

Supplemental Digital Content is available in the text.
Abstract
Introduction:
Total parenteral nutrition (TPN) provides vital intravenous nutrition for patients who cannot tolerate enteral nutrition but is susceptible to medical errors due to its formulation, ordering, and administrative complexities. At Johns Hopkins All Children’s Hospital, 22% of TPN orders required clarification of errors and averaged 10 minutes per order for error correction by pharmacists. Quality improvement methodology improved patient safety by standardizing TPN formulations and incorporating TPN ordering processes into the electronic medical record.
Methods:
A multidisciplinary group of providers developed standardized TPN solutions for neonatal and pediatric patients. Inclusion, exclusion, and discontinuation criteria were defined. The primary outcome measure was reducing TPN ordering error rate, and secondary outcomes were improving TPN ordering and processing time along with reducing blood draws. Through multiple plan-do-study-act cycles, we standardized TPN solutions, incorporated them in the electronic medical record, monitored blood draws, and evaluated resource efficiency. Data were analyzed using chi-square tests of independence and t tests for 2 independent samples.
Results:
The TPN ordering error rate significantly decreased from baseline of 22% to 3.2% over the final quarter of the study period, χ2 (1, N = 2,467) = 89.13, P < 0.001. Order processing time fell from 10 to 5 minutes by project end. The average number of blood draws decreased significantly from 6.2 (SD = 3.12) blood draws to 4.3 (SD = 2.13) in the last quarter of the study, t (506) = 5.97, P < 0.001.
Conclusions:
Standardizing TPN and transitioning to electronic ordering effectively and significantly reduced ordering errors and processing time. It also substantially improved resource efficiency by reducing the number of blood draws.
INTRODUCTION
Total parenteral nutrition (TPN) is a lifesaving source of intravenous nutrition for patients who cannot tolerate enteral nutrition. Ordering TPN is complicated and time-consuming. It is a complex formulation of macro- and micronutrients, resulting in a high incidence of ordering and administrative errors, especially in neonates and pediatric patients.1 Safe administration of customized TPN requires clinician concentration and interpretation.
As more infants are born prematurely or with medical complications requiring TPN, it is likely that its utilization will continue to increase. Conventional wisdom suggests individualized TPN provides the best combination of micronutrients for unstable patients.2 Conversely, micromanaging parenteral nutrition with frequent manipulation of the components increases the risk of error without measurable benefit to the patient.3,4 Further, studies have shown customized orders often deviate from recommendations.5
The American Society for Parenteral and Enteral Nutrition advocates for standardized processes for TPN delivery.6 Creating standardized TPN solutions reduces the likelihood of ordering errors and increases efficiency in both ordering and preparing TPN,3 which can improve patient safety, increase clinical effectiveness, and maximize resource efficiency. Boosting efficiency enhances patient care by allowing clinicians to focus their time identifying and rectifying other issues to optimize patient outcomes.3 Standardization reduces variation and promotes uniformity among clinicians.5–7 Brown et al.8 demonstrated a reduction in TPN ordering errors by instituting a tool that allows prescribers to uncover solubility issues before placing orders.
At our institution, baseline TPN ordering error rates requiring correction of nutritional contents and solution compatibility errors (eg, calcium-phosphate ratios) was 22% for 1,996 orders placed over 66 days. Pharmacists spent 10 minutes per TPN order clarifying these errors.
Aims
The specific aim of this project was to improve patient safety by standardizing TPN solutions and the ordering process to reduce TPN errors from 22% to 5%. Sub-aim 1 was to decrease pharmacy TPN order processing time. Sub-aim 2 was to reduce patient laboratory draws. Sub-aim 3 was to implement regular use of standardized TPN solutions over customized solutions in eligible patients, with a goal of having 80% of patients given standardized TPN remaining on that formulation during the entire course of TPN treatment.
METHODS
This project was approved by our institutional review board in December 2013. This manuscript was prepared using the Standards for Quality Improvement Reporting Excellence guidelines for reporting of QI research.9
Context
Before project implementation, TPN orders were paper-based. Providers needed to individually order correct macro- and micronutrients, order electrolytes, calculate osmolarity and component compatibility for a solution to be without error. The order was faxed to the pharmacy by 10 am Pharmacy technicians contacted the ordering provider for clarifications, missing components, or corrections for incompatibility issues.
