaining articles, abstracts of all existing papers were studied and 140 irrelevant studies were excluded. Then the full text of the remaining articles has been studied to find related articles. Finally, thirty-eight articles including 36,419 cases and 105,293 controls entered the final analysis (Figure 1).
Figure 1.
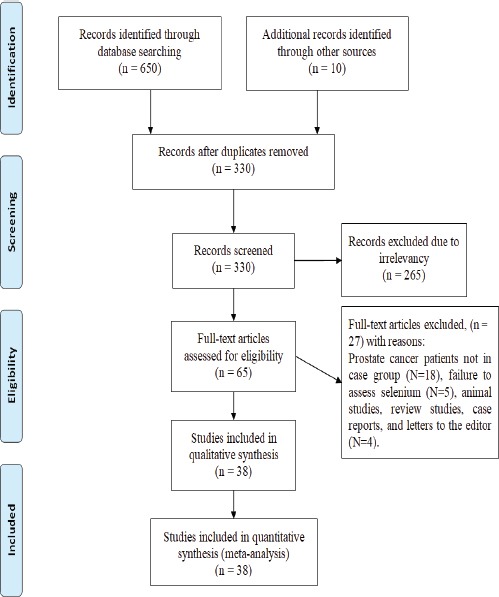
The Entrance Steps of Systematic Review and Meta- Analysis
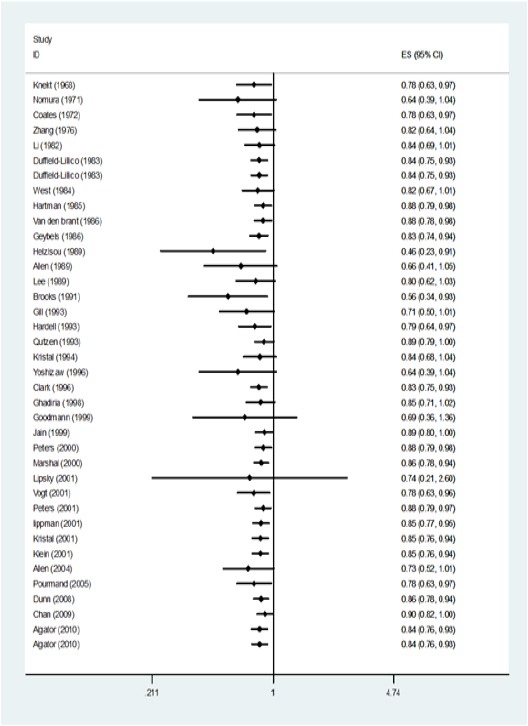
The Overall Association of Selenium and Prostate Cancer. Data analysis showed a RR of 0.86 (95% CI: 0.78-0.94) and showed the significant protective role of selenium in prostate cancer (Figure 2) Significant heterogeneity was observed (I2=69.4, P<0.001). Cumulative analysis was showed in Figure 3.
Figure 2.

Data Analysis of studies about the Relation between Selenium and Prostate Cancer. Mean point of each segment shows the estimation of Relative Risk (RR) and the length of each segment showed the 95% confidential interval in each study. The diamond mark shows the RR of each study.
Figure 3.
Cumulative Forest Plot in the Meta-Analysis of Studies about the Relation between Selenium and Prostate Cancer.
Sub-group analysis of Selenium and Prostate Cancer In subgroup analysis based on place of study, most of the studies were conducted in the USA (57.5%) and RR was 0.89 (95% CI: 0.78-1.02) (Table 2).
Table 2.
