

Abstract
Obstructing lesions of vagina, such as transverse vaginal septum, are rare anomalies. In this paper, we report a case of posttraumatic transverse vaginal septum. The patient was a 14-year-old girl who had a transverse vaginal septum because of repaired perineal trauma happened during earthquake that hit Bam city of Iran, when she was three years old. Post-traumatic vaginal septum had resulted in development of a massive hematometra. To our knowledge, this is the first report of urinary incontinence due to massive hematometra, which resulted from a posttraumatic vaginal septum. The rareness and diversity of clinical presentations of vaginal obstructing lesions can lead to misdiagnosis. The patient might refer to different medical and surgical specialists. So, knowing the symptoms is necessary for its early diagnosis. The probability of vaginal obstructing lesions in peripubertal girls with lower urinary tract symptoms should always be considered.
Keywords: Urinary incontinence, urinary retention, vaginal septum
Introduction
Obstructing lesions of vagina, such as transverse vaginal septum, are rare anomalies.[1] Their major manifestations are primary amenorrhea and cyclic abdominal pain, but acute urinary retention is less common.[2] In this paper, we report a case of posttraumatic transverse vaginal septum. It had two different urinary symptoms: 1) irritative symptoms like frequency, nacturia and urinary incontinence because of the compressive forces exerted by massive hematometra on the bladder; 2) obstructive symptoms and urinary retention because of mechanical obstruction by hematocolpus that was due to vaginal restenosis developed three months after her treatment.
The case was a 14-year-old girl who had a transverse vaginal septum because of repaired perineal trauma after Bam earthquake, Iran, when she was three years old that had resulted in a massive hematometra. To our knowledge, this is the first report of urinary incontinence due to massive hematometra developed secondary to a posttraumatic vaginal septum.
Case Presentation
In April 2014, a 14-year-old girl referred to our hospital in Kerman city, Iran, with fever, abdominal pain and urinary incontinence. She had suffered from recurring abdominal pain two to three days per month for six months before her referral. First, she required oral analgesics for pain relief, but later the pain was relieved only with parenteral analgesics. Her parents gave an informed consent to perform all the required therapeutic interventions for her treatment.
She had a reduced appetite and constipation. Her urination had a disruptive pattern and she had irritative symptoms like frequency and nocturia. However, sometime after admittance, she had urinary incontinence and used pads. Gradual abdominal enlargement and low-grade fever were the other symptoms. She had developed secondary sexual characteristics but had never menstruated. She was ill-looking and febrile at 38.5°C.
A suprapubic mass was detected on her abdominal examination. Perineal examination revealed a thick transverse septum that obstructed the vaginal opening at introitus (Figure 1). This septum was a sequela of a pelvic trauma repair after the Bam earthquake in 2003 when she was three years old.
Figure 1.

A thick transverse septum that obstructed the vaginal opening at introitus detected during perineal examination
Ultrasound of the pelvis and abdomen showed significant mixed echogenic thick fluid accumulation in the retropubic space. This was suspected to be hematometrocolpos associated with vaginal septum. The ovaries appeared normal. Both kidneys were normal. Urinalysis was normal.
Due to the complex anatomy, we inserted Foley catheter, following cystoscopic examination and urethral dilation, but significant amount of residual urine was not detected. The patient underwent intravenous pyelography, voiding cystography, computed-topographic cystography, pelvi-abdominal magnetic resonance imaging (Figures 2–5). All of them revealed a cystic retropubic mass that compressed the bladder and rectum. The patient was operated under general anesthesia in the lithotomy position. A tense and tender mass was found on vaginal examination that had made the vaginal septum bulge. Rectal examination revealed an anterior cystic mass.
Figure 2.

Intravenous pyelogram demonstrating a mass effect on the bladder but the kidneys are intact
Figure 3.
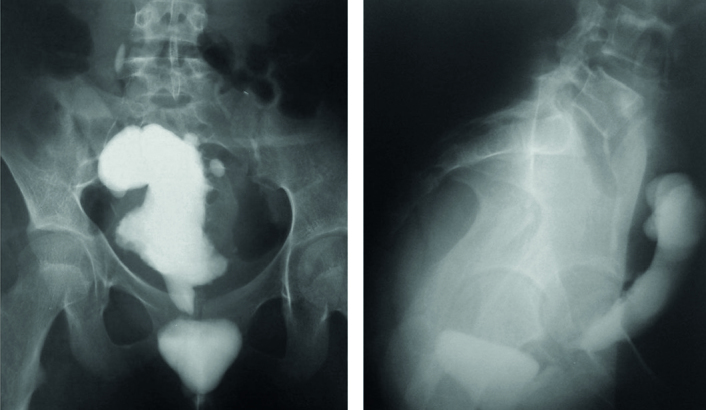
Voiding cystogram demonstrating mass effect on the bladder and mild reflux on the right side
Figure 4.