Study Design
Our project focused on shifting from paper to electronic TPN ordering, development of standardized TPN solutions based on multiple weight categories, and simplifying the TPN ordering process by TPN order sets including standardized laboratory orders for biochemical monitoring. For neonates, these order sets included a metabolic panel, magnesium, phosphate, and triglycerides on days 1 and 3, and then weekly after that. For pediatric patients, we obtained these studies on TPN days 1, 2, 3, and then semiweekly. A multidisciplinary group including neonatologists, pediatric intensivists, pediatric hospitalists, neonatal nurse practitioners, pharmacists, and nutritionists developed standardized TPN solutions for neonatal and pediatric patients using evidence-based nutrient requirements for each weight category and data from a published resource.10 The solutions were standardized for peripheral and central access, with caloric, nutritional, and fluid requirements tailored to weight-based categories (see Supplemental Digital Content at http://links.lww.com/PQ9/A33 for Appendix). After review by our pharmacists, the order entry was checked, and solutions were prepared daily at an off-site pharmacy.
Setting
Our institution is a large, freestanding, academic pediatric hospital. Seventy-one percentage of TPN orders were placed in units participating in this project. Errors were tracked during a baseline period of 66 days from November 2014 through January 2015 (Fig. 1).
Fig. 1.
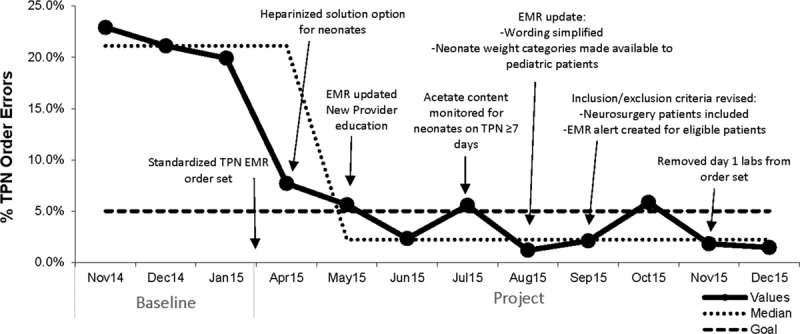
Run-chart of errors following implementation of standardized TPN. Errors in TPN ordering were tracked against standardized TPN utilization. Baseline data were collected between November 2014 and January 2015. Despite consistent use of standardized TPN with electronic ordering in eligible patients, the error rate remained low from the beginning of this project’s implementation.
Patient Population
This project included pediatric patients from birth to 21 years. Participating hospital units included the neonatal intensive care unit (NICU), pediatric intensive care unit, and general hospital wards. Neonates receive the majority of TPN solutions at our institution. The scope of the project was limited to NICU patients and patients on pediatric wards. We included neonatal patients born greater than 30 weeks gestation, weighing greater than 1,500 g, and who had not received TPN at another institution. We included pediatric patients neither receiving home TPN nor with electrolyte imbalances. We excluded patients in “critical” status, for example, weighing less than 1.5 kg, illnesses requiring frequent TPN manipulations, and renal failure requiring dialysis; those with complicated surgeries, such as major abdominal surgeries or neurosurgical shunt placements; and sepsis. We created ranges for laboratory values as withdrawal criteria, including serum glucose, sodium, potassium, bicarbonate, and calcium. Further exclusion criteria consisted of neonates with necrotizing enterocolitis or feeding intolerance, electrolyte imbalance, severe intrauterine growth restriction, abdominal wall defects, surgical or postoperative patients, or renal/endocrinologic issues. For pediatric patients, exclusion criteria consisted of electrolyte imbalance, home TPN, or renal/hepatic disorders. Patients meeting these discontinuation criteria or who, after starting standardized TPN subsequently did not meet inclusion criteria, were placed on customized TPN. Figure 2 illustrates utilization for both standardized and custom TPN solutions.
Fig. 2.