Meta-Analysis of Studies Regarding the Relationship between Selenium and Prostate Cancer Based on Country, Type of study and sample of selenium. random effects model
| Variable | Study(Na) | Case | Control | I2(%) | 95% CIb | RRc | |
|---|---|---|---|---|---|---|---|
| Country | USA | 23 | 31,691 | 70,385 | 51.6 | 0.78,1.02 | 0.89 |
| Austria | 1 | 70 | 80 | 0.21,2.60 | 0.74 | ||
| United Kingdim | 1 | 300 | 300 | 0.73,2.10 | 1.24 | ||
| Hawaii | 1 | 450 | 936 | 0.59,1.14 | 0.82 | ||
| Europe | 1 | 959 | 1,059 | 0.22,4.15 | 0.96 | ||
| China | 1 | 133 | 265 | 0.98,1.02 | 1 | ||
| Iran | 1 | 62 | 68 | 0.06,0.45 | 0.16 | ||
| Finland | 1 | 317 | 28,816 | 0.43,1.66 | 0.84 | ||
| Sweden | 1 | 164 | 121 | 0.11,0.79 | 0.3 | ||
| Denmark | 1 | 784 | 784 | 0.94,1.08 | 1.01 | ||
| Netherlands | 2 | 540 | 1,211 | 84.4 | 0.27,0.92 | 0.5 | |
| Type of study | Case-control | 19 | 8,639 | 16,967 | 59.1 | 0.80,1.00 | 0.89 |
| Cohort | 6 | 3,786 | 66,682 | 85.5 | 0.52,1.14 | 0.77 | |
| Randomized controlled trial | 9 | 23,994 | 21,644 | 54.3 | 0.74,1.09 | 0.9 | |
| Sample of selenium | Serum | 6 | 1,983 | 2,913 | 62.5 | 0.51,0.95 | 0.69 |
| Plasma | 6 | 2,982 | 2,637 | 70.1 | 0.61,1.17 | 0.85 | |
| Nail | 6 | 2,189 | 3263 | 74.8 | 0.41,1.05 | 0.66 | |
| Diet | 7 | 5,206 | 74,814 | 0 | 0.98,1.02 | 1 | |
| Selenium supplement and placebo | 9 | 23,994 | 21,644 | 54.3 | 0.74,1.09 | 0.9 |
, Number ;
, Confidence interval ;
, Relative risk
Table 1.
Data Obtained from Studies to Evaluate the Relationship between Selenium and Prostate Cncer
| Method | Authors name | Year | Place | Sample | RRa | 95% CIb |
|---|---|---|---|---|---|---|
| Case-control | Lipsky (19) | 2003 | Austria | Nail | 0.74 | 0.22-2.71 |
| Helzlsouer (20) | 2000 | USA | Nail | 0.38 | 0.17-0.85 | |
| Goodmann(21) | 2001 | USA | Serum | 1.02 | 0.65-1.60 | |
| Nomura (22) | 2000 | USA | Serum | 0.5 | 0.3-0.9 | |
| Yoshizawa (23) | 1998 | USA | Nail | 0.35 | 0.16-0.78 | |
| Brooks (24) | 2001 | USA | Plasma | 0.24 | 0.07-0.77 | |
| Allen (25) | 2004 | United k | Nail | 1.24 | 0.73-2.10 | |
| Gill (26) | 2009 | Hawaii | Serum | 0.82 | 0.59-1.14 | |
| Allen (27) | 2008 | Europe | Plasma | 0.96 | 0.07-1.31 | |
| Lee (28) | 1998 | China | Diet | 1 | 0.99-1.04 | |
| Zhang (29) | 2009 | USA | Diet | 1.3 | 0.30-5.70 | |
| Kristal (30) | 2010 | USA | Diet | 1 | 0.58-1.73 | |
| Li (31) | 2004 | USA | Plasma | 0.78 | 0.54-1.13 | |
| Ghadirian (32) | 2000 | USA | Nail | 1.14 | 0.46-2.83 | |
| Pourmand (33) | 2008 | Iran | Serum | 0.16 | 0.06-0.47 | |
| Knekt (34) | 1990 | Finland | Serum | 1.15 | ||
| Coates (35) | 1988 | USA | Serum/Plasma | 0.3 | ||
| Vogt (17) | 2003 | USA | Serum | 0.71 | 0.39-1.28 | |
| West (36) | 1991 | USA | Diet | 1.6 | 1-2.80 | |
| Hardell (37) | 1995 | Sweden | Plasma | 0.3 | 0.10-0.70 | |
