

Abstract
Uterine compression suturing is a relatively easy and effective way of hemostasis during cesarean section and is becoming widely accepted. However, complications such as necrosis or synechiae have been reported. We firstly report a case of laparoscopic removal of vertical compression sutures and discuss its benefits and improvements to be made. This case report is of a 32-year-oId woman with placenta previa who received uterine vertical compression sutures for controlling massive bleeding during cesarean section. Because she complained of unbearable pelvic pain, laparoscopic compression suture removal was performed. Her pain was relieved after the threads were removed, suggesting that the compression sutures were the cause of her pelvic pain due to uterine ischemia. Although the risks of reoperation during the early postpartum period still exist, compression suture thread removal should be considered in cases of suspected uterine ischemia.
Keywords: laparoscopic surgery, side effect, suture removal, uterine ischemia, vertical compression suture
Introduction
Uterine compression suturing is now widely accepted for hemostasis during cesarean section. Above all, B-Lynch suturing is one of the most widely employed methods for controlling postpartum hemorrhage.1 Several different types of compression sutures have been developed since then; however, most of them are for controlling uterine corpus bleeding. Double vertical compression sutures have been reported as specialized because they control bleeding from both the uterine corpus and uterine isthmus, especially in placenta previa cases.2 Above all, those compression sutures are relatively easy and an effective way of hemostasis; however, complications such as necrosis or synechiae have been reported.3,4,5,6,7,8 To avoid these complications, compression suture removal was attempted vaginally and abdominally.9,10 The compression sutures required special techniques for removal. Here we report a case of laparoscopic removal of vertical compression sutures, which is another method for avoiding uterine ischemia or synechiae, and we discuss its benefit and any improvements to be made.
Case Report
A 32-year-old (gravida 1 para 1) woman with elective cesarean section for placenta previa received vertical compression sutures2 using 0 Vicryl plus (Ethicon, Somerville, NJ, USA) after a balloon tamponade test had no effect (Figure 1). As she complained of unbearable pelvic pain and a small amount of lochia without pooling in the uterus, uterine ischemia was conceivable. We decided to remove the compression suture threads using laparoscopy.
Figure 1.
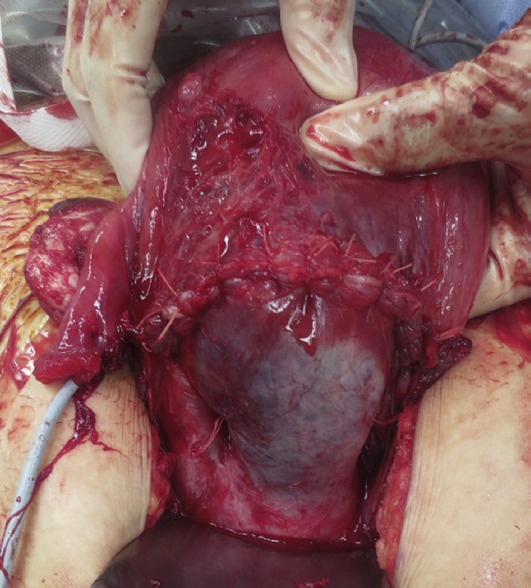
Vertical compression sutures during cesarean section. Compression suture threads are seen at the uterine isthmus.
We considered that a flexible laparoscope (EndoEye; Olympus, Tokyo, Japan) would be helpful in detecting the compression sutures located on her uterine isthmus, as her enlarged uterus at 3 days after cesarean section might have disturbed the view into the deep aspect of her pelvis. After a 5-mm trocar was inserted into her umbilicus for the optical device and a pneumoperitoneum was created, two 3.5-mm thin trocars (Aesculap AdTec mini, B. Braun, Germany) were inserted into her lower abdomen 3 cm inside of the bilateral anterior superior iliac spine. Although the flexible laparoscope allowed the visualization of the uterine isthmus, the locations of the sutured points were obscure due to flaccid uterine isthmus. We then elevated her uterus by vaginally inserting a Kocher crump (MIZUHO Corporation, Tokyo, Japan) with folded gazes. As a result, we could detect the sutured points and the threads were carefully pulled and successfully removed using 3-mm forceps without the special technique to presuppose the suture removal that was previously reported.9,10 As a result of compression suture removal, the patient was relieved from her pelvic pain and the lochia discharge started, suggesting that the compression sutures were the causes of the pelvic pain due to uterine ischemia. Compression suture removal may contribute to the avoidance of uterine necrosis.
Compression suture removal is a good way to avoid severe complications after compression suture; however, patient selection has to be carefully discussed because of the following reasons. Reoperation itself may lead to additional complications and it costs much more than the natural course. Only patients with extreme pelvic pain, which suggests the existence of uterine ischemia or necrosis, will be candidates for this operation. Aboulfalah et al9 reported that removal of the sutures 24–48 hours after the compression suture application may prevent synechia and help maintain fertility. Once it is decided that the compression sutures are to be removed, it has to be done as soon as the situation allows.