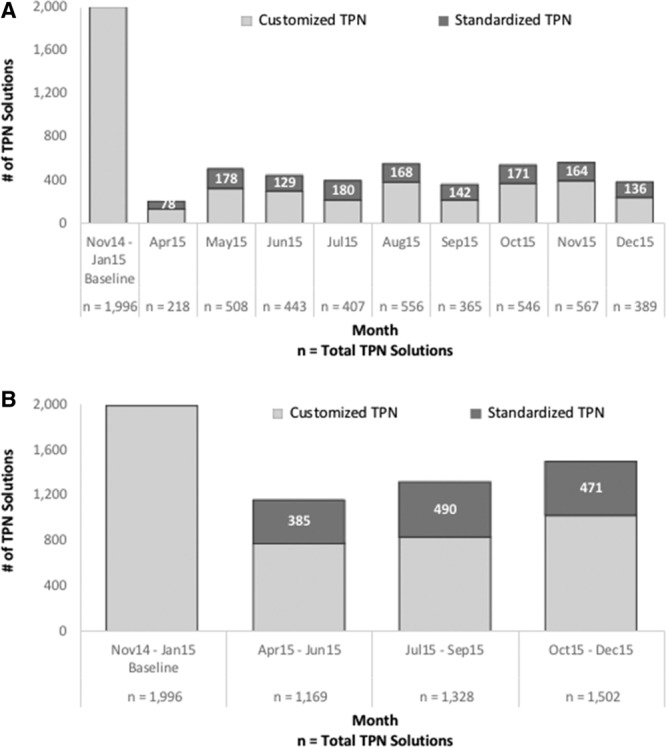
Utilization of standardized TPN for combined neonates and pediatric patients. Utilization of the standardized TPN composition was tracked for patients on TPN and meeting eligibility criteria. A, Illustrates breakdown of usage for standardized and customized TPN solutions for all patients receiving TPN during the study period, broken down by month. B, Illustrates utilization with the proportion of orders for standardized TPN given to eligible patients by quarter for comparison to baseline.
Intervention
We implemented 4 key interventions: (1) transitioning from paper to electronic ordering; (2) providing standardized TPN solutions; (3) creating predetermined laboratory draw schedules; and (4) having preset laboratory parameters. The implementation of electronic TPN ordering and the standardized formulations occurred at the onset of the project. We integrated the TPN solution compositions, patient criteria, and laboratory orders within the hospital’s electronic medical record (EMR).
We performed 4 Plan-Do-Study-Act (PDSA) cycles during the project. Each cycle assessed different outcomes from the standardized solutions while we monitored errors throughout the project. The preimplementation phase from January through March 2015 included a planning period and development of the EMR set. In the first phase, from March to May of 2015, standardized solutions with electronic ordering and monitoring were introduced and adjusted based on their impact on error rates. Before and throughout project implementation, neonatal nurse practitioners, pediatric residents, and neonatology fellows wrote all orders for TPN.
PDSA Cycles and Project Adjustments
In phases 1, 2, and 3, the EMR content was reconfigured based on errors found during PDSA cycles and user feedback regarding the use of the standardized electronic order sets and effectiveness of the standardized TPN solution. Based on this feedback, we expanded the laboratory value discontinuation criteria to a wider range of acceptable values. In phase 2, inclusion criteria were broadened to allow more patients to receive standardized TPN and we added an option for pediatric, nonneonatal patients weighing less than 10 kg. This phase evaluated the nutritional efficacy of the solutions. In phase 3, we monitored the number of blood draws over the first 7 days patients were on TPN. Phase 4 monitored maintenance of utilization.
Data Collection
We obtained baseline data from November 2014 to January 2015 by retrospective chart review.
Before project implementation, providers completed paper forms for TPN orders. Prescribers wrote on preprinted forms and scanned the completed form to the pharmacy. A clinical pharmacist reviewed and verified the order, individually documenting any clarification or revision by a clinical pharmacist. The pharmacists were not active participants in the project, therefore avoiding bias. The lead pharmacist would review the errors and report in data evaluation meetings and drill downs.