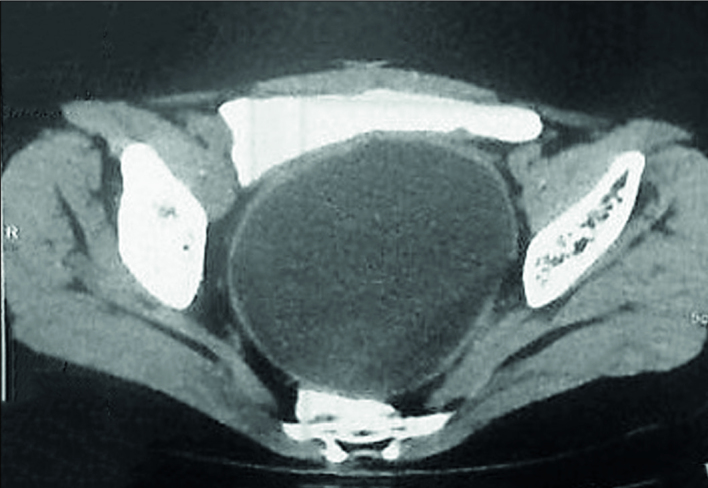
Computed tomographic cryptogram demonstrating hematocolpos posterior to the bladder
Figure 5.

Magnetic resonance imaging demonstrating the hematocolpos posterior to the urinary bladder
A layer of repaired tissue formed a thick transverse septum and obstructed the vaginal opening at introitus. A Sheeba needle was inserted into the abscess cavity under general anesthesia under ultrasound guidance. A chocolate-colored menstrual blood and pus was aspirated. Then the tract was dilated up to a finger size. Vaginal septal was about 1 cm-thick. At least 600 cc of pus was drained by a metallic suction catheter. Because of reduced injury risk to the urethra, we made an X-shaped incision with finger guide on septum. Digital rectal examination was done to protect the rectum during surgery.
After four days, the patient was discharged with a good general condition. She was recommended to do vaginal dilation with Vaginal Dilator Mold every night. But three months later, she referred with acute urinary retention and severe lower abdominal pain. In the physical examination, her vital signs were normal. Only a low-grade fever was detected. The full bladder was distended to the umbilicus. She had no history of neurologic disorder and had not had taken antihistamines or anticholinergic drugs. After urethral catheterization, 500 mL of turbid urine was drained. Then we administered intravenous antibiotics. Vaginal examination and ultrasound revealed that the septum had reclosed. This time the septum was completely removed by wedge resection and anchored by 0–2 Vicryl sutures. A 1 cm-vaginal mold with a drain was sutured to vagina for a week and then was removed. Vaginal dilation with mold continued for two months every night. The regular voiding function of the patient was restored after the surgery until two years follow-up.
Discussion
Obstructing lesions of vagina, such as imperforate hymen, transverse vaginal septum, urogenital sinus, and cloacal malformation, might happen during early childhood and adolescence. They may have different clinical presentations. So, knowing their clinical presentation may prevent misdiagnosis. Congenital transverse vaginal septum is a rare anomaly, with an unknown prevalence ranging from 1/2,100 to 1/84,000 people.[3–5] It occurs in adolescents with a median age of 13.2 years (11–16 years )[6] or 2.5–4 years after the menarche.[7] Family history has been reported as the cause in few cases. For example, in a study, two sisters had this rare anomaly and were presented with hypogastric abdominal pain at 11 and 12 years old.[8]
These obstructing lesions of vagina are mostly revealed with manifestations of primary amenorrhea, cyclical lower abdominal or pelvic pains (up to 60%),[9] low back pain (38–40%),[10] urinary outflow obstruction and its complications (58%),[2,11] constipation (20–27%),[11–13] edema of the lower extremities due to compression of the pelvic veins,[9] pelvic mass on examination (20%),[11] a bluish bulging hymen (60%),[11] and complications because of late presentation such as ruptured hematosalpinx, endometriosis, tubal adhesions and infection.[11]
Based on previous reports, obstructing vaginal lesions can cause urinary obstructive symptoms due to pressure on the bladder neck, urethra kinking, urethral tamponade and cephalad angulation at the urethral meatus.[14] Here, we have reported a case of urinary incontinence due to massive hematometra that resulted from a posttraumatic vaginal septum. She was a 14-year-old girl who had two different urinary system presentations due to obstructing vaginal septum including irritative symptoms like frequency, nocturia and urinary incontinence due to a compression of massive hematometra on the bladder, and obstructive symptoms and urinary retention because of urethral obstruction by hematocolpos after reclosure of vaginal septum.