| Qutzen (38) | 2016 | Danish | Plasma | 1.01 | 0.94-1.08 | |
| Jain (18) | 1999 | USA | Diet | 0.93 | 0.68-1.28 | |
| Cohort | Van den brant (9) | 2003 | Netherlands | Nail | 0.69 | 0.48-0.99 |
| Hartman (39) | 1998 | Finland | Diet | 0.84 | 0.43-1.67 | |
| Peters (40) | 2008 | USA | Diet | 0.9 | 0.62-1.30 | |
| Peters (41) | 2007 | USA | Serum | 0.84 | 0.62-1.14 | |
| Chan (10) | 2009 | USA | Plasma | 1.35 | 0.99-1.84 | |
| Geybels (42) | 2013 | Netherlands | Nail | 0.37 | 0.27-0.51 | |
| Randomized controlled trial | lippman (8) | 2009 | USA | Sel supplementation | 1.04 | 0.90-1.18 |
| Duffield Lillico-(43) | 2002 | USA | Sel supplementation | 0.48 | 0.28-0.80 | |
| Kristal (44) | 2014 | USA | Sel supplementation | 1.25 | 0.79-1.98 | |
| Klein (45) | 2011 | USA | Sel supplementation | 1.09 | 0.93-1.27 | |
| Clark (46) | 1998 | USA | Sel supplementation | 0.37 | 0.18-0.71 | |
| Duffield Lillico-(47) | 2003 | USA | Sel supplementation | 1.14 | 0.51-2.59 | |
| Algator (48) | 2013 | USA | Sel supplementation | 0.9 | 0.48-1.70 | |
| Algator (48) | 2013 | USA | Sel supplementation | 0.94 | 0.52-1.70 | |
| Dunn (49) | 2010 | USA | Sel supplementation | 1.04 | 0.87-1.24 | |
| Marshal (50) | 2011 | USA | Sel supplementation | 0.82 | 0.40-1.69 |
, Relative risk;
, Confidence interval
In subgroup analysis based on type of study in case-control, cohort and RCT (Randomized controlled trial), the RR was estimated to be 0.89 (95% CI: 0.80-1.00), 0.77 (95% CI: 0.52-1.14), 0.90 (95% CI: 0.74-1.09), respectively (Table 2).
In subgroup analysis based on samples the RR was estimated 0.69 (95% CI: 0.51-0.95) for serum, 0.85 (95% CI: 0.61-1.17) for plasma, 0.66 (95% CI: 0.41-1.05) for nail. In selenium supplementation and placebo group and in group which dietary selenium examined, RR was 0.90 (95% CI: 0.74-1.09) and 1.00 (95% CI: 0.98-1.02), respectively (Table 2).
Selenium and advanced prostate cancer
In the ten studies about the relation between selenium and advanced prostate cancer, RR was 0.67 (95% CI: 0.52-0.87), showing the significant protective role of selenium in advanced prostate cancer (Figure 4).
Figure 4.

Meta- Analysis of Studies about the Relation between Selenium and Advanced Prostate Cancer
Publication bias
In this study, p-value for publication bias of the relation between selenium and prostate cancer and its advanced type was 0.007 and 0.002, respectively. Funnel plot shows a significant effect for publication bias and some articles with significant effect may not have been published (Figure 1, 2 in supplement file).
Sub-group analysis of Selenium and advanced prostate cancer
In subgroup analysis based on the place of study, most of the studies were conducted in the USA (70%) and RR was 0.6 (95% CI: 0.45-0.81) (Table 3).
Table 3.