A 66-day review period was selected because our institution averaged 25–30 orders per day, which resulted in an estimated 1,500–1,800 orders to review. A time period longer than 1 month increased the number of prescribers because our medical teams change members at least monthly and ensured an adequate number of orders from each nursing unit. In total, 1,996 baseline TPN orders were reviewed, with 437 (21.9%) orders requiring pharmacist clarification.
The main outcome measure analyzed throughout the project was the TPN ordering error rate. We define a TPN error as any clarification and reentry of order needed before sending the order to the outside facility. These clarifications included calcium/phosphorous incompatibility; missing macro- or micronutrients; a glucose concentration inappropriate for the IV route; intolerable osmolarity; illegibility of handwritten orders; and blank or incorrect entries regarding patient weight, rate, or route of TPN administration.
Order processing time includes order writing, pharmacy review, and order correction. The project lead physician measured this by random audits of neonatal nurse practitioners writing TPN orders. The project lead pharmacist timed pharmacy technicians upon receipt of the faxed TPN order sheet, reviewing the ingredients requested, and, if necessary, calling the practitioner to correct the order. This process measurement occurred at quarterly time intervals throughout the project to track progress. We evaluated the impact on laboratory draws based only on those related to standard TPN solutions (ie, metabolic panels, magnesium, phosphate, and triglycerides in patients on TPN for at least 7 days.) The balancing measure of standardized solution effectiveness evaluated the number of patients on the standardized solutions requiring a switch to a custom solution.
We monitored data via a monthly dashboard of process and outcome measures. A small team of individuals performing EMR chart reviews performed prospective analysis throughout the project. Chi-square tests of independence and t tests for 2 independent samples were performed using IBM SPSS Version 23 software to compare TPN ordering error rates and the average number of blood draws, respectively. Run charts were created to track error rates for the standardized solutions with annotations for the multiple PDSA cycles (Fig. 1), and dashboards tracked utilization of standardized solutions for all patients and those meeting eligibility criteria (Fig. 2).
We did not monitor growth measures as the standardized solutions provided a calorie content and macro- and micronutrient breakdown suitable for patients based on their weight categories. Moreover, this was not a goal of the project as the majority of patients were not on TPN solutions for more than 1 week.
RESULTS
Ordering Errors
Implementation of standardized TPN with electronic ordering for eligible patients decreased TPN order errors from a baseline of 22% (n = 1996 orders) to 3.2% (n = 471 orders) in the last quarter of the study, representing an 85.4% reduction (Fig. 1). Ordering errors in NICU patients decreased from 25.5% (n = 1194 orders) to 3.4% (n = 322 orders) in the last 3 months of the project, an 86.7% reduction, whereas the pediatric ordering error rate fell from 19.7% (n = 208 orders) to 2.7% (n = 149 orders) during the same period. Chi-squared tests of independence revealed statistical significant in the overall group [χ2 (1, N = 2467) = 89.13, P < 0.001], and in the neonatal patient [χ2 (1, N = 1516) = 74.87, P < 0.001] and pediatric patient [χ2 (1, N = 357) = 22.85, P < 0.001] strata (Table 1).
Table 1.
Standardized TPN Order Error Rates

Order Processing Time
Average order writing time for clinicians dropped from 3.5 minutes to less than 1 minute at the project end. Time for pharmacist error clarification, correction, and processing for custom TPN was 10 minutes per order at baseline, compared with 5 minutes per standardized TPN order by project conclusion.
Reduction of Monitoring Laboratory Draws
Overall, the average number of blood draws for laboratory orders in the first week of standardized TPN administration was reduced from 6.2 (SD = 3.12) to 4.3 (SD = 2.13) in the last quarter of the study. This 30.9% drop in patients receiving TPN for a minimum of 7 days was statistically significant by t test for independent groups, t (506) = 5.97, P < 0.001. At baseline, neonates averaged 5.9 (SD = 2.48) laboratory draws in the first week of standardized TPN therapy, which decreased to a mean of 3.8 (SD = 1.61) draws over the last 3 months of the project. This 35.3% reduction was statistically significant, t (401) = 7.29, P < 0.001. The mean pediatric patient blood draws decreased from 7.5 to 6.3 (SD = 2.78) during this period. Although this change was not statistically significant with an alpha level of 0.05, t (103) = 1.18, P = 0.240, the 16.6% drop corresponds to a practically significant change with an average of 1 laboratory draw eliminated per pediatric patient in the first week of TPN administration (Table 2).