Laparoscopic surgery is known for good visibility; however, during the operation, we felt it was difficult to distinguish the threads between the cesarean wound sutures and compression sutures because the color of the threads were both white. Contrivance, such as to choose a different color thread or to change lengths or numbers of the knots, may help to make it easier to and scissors (Figure 2). Her pelvic pain was relieved and the lochia discharge started after the surgery with a visual analogue scale score decrease from 6 out of 10 to 2 out of 10. She was discharged from the hospital 5 days after the cesarean section. She was followed up at the outpatient clinic and currently has no evident complications.
Figure 2.
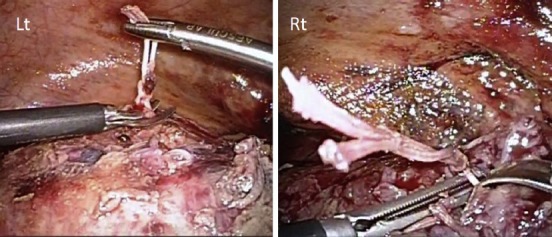
Laparoscopic compression suture removal. The threads were pulled with 3-mm forceps and cut using scissors. Adhesion prevention agent (Seprafilm; Kaken Pharmaceutical, Tokyo, Japan) started to dissolve to form a belag. Lt = left; Rt = right.
Discussion
This is the first report of laparoscopic compression suture removal. The surgery was successfully accomplished without any complications. Minimal invasiveness–the advantage of the laparoscopic surgery–contributed to the short length of her hospital stay; she was discharged from hospital 5 days after the caesarean section, which is the same length of time for normal cesarean sections in our facility. Furthermore, laparoscopic removal may accommodate any type of compression suture, even detect the compression suture threads.
In conclusion, although the risk of reoperation during the early postpartum period still exists, compression suture thread removal should be considered in the cases of uterine ischemia.
Footnotes
Conflicts of interest: The authors have no conflicts of interest relevant to this article.
References
- 1.B-Lynch C, Coker A, Lawal AH, Abu J, Cowen MJ. The B-Lynch surgical technique for the control of massive postpartum hemorrhage: an alternative to hysterectomy?Five cases reported. Br J Obstet Gynaecol. 1997;104:372–375. doi: 10.1111/j.1471-0528.1997.tb11471.x. [DOI] [PubMed] [Google Scholar]
- 2.Makino S, Tanaka T, Yorifuji T, Koshiishi T, Sugimura M, Takeda S. Double vertical compression sutures: A novel conservative approach to managing post-partum hemorrhage due to placenta previa and atonic bleeding. Aust NZJ Obstet Gynaecol. 2012;52:290–292. doi: 10.1111/j.1479-828X.2012.01422.x. [DOI] [PubMed] [Google Scholar]
- 3.Joshi VM, Shrivastava M. Partial ischemic necrosis of the uterus following a uterine brace compression suture. BJOG. 2004;111:279–280. doi: 10.1111/j.1471-0528.2004.00056.x. [DOI] [PubMed] [Google Scholar]
- 4.Wu HH, Yeh GP. Uterine cavity synechiae after hemostatic square suturing technique. Obstet Gynecol. 2005;105:1176–1178. doi: 10.1097/01.AOG.0000159978.26472.a4. [DOI] [PubMed] [Google Scholar]
- 5.Treloar EJ, Anderson RS, Andrews HS, Bailey JL. Uterine necrosis following B-Lynch suture for primary postpartum hemorrhage. BJOG. 2006;113:486–488. doi: 10.1111/j.1471-0528.2006.00890.x. [DOI] [PubMed] [Google Scholar]
- 6.Gottlieb AG, Pandipati S, Davis KM, Gibbs RS. Uterine necrosis: a complication of uterine compression sutures. Obstet Gynecol. 2008;112:429–431. doi: 10.1097/AOG.0b013e31817b0781. [DOI] [PubMed] [Google Scholar]
- 7.Poujade O, Grossetti A, Mougel L, Ceccaldi PF, Ducarme G, Luton D. Risk of synechiae following uterine compression sutures in the management of major postpartum hemorrhage. BJOG. 2011;118:433–439. doi: 10.1111/j.1471-0528.2010.02817.x. [DOI] [PubMed] [Google Scholar]
- 8.Rathat G, Do Trinh P, Mercier G, Ceccaldi PF, Ducarme G, Luton D. Synechia after uterine compression sutures. Fertil Steril. 2011;95:405–409. doi: 10.1016/j.fertnstert.2010.08.055. [DOI] [PubMed] [Google Scholar]
- 9.Aboulfalah A, Fakhir B, Ait Ben Kaddour Y, Asmouki H, Soummani A. A new removable uterine compression by a brace suture in the management of severe postpartum hemorrhage. Front Surg. 2014;17:43. doi: 10.3389/fsurg.2014.00043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zhang ZW, Liu CY, Yu N, Guo W. Removable uterine compression sutures for postpartum hemorrhage. BJOG. 2015;122:429–433. doi: 10.1111/1471-0528.13025. [DOI] [PubMed] [Google Scholar]