Meta- Analysis of Studies Regarding the Relationship between Selenium and Advanced Prostate Cancer According to the Country, Type of Study and Sample of Selenium. Random Effects Model.
| Variable | Study (Na) | Case | Control | I2(%) | 95% CIb | RRc | |
|---|---|---|---|---|---|---|---|
| Country | USA | 7 | 960 | 37,175 | 10.8 | 0.45,0.81 | 0.6 |
| United Kingdim | 1 | 89 | 300 | 0.27,2.25 | 0.78 | ||
| Denmark | 1 | 525 | 784 | 0.87,1.05 | 0.96 | ||
| Netherlands | 1 | 183 | 1,211 | 0.37,1.04 | 0.62 | ||
| Type of study | Case-control | 7 | 1,173 | 2,780 | 57.7 | 0.43,0.93 | 0.64 |
| Cohort | 3 | 584 | 36,690 | 0 | 0.51,0.97 | 0.71 | |
| Sample of selenium | Serum | 4 | 485 | 1,817 | 6.7 | 0.51,1.03 | 0.72 |
| Plasma | 2 | 696 | 1,361 | 67.1 | 0.44,1.38 | 0.78 | |
| Nail | 3 | 453 | 1,692 | 0 | 0.37,0.83 | 0.55 | |
| Diet | 1 | 123 | 34,600 | 0.17,1.27 | 0.46 |
, Number;
, Confidence interval;
, Relative risk
In subgroup analysis based on type of study in case-control and cohort studies, the RR was estimated to be 0.64 (95% CI: 0.43-0.93) and 0.71 (95% CI: 0.51-0.97) respectively (Table 3).
In subgroup analysis based on serum, plasma, nail and diet samples was estimated to be 0.72 (95% CI: 0.51-1.03), 0.78 (95% CI: 0.44-1.38), 0.55 (95% CI: 0.37-0.83), 0.46 (95% CI: 0.17-1.27) respectively (Table 3).
Discussion
Several studies have been done conducted worldwide to evaluate the relationship between selenium and prostate cancer. However, the results are inconsistent and the clear association have not been found. So our meta-analysis and systematic review study, which is a quantitative assessment of published data on the role of selenium in prostate cancer, was conducted to find the clear relation between prostate cancer and selenium without time limitation up to 2016.
There were several limitations in our study including lack of access to all articles or their full text. Other limitations were the different design for papers and using different samples for detecting selenium. One of the advantages of this meta-analysis study was the ability to do a complete analysis on subgroups, such as type of studies (RCT, Cohort, Case-control), subgroup of total prostate cancer and advanced prostate cancer as well as the samples used (toenail and plasma, serum, diet, supplementation selenium). Analysis of data showed the RR of 0.86 (95% CI: 0.78-0.94) and since confidence interval doesn’t cross significant protective role of selenium in prostate cancer was found. The heterogeneity rate in the current study was 69.4% (p=0.000), accounted in the range of studies with moderate heterogeneity. Thus, random effects model in the meta-analysis was used.
Our study confirms the result of Etminan’s (2005) systematic review showing that selenium may have a protective role against prostate cancer. However, our study is not in line with another study which indicates the increase in the risk of prostate cancer in the state of low selenium (Brinkman et al., 2006). Hurst et al., (2012) in a systematic review and meta-analysis showed that the relationship between selenium status and decreased prostate cancer risk was examined over a relatively narrow range of selenium status and they suggested more studies in low-selenium population. In Brinkman’s (2006) review study, selenium levels were inversely associated with prostate cancer risk and the need to further investigations was recommended. In another systematic review and meta-analysis, no evidence of the effect of vitamins and multivitamins was found on the occurrence and severity of the prostate cancer (Brinkman et al., 2006). According to a review study published in 2015 based on SELECT (Selenium and Vitamin E Cancer Prevention Trial) studies, there was no significant decline in the risk of prostate cancer by selenium and vitamin E supplementations and it recommended further studies to find the probable mechanisms of prostate cancer and searching newer preventive agents (Ramamoorthy et al., 2015). In a systematic review and meta-analysis, no evidence of the effect of vitamins and multivitamins on the occurrence and severity of the prostate cancer was found (Stratton et al., 2011).
