
Figure 3.
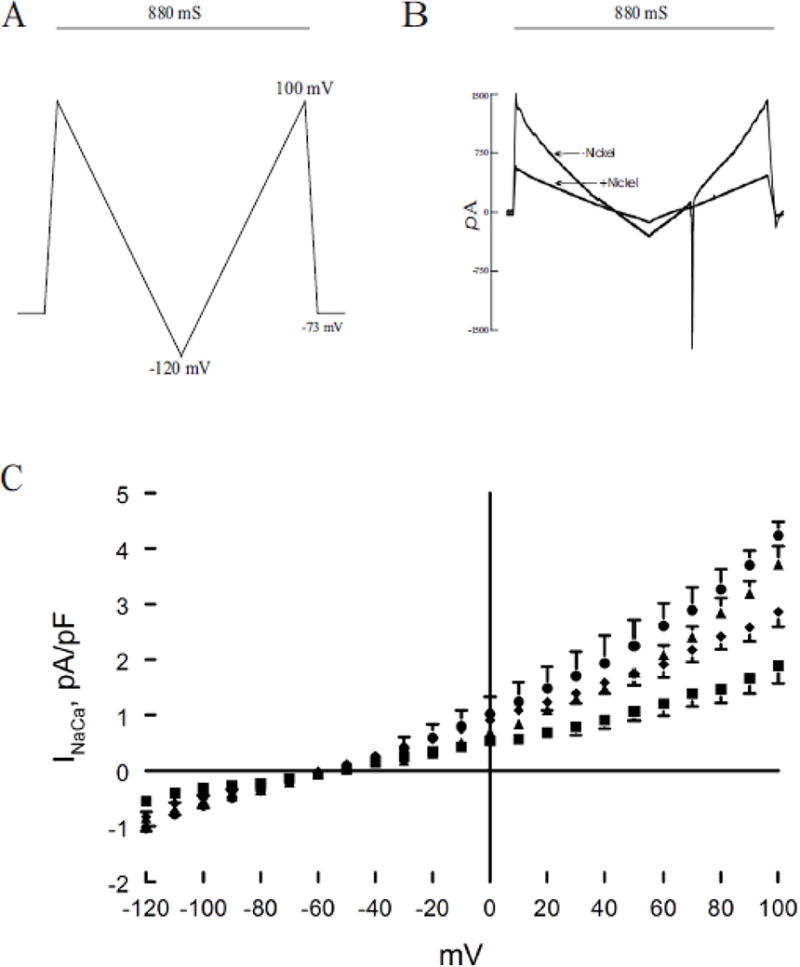
H2S inhibits Na+/Ca2+ exchanger current (INaCa): reversal by MB. Pipette solution contained (in mM) 100 Cs+ glutamate, 7.25 NaCl, 1 MgCl2, 20 HEPES, 2.5 Na2ATP, 10 EGTA and 6 CaCl2, pH 7.2. Free Ca2+ in the pipette solution was 205 nM, measured fluorimetrically with fura-2. External solution contained (in mM) 130 NaCl, 5 CsCl, 1.2 MgSO4, 1.2 NaH2PO4, 5 CaCl2, 10 HEPES, 10 Na+ HEPES and 10 glucose, pH 7.4. Verapamil (1 μM) was used to block ICa,L. Our measurement conditions were biased towards measuring outward (3 Na+ out: 1 Ca2+ in) INaCa. (A). After holding the myocyte at the calculated reversal potential (−73 mV) of INaCa for 5 min (to minimize fluxes through Na+/Ca2+ exchanger and thus allowed [Na+]i and [Ca2+]i to equilibrate with those in pipette solution), INaCa (30°C) was measured in myocytes using a descending (from +100 to −120 mV; 500 mV/s) – ascending (from −120 to +100 mV; 500 mV/s) voltage ramp, first in the absence and then in the presence of 1 mM NiCl2. (B). Raw currents measured in a WT myocyte. INaCa was defined as the difference current measured in the absence and presence of Ni+ during the descending voltage ramp. Note that with the exception of small contamination of the ascending ramp by the cardiac Na+ current, there were little to no differences in INaCa measured between the descending and ascending voltage ramps. This suggests that [Ca2+]i and [Na+]i sensed by Na+/Ca2+ exchanger did not appreciably change by ion fluxes during the brief (880 ms) voltage ramp. INaCa was divided by Cm prior to comparisons. (C). At time 0, either saline or NaHS (100 μM) was added followed by MB (20 μg/ml) or saline at 3 min before INaCa was measured at 7 min. Current-voltage relationships of INaCa (means ± SE) from control (▲; n=6), MB (●; n=3), NaHS (■; n=5) and NaHS + MB (◆; n=5) myocytes are shown. The reversal potential of INaCa was ~ −60 mV, close to the theoretical reversal potential of −73 mV. Error bars are not shown if they fall within the boundaries of the symbol.