In 2016 two cases of Herlyn-Werner-Wunderlich syndrome were presented with overflow incontinence and abdominal pain in puberty. These symptoms were completely resolved after vaginal septum resection.[15]
The rareness and diversity of clinical presentations of vaginal obstructing lesions may lead to misdiagnosis. The patient might refer to different medical and surgical specialists. So, knowing the symptoms is necessary for its early diagnosis. The probability of vaginal obstructing lesions in peripubertal girls with lower urinary tract symptoms should always be considered.
Acknowledgments
The authors would like to thank Muhammed Hussein Mousavinasab for editing this text.
Footnotes
Informed Consent: Written informed consent was obtained from the parents of the patient.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - M.M., A.D.; Design - M.M., A.D.; Supervision - M.M., A.D.; Resources - M.M., A.D.; Materials - M.M., A.D.; Data Collection and/or Processing - M.M., A.D.; Analysis and/or Interpretation - M.M., A.D.; Literature Search - M.M., A.D.; Writing Manuscript - M.M., A.D.; Critical Review - M.M., A.D.
Conflict of Interest: Authors have no conflicts of interest to declare.
Financial Disclosure: The authors have declared that did not receive any financial support for this study.
References
- 1.Nazir Z, Rizvi RM, Qureshi RN, Khan ZS, Khan Z. Congenital vaginal obstructions: varied presentation and outcome. Pediatr Surg Int. 2006;22:749–53. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]
- 2.Al-Hunaidi O, El-Shazly M, Alkandari M, Ghobashy A, Alhajeri F, Allam A. Acute urine retention caused by hematocolpos after failed hymenotomy in 23 year old female. Urol Case Rep. 2015;3:50–1. doi: 10.1089/end.2007.0380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Edmonds DK, Rose GL. Outflow tract disorders of the female genital tract. Obstet Gynaecol. 2013;15:11–7. [Google Scholar]
- 4.Williams C, Nakhal RS, Hall-Craggs MA, Wood D, Cutner A, Pattison SH, Creighton SM. Transverse vaginal septae: management and long-term outcomes. BJOG. 2014;121:1653–8. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]
- 5.Arkoulis N, Kearns C, Deeny M, Telfer J. The interdigitating Y-plasty procedure for the correction of transverse vaginal septa. BJOG. 2017;124:331–5. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]
- 6.Liang CC, Chang SD, Soong YK. Long-term follow-up of women who underwent surgical correction for imperforate hymen. Arch Gynecol Obstet. 2003;269:5–8. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]
- 7.Kurdoglu Z, Kurdoglu M, Kucukaydin Z. Spontaneous rupture of the imperforate hymen in an adolescent girl with hematocolpometra. ISRN Obstet Gynecol. 2010 doi: 10.5402/2011/520304. 520304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.González García G, Bretón Hernández P, Boillos Calvo MJ, Puigbert AM. Transverse vaginal septum diagnosed in sisters: cases report. Arch Argent Pediatr. 2017;115:e150–2. doi: 10.5546/aap.2017.e150. [DOI] [PubMed] [Google Scholar]
- 9.Nagai K, Murakami Y, Nagatani K, Nakahashi N, Hayashi M, Higaki T, et al. Life-threatening acute renal failure due to imperforate hymen in an infant. Pediatr Int. 2012;54:280–2. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]
- 10.Dane C, Dane B, Erginbas M, Cetin A. Imperforate hymen-a rare cause of abdominal pain: two cases and review of the literature. J Pediatr Adolesc Gynecol. 2007;20:245–7. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]
- 11.Lui CT, Chan TWT, Fung HT, Tang SYH. A retrospective study on imperforate hymen and haematometrocolpos in a regional hospital. Hong Kong J Emerg Med. 2010;17:435–40. doi: 10.1089/end.2007.0380. [DOI] [Google Scholar]
- 12.Heckmann R, de la Fuente FA, Heiner JD. Pediatric urinary retention and constipation: vaginal agenesis with hematometrocolpos. West J Emerg Med. 2015;16:418–9. doi: 10.1089/end.2007.0380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mou J, Tang PM, Chan KW, Tam YH, Lee KH. Imperforate hymen: cause of lower abdominal pain in teenage girls. Singapore Med J. 2009;50:e378–9. [PubMed] [Google Scholar]
- 14.Quinn T, Erickson V, Knudson MM. Down’s syndrome, precocious puberty, and transverse vaginal septum: An unusual cause of abdominal pain. J Pediatr Surg. 2001;36:641–3. doi: 10.1089/end.2007.0380. [DOI] [PubMed] [Google Scholar]
- 15.Dogan A, Uyar I, Demirtas GS, Ekin A, Gulhan I, Ertas IE, et al. Urinary incontinence in puberty: a rare clinical presentation of the herlyn-werner-wunderlich syndrome. J Pediatr Adolesc Gynecol. 2016;29:e101–3. doi: 10.1016/j.jpag.2016.07.013. [DOI] [PubMed] [Google Scholar]