Table 2.
Mean Laboratory Draws in Neonatal and Pediatric Patients

Standardized Solution Utilization
We measured utilization of the new TPN composition by calculating the percentage of patients eligible for standardized TPN solutions who remained on that formulation throughout their TPN treatment. Efficacy of the standardized solutions was assessed by categorizing patients as those receiving only standardized TPN during their treatment versus those who were started on standardized TPN and later switched to customized TPN. After implementation, utilization ranged between 74 and 96% each month with 84% of the 304 eligible patients over the entire study period receiving only standardized solutions (Fig. 2).
DISCUSSION
This study used a multifaceted approach to decrease a significant number of errors in our institution involving TPN ordering. Our project focused on 4 key interventions: transitioning from paper to electronic ordering, providing standardized TPN solutions, creating standardized laboratory draw schedules, and having predetermined acceptable laboratory parameters. The combination of these interventions decreased TPN ordering errors (Table 1), improved time spent ordering and clarifying errors, and reduced the average number of blood draws (Table 2). It is also possible that a larger population of pediatric patients in the last quarter of the project (n = 21) might change the conclusion drawn from the t test performed for this group, due to the relationship between sample and effect sizes on P values. Further, the order set treated laboratory values outside the acceptable ranges as withdrawal criteria; the low frequency of patients switched to customized TPN reflects the low frequency of patients with abnormal laboratory studies.
Our multiple interventions focused on streamlining the ordering process by making it easier and faster, while reducing the likelihood of ordering errors, to enhance patient safety and outcomes. Despite order writing for TPN taking less than 1 minute to complete after implementation of this project, patients did not require excessive changes to standardized TPN, demonstrating the ability to enhance patient safety through this process.
Standardized electronic TPN ordering reduces ordering errors.3,8 Previous successful attempts to improve TPN administration have relied mostly on single interventions, such as standard ordering processes or standardized solutions. We believe our quality improvement project is the first to combine multiple interventions and demonstrate multiple positive outcomes including a significant decrease in TPN ordering errors, and the time to order TPN and correct errors. Other institutions have also demonstrated that adopting a standardized ordering and administration process for TPN led to a meaningful reduction of errors, less need for pharmacists to correct orders, and a more efficient ordering and administrating process leading to increased staff satisfaction.11 The majority of patients participating in this project were neonates admitted to our hospital’s 97-bed level 3 NICU. After completion of this project, we introduced the standardized TPN solutions and ordering process into additional units in our hospital. Given the success noted in the NICU, this may be a tool to manage parenteral nutrition in the neonatal population elsewhere as a means of error reduction. Our pediatric population experienced a milder reduction in errors, likely due to fewer eligible participants during the study period and less frequent use of TPN in that population at our institution.
Transitioning TPN ordering from paper to electronic form within the EMR eliminated a number of the errors previously encountered, including missing or illegible information, and calcium-phosphate compatibility issues. Incorporating lean sigma methodology like streamlining and simplification of the ordering process, minimizing variation, reducing waste, and eliminating overprocessing were highly impactful to the success of this project and may apply to a variety of other processes to maximize productivity and reduce the likelihood of errors.
Other benefits of standardizing TPN are patient satisfaction and cost savings. Though not the main outcome of this project, reducing the average number of blood draws likely reduces patient discomfort, decreases costs from unnecessary laboratory studies, and saves substantial patient blood volume, which is especially impactful for the neonatal population. Furthermore, standardized solutions reduce unnecessary micromanagement of TPN compositions by health care providers.4 Though not directly calculated, further cost benefits may result from less waste from duplicate or incorrect orders and time saved by pharmacists, nurses, and providers
Limitations
The TPN utilized by our hospital is made off-site. Providers must place orders by a certain time so the manufacturing company may later ship the product to the hospital. Standardizing TPN solutions allows for in-house stores of TPN, alleviating this time restriction.