In conclusion, our study shows that selenium plays a protective role in prostate cancer. However, it is suggested that more studies be conducted with less limitation, considering other environmental factors such as other trace elements, economic situation and social situation such as level of education in future.
Acknowledgments
We appreciate Ilam University of Medical Sciences for financial support.
Authorship contribution
Study concepts/study design: all authors; Collection demographic data: all authors; Meta-analysis: Koroush Sayehmiri; manuscript drafting: Zeinab Tardeh; manuscript final version approval and manuscript editing: all authors.
Conflicts of interest
None.
References
- 1.Albanes D, Till C, Klein EA, et al. Plasma tocopherols and risk of prostate cancer in the Selenium and vitamin E cancer prevention trial (SELECT) Cancer Prev Res. 2014;7:886–95. doi: 10.1158/1940-6207.CAPR-14-0058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Algotar AM, Stratton MS, Ahmann F, et al. Phase 3 clinical trial investigating the effect of selenium supplementation in men at high-risk for prostate cancer. The Prostate. 2013;73:328–35. doi: 10.1002/pros.22573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Allen N, Morris J, Ngwenyama R, et al. A case–control study of selenium in nails and prostate cancer risk in British men. Br J Cancer. 2004;90:1392–6. doi: 10.1038/sj.bjc.6601701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Allen NE, Appleby PN, Roddam AW, et al. Plasma selenium concentration and prostate cancer risk:results from the European prospective investigation into cancer and nutrition (EPIC) Am J Clin Nutr. 2008;88:1567–75. doi: 10.3945/ajcn.2008.26205. [DOI] [PubMed] [Google Scholar]
- 5.Azami M, Hafezi Ahmadi MR, Sayehmiri K. Hepatitis B vaccination efficacy in Iranian healthcare workers:A meta-analysis study. Hepat Mon. 2017;17:e37781. [Google Scholar]
- 6.Azami M, Nasirkandy MP, Mansouri A, et al. Global prevalence of Helicobacter pylori infection in pregnant women:A systematic review and meta-analysis study. IJWHR. 2017;5:30–6. [Google Scholar]
- 7.Brinkman M, Reulen RC, Kellen E, et al. Are men with low selenium levels at increased risk of prostate cancer? Eur J Cancer. 2006;42:2463–71. doi: 10.1016/j.ejca.2006.02.027. [DOI] [PubMed] [Google Scholar]
- 8.Brooks JD, Metter EJ, Chan DW, et al. Plasma selenium level before diagnosis and the risk of prostate cancer development. J Urol. 2001;166:2034–8. [PubMed] [Google Scholar]
- 9.Chan JM, Oh WK, Xie W, et al. Plasma selenium, manganese superoxide dismutase, and intermediate-or high-risk prostate cancer. J Clin Oncol. 2009;27:3577–83. doi: 10.1200/JCO.2008.18.8938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Coates RJ, Weiss NS, Daling JR, et al. Serum levels of selenium and retinol and the subsequent risk of cancer. Am J Epidemiol. 1998;128:515–23. doi: 10.1093/oxfordjournals.aje.a114999. [DOI] [PubMed] [Google Scholar]
- 11.Deeks JJ, Higgins JPT, Altman DG. Higgins JPT, Green S, editors. Chapter 9:Analysing data and undertaking meta-analyses. Cohrane handbook for sustematic reviews of interventions. Version 5.1.0, The Cochrane Collaboration. 2011. [Accessed Mar 2011]. http://training.cochrane.org/handbook .
