
Figure 1.
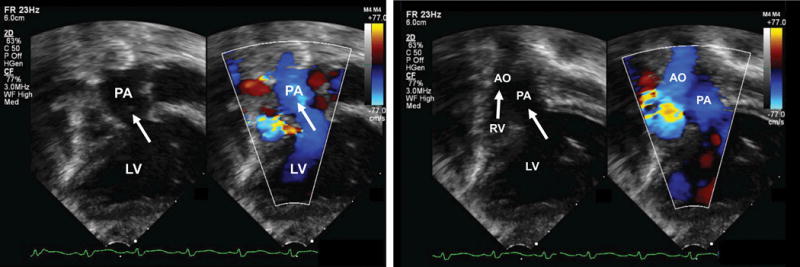
Application of the Fetal Intelligent Navigation Echocardiography (FINE) method to a spatiotemporal image correlation (STIC) volume dataset of a fetus with dextrocardia, situs solitus, and complex congenital heart disease at 35 weeks of gestation (Videoclip S1). Nine cardiac diagnostic planes are displayed automatically in a single template with automatic labeling of the fetal left and right sides, cranial and caudal direction, each diagnostic plane, and anatomical structures. All of the nine echocardiography views are abnormal [diagnostic planes and/or Virtual Intelligent Sonographer Assistance (VIS-Assistance®)]. The three-vessels and trachea view diagnostic plane shows the well-developed leftward pulmonary artery arising from the dilated left ventricle, while a hypoplastic aorta is rightward and anterior to the pulmonary artery, and arises from the hypoplastic right ventricle (ventricle not shown in this frame) (i.e. D-transposition of the great vessels). Note that the three-vessel and trachea view shows a “Y-shape” configuration, in which the aorta is anterior to the pulmonary artery. In addition, automatic labeling by FINE is correct. The four-chamber view diagnostic plane shows dextrocardia, a dilated left ventricle, enlarged mitral valve with redundancy in leaflet tissue, severely hypoplastic right ventricle, tricuspid atresia caused by a thick membrane, enlarged right atrium, and large interatrial communication. Note that automatic labeling of all four chambers by FINE is correct. The five-chamber view diagnostic plane shows findings similar to that of the four-chamber view, as well as a ventricular septal defect. The “Ao” label here does not actually point to the aorta itself; however, the label is precisely where the aorta should exit from the hypoplastic right ventricle. In the left ventricular outflow tract diagnostic plane, the well-developed pulmonary artery arises from the left ventricle (not well shown in this frame). For the short-axis view of great vessels/right ventricular outflow tract, VIS-Assistance® was activated to show this plane, which appears abnormal. The pulmonary artery arises from the dilated left ventricle (the “RV” automatic label is incorrect here). In the abdomen view diagnostic plane, viscero-atrial situs solitus was determined by the location of the inferior vena cava (anterior and right of the spine), descending aorta (posterior and left of the spine), hepatic venous drainage (not shown here), right-sided liver, and stomach on the left side. For the ductal arch view, VIS-Assistance® was activated to show this image, which appears abnormal. The pulmonary artery arises from the dilated left ventricle (the “RV” automatic label is incorrect here). For the aortic arch view, triple VIS-Assistance® was performed to obtain the plane displayed here. The ascending aorta is seen arising from the hypoplastic right ventricle, and narrowing in the transverse aortic arch and isthmus region is consistent with coarctation of the aorta. Note that automatic labeling of the aortic arch view by FINE is correct. The venae cavae diagnostic plane shows the superior and inferior vena cava entering the right atrium. In the superior part of the image, tricuspid atresia (between the right atrium and ventricle), is shown. A, transverse aortic arch; Ao, aorta; Desc., descending; IVC, inferior vena cava; LA, left atrium; LV, left ventricle; P, pulmonary artery; PA, pulmonary artery; RA, right atrium; RV, right ventricle; RVOT, right ventricular outflow tract; S, superior vena cava; SVC, superior vena cava; Trans., transverse