- 12.Duffield-Lillico A, Dalkin B, Reid M, et al. Selenium supplementation, baseline plasma selenium status and incidence of prostate cancer:an analysis of the complete treatment period of the nutritional prevention of cancer trial. BJU Int. 2003;91:608–12. doi: 10.1046/j.1464-410x.2003.04167.x. [DOI] [PubMed] [Google Scholar]
- 13.Duffield-Lillico AJ, Reid ME, Turnbull BW, et al. Baseline characteristics and the effect of selenium supplementation on cancer incidence in a randomized clinical trial A summary report of the nutritional prevention of cancer trial. Cancer Epidemiol Biomarkers Prev. 2002;11:630–9. [PubMed] [Google Scholar]
- 14.Dunn BK, Richmond ES, Minasian LM, Ryan AM, Ford LG. A nutrient approach to prostate cancer prevention:The Selenium and vitamin E cancer prevention trial (SELECT) Nutr Cancer. 2010;62:896–918. doi: 10.1080/01635581.2010.509833. [DOI] [PubMed] [Google Scholar]
- 15.Etminan M, FitzGerald JM, Gleave M, Chambers K. Intake of selenium in the prevention of prostate cancer:a systematic review and meta-analysis. Cancer Causes Control. 2005;16:1125–31. doi: 10.1007/s10552-005-0334-2. [DOI] [PubMed] [Google Scholar]
- 16.Geybels MS, Verhage BA, van Schooten FJ, et al. Advanced prostate cancer risk in relation to toenail selenium levels. J Natl Cancer Inst. 2013;105:1394–401. doi: 10.1093/jnci/djt186. [DOI] [PubMed] [Google Scholar]
- 17.Ghadirian P, Maisonneuve P, Perret C, et al. A case-control study of toenail selenium and cancer of the breast, colon, and prostate. Cancer Detect Prev. 1999;24:305–13. [PubMed] [Google Scholar]
- 18.Gill JK, Franke AA, Morris JS, et al. Association of selenium, tocopherols, carotenoids, retinol, and 15-isoprostane F2t in serum or urine with prostate cancer risk:the multiethnic cohort. Cancer Causes Control. 2009;20:1161–71. doi: 10.1007/s10552-009-9304-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Goodman GE, Schaffer S, Bankson DD, et al. Predictors of serum selenium in cigarette smokers and the lack of association with lung and prostate cancer risk. Cancer Epidemiol Biomarkers Prev. 2001;10:1069–76. [PubMed] [Google Scholar]
- 20.Grönberg H. Prostate cancer epidemiology. Lancet. 2003;361:859–64. doi: 10.1016/S0140-6736(03)12713-4. [DOI] [PubMed] [Google Scholar]
- 21.Harbord RM, Harris RJ, Sterne JAC. Updated tests for small-study effects in meta-analyses. Stata J. 2009;9:197. [Google Scholar]
- 22.Hardell L, Degerman A, Tomic R, et al. Levels of selenium in plasma and glutathione peroxidase in erythrocytes in patients with prostate cancer or benign hyperplasia. Eur J Cancer prev. 1995;4:91–6. doi: 10.1097/00008469-199502000-00009. [DOI] [PubMed] [Google Scholar]
- 23.Hartman TJ, Albanes D, Pietinen P, et al. The association between baseline vitamin E, selenium, and prostate cancer in the alpha-tocopherol, beta-carotene cancer prevention study. Cancer Epidemiol Biomarkers Prev. 1998;7:335–40. [PubMed] [Google Scholar]
- 24.Helzlsouer KJ, Huang H-Y, Alberg AJ, et al. Association between α-tocopherol, γ-tocopherol, selenium, and subsequent prostate cancer. J Natl Cancer Inst. 2000;92:2018–23. doi: 10.1093/jnci/92.24.2018. [DOI] [PubMed] [Google Scholar]
- 25.Humphrey P, Schuz J. Cancers of the male reproductive organs. World cancer report Lyon:World health organization. 2014:453–64. [Google Scholar]
- 26.Hurst R, Hooper L, Norat T, et al. Selenium and prostate cancer:systematic review and meta-analysis. Am J Clin Nutr. 2012;96:111–22. doi: 10.3945/ajcn.111.033373. [DOI] [PubMed] [Google Scholar]
- 27.Jain MG, Hislop GT, Howe GR, et al. Plant foods, antioxidants, and prostate cancer risk:findings from case-control studies in Canada. Nutr Cancer. 1999;34:173–84. doi: 10.1207/S15327914NC3402_8. [DOI] [PubMed] [Google Scholar]
- 28.Knekt P, Aromaa A, Maatela J, et al. Serum selenium and subsequent risk of cancer among Finnish men and women. J Natl Cancer Inst. 1990;82:864–8. doi: 10.1093/jnci/82.10.864. [DOI] [PubMed] [Google Scholar]
- 29.Kristal AR, Arnold KB, Neuhouser ML, et al. Diet, supplement use, and prostate cancer risk:results from the prostate cancer prevention trial. Am J Epidemiol. 2010;172:566–77. doi: 10.1093/aje/kwq148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kristal AR, Darke AK, Morris JS, et al. Baseline selenium status and effects of selenium and vitamin E supplementation on prostate cancer risk. J Natl Cancer Inst. 2014;106:djt456. doi: 10.1093/jnci/djt456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lee MM, Wang R-T, Hsing AW, et al. Case-control study of diet and prostate cancer in China. Cancer Causes Control. 1998;9:545–52. doi: 10.1023/a:1008840105531. [DOI] [PubMed] [Google Scholar]
- 32.Li H, Stampfer MJ, Giovannucci EL, et al. A prospective study of plasma selenium levels and prostate cancer risk. J Natl Cancer Inst. 2004;96:696–703. doi: 10.1093/jnci/djh125. [DOI] [PubMed] [Google Scholar]
- 33.Lippman SM, Klein EA, Goodman PJ, et al. Effect of selenium and vitamin E on risk of prostate cancer and other cancers:the Selenium and vitamin E cancer prevention trial (SELECT) JAMA. 2009;301:39–51. doi: 10.1001/jama.2008.864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Lipsky K, Zigeuner R, Zischka M, et al. Selenium levels of patients with newly diagnosed prostate cancer compared with control group. J Urol. 2004;63:912–6. doi: 10.1016/j.urology.2003.12.028. [DOI] [PubMed] [Google Scholar]
- 35.Marshall JR, Tangen CM, Sakr WA, et al. Phase III trial of selenium to prevent prostate cancer in men with high-grade prostatic intraepithelial neoplasia:SWOG S9917. Cancer Prev Res. 2011;4:1761–9. doi: 10.1158/1940-6207.CAPR-10-0343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Miller AB. New data on prostate-cancer mortality after PSA screening. N Engl J Med. 2012;366:1047–8. doi: 10.1056/NEJMe1200185. [DOI] [PubMed] [Google Scholar]
- 37.Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses:the PRISMA statement. Ann Intern Med. 2009;151:264–9. doi: 10.7326/0003-4819-151-4-200908180-00135. [DOI] [PubMed] [Google Scholar]
- 38.Nomura AM, Lee J, Stemmermann GN, et al. Serum selenium and subsequent risk of prostate cancer. Cancer Epidemiol Biomarkers Prev. 2000;9:883–7. [PubMed] [Google Scholar]
- 39.Ornish D, Weidner G, Fair WR, et al. Intensive lifestyle changes may affect the progression of prostate cancer. J Urol. 2005;174:1065–70. doi: 10.1097/01.ju.0000169487.49018.73. [DOI] [PubMed] [Google Scholar]
- 40.Outzen M, Tjønneland A, Larsen EH, et al. Selenium status and risk of prostate cancer in a Danish population. Br J Nutr. 2016;115:1669–77. doi: 10.1017/S0007114516000726. [DOI] [PubMed] [Google Scholar]
- 41.Peters U, Foster CB, Chatterjee N, et al. Serum selenium and risk of prostate cancer-a nested case-control study. Am J Clin Nutr. 2007;85:209–17. doi: 10.1093/ajcn/85.1.209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Peters U, Littman AJ, Kristal AR, et al. Vitamin E and selenium supplementation and risk of prostate cancer in the Vitamins and lifestyle (VITAL) study cohort. Cancer Causes Control. 2008;19:75–87. doi: 10.1007/s10552-007-9072-y. [DOI] [PubMed] [Google Scholar]
- 43.Pourmand G, Salem S, Moradi K, et al. Serum selenium level and prostate cancer:a case-control study. Nutr Cancer, 2008;60:171–6. doi: 10.1080/01635580701627277. [DOI] [PubMed] [Google Scholar]
- 44.Ramamoorthy V, Rubens M, Saxena A, et al. Selenium and vitamin E for prostate cancer-justifications for the SELECT study. Asian Pac J Cancer Prev. 2015;16:2619–27. doi: 10.7314/apjcp.2015.16.7.2619. [DOI] [PubMed] [Google Scholar]
- 45.Siegel R, Ward E, Brawley O, et al. Cancer statistics. CA Cancer J Clin. 2011;61:212–36. doi: 10.3322/caac.20121. [DOI] [PubMed] [Google Scholar]
- 46.Siegel RL, Miller KD, Jemal A. Cancer statistics. CA Cancer J Clin. 2016;66:7–30. doi: 10.3322/caac.21332. [DOI] [PubMed] [Google Scholar]
- 47.Stratton J, Godwin M. The effect of supplemental vitamins and minerals on the development of prostate cancer:a systematic review and meta-analysis. J Fam Pract. 2011;28:243–52. doi: 10.1093/fampra/cmq115. [DOI] [PubMed] [Google Scholar]
- 48.van den Brandt PA, Zeegers MP, Bode P, et al. Toenail selenium levels and the subsequent risk of prostate cancer a prospective cohort study. Cancer Epidemiol Biomarkers Prev. 2003;12:866–71. [PubMed] [Google Scholar]
- 49.Vinceti M, Rovesti S, Gabrielli C, et al. Cancer mortality in a residential cohort exposed to environmental selenium through drinking water. J Clin Epidemiol. 1995;48:1091–7. doi: 10.1016/0895-4356(95)00014-u. [DOI] [PubMed] [Google Scholar]
- 50.Virtamo J, Valkeila E, Alfthan G, et al. Serum selenium and risk of cancer. A prospective follow-up of nine years. Cancer. 1987;60:145–8. doi: 10.1002/1097-0142(19870715)60:2<145::aid-cncr2820600203>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- 51.Vogt TM, Ziegler RG, Graubard BI, et al. Serum selenium and risk of prostate cancer in US blacks and whites. Int J Cancer. 2003;103:664–70. doi: 10.1002/ijc.10866. [DOI] [PubMed] [Google Scholar]
- 52.West DW, Slattery ML, Robison LM, et al. Adult dietary intake and prostate cancer risk in Utah:a case-control study with special emphasis on aggressive tumors. Cancer Causes Control. 1991;2:85–94. doi: 10.1007/BF00053126. [DOI] [PubMed] [Google Scholar]
- 53.Witherington R, Janosko JHE, Borosso DCС, et al. Decreased incidence of prostate cancer with selenium supplementation:results of a double-blind cancer prevention trial. Br J Urol. 1998;81:730–4. doi: 10.1046/j.1464-410x.1998.00630.x. [DOI] [PubMed] [Google Scholar]
- 54.Yoshizawa K, Willett WC, Morris SJ, et al. Study of prediagnostic selenium level in toenails and the risk of advanced prostate cancer. J Natl Cancer Inst. 1998;90:1219–24. doi: 10.1093/jnci/90.16.1219. [DOI] [PubMed] [Google Scholar]
- 55.Zhang Y, Coogan P, Palmer JR, et al. Vitamin and mineral use and risk of prostate cancer:the case–control surveillance study. Cancer Causes Control. 2009;20:691–8. doi: 10.1007/s10552-008-9282-y. [DOI] [PMC free article] [PubMed] [Google Scholar]