This pilot study excluded newborns born less than 30 weeks gestational age, patients receiving TPN at home or another institution, and patients with complicated surgeries or sepsis. This project was successful in the NICU where a majority of TPN ordering occurs. We presented the results of the project in the hospital’s annual quality and research symposium and other division meetings including the Cardiovascular Intensive Care Unit and Hematology/Oncology. Plans are to have standardized solutions for patients weighing < 1,500 g for optimal nutritional efficacy crucial for this patient population.
Lastly, we did not monitor growth measures because calorie content and macro- and micronutrient breakdown were known to be suitable for patients based on their weight categories and the majority of patients were not on TPN solutions for more than 1 week. If the patients were nil per os (“NPO”) and receiving solely parenteral nutrition at 150 mL/kg/d, their nutritional needs by the standardized solution were calculated to meet their requirements appropriately. As enteral nutrition was advanced, we did not collect data to assess nutritional efficacy. This was beyond the scope of this project.
CONCLUDING SUMMARY
Transitioning to standardized TPN solutions and electronic ordering processes within the EMR eliminated or significantly reduced the number of TPN ordering errors. We also improved order processing time and the mean number of patient blood draws in the first 7 days of TPN administration. These outcomes occurred without negatively impacting utilization rates. During the sustainability phase of this quality improvement project, continued monitoring of standardized TPN utilization will allow reevaluation and modification if the utilization rate falls below the goal of 80%.
DISCLOSURE
The authors have no financial interest to declare in relation to the content of this article.
Supplementary Material
Footnotes
Published online July 27, 2018.
Presented at the American Academy of Pediatrics National Conference and Exhibition, October 2016—Podium Presentation (San Francisco, CA); Pediatric Hospitalist Medicine Conference, July 2016—Poster (Chicago, IL); Pediatric Academic Societies Conference, May 2016—Poster (Baltimore, MD); American Board of Medical Specialties Quality Improvement Forum, May 2016—Poster (Rosemont, IL); Florida Perinatal Quality Collaborative Conference, April 2016—Poster (Tampa, FL); Institute for Healthcare Improvement National Forum, December 2015—Poster (Orlando, FL); and Johns Hopkins All Children’s Hospital Research Symposium, October 2015—Poster (St. Petersburg, FL).
Supplemental digital content is available for this article. Clickable URL citations appear in the text.
To cite: Crews J, Rueda-de-Leon E, Remus D, Sayles R, Mateus J, Shakeel F. Total Parenteral Nutrition Standardization and Transition to Electronic Ordering to Reduce Errors: A Multifaceted Quality Improvement Initiative. Pediatr Qual Saf 2018;3:093.
REFERENCES
- 1.Krzyzaniak N, Bajorek B.Medication safety in neonatal care: a review of medication errors among neonates. Ther Adv Drug Saf. 2016;7:102–119.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chowdary KV, Reddy PN.Parenteral nutrition: revisited. Indian J Anaesth. 2010;54:95–103.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mackay MW, Cash J, Farr F, et al. Improving pediatric outcomes through intravenous and oral medication standardization. J Pediatr Pharmacol Ther. 2009;14:226–235.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Iacobelli S, Bonsante F, Vintéjoux A, et al. Standardized parenteral nutrition in preterm infants: early impact on fluid and electrolyte balance. Neonatology. 2010;98:84–90.. [DOI] [PubMed] [Google Scholar]
- 5.Lenclen R, Crauste-Manciet S, Narcy P, et al. Assessment of implementation of a standardized parenteral formulation for early nutritional support of very preterm infants. Eur J Pediatr. 2006;165:512–518.. [DOI] [PubMed] [Google Scholar]
- 6.American Society for Parenteral and Enteral Nutrition. ASPEN statement on parenteral nutrition standardization. JPEN J Parenter Enteral Nutr. 2007;31:441–448.. PMID 17712154. [DOI] [PubMed] [Google Scholar]
- 7.American Society for Parenteral and Enteral Nutrition (ASPEN) clinical guidelines: parenteral nutrition ordering, order review, compounding, labeling, and dispensing JPEN. JPEN J Parenter Enteral Nutr. 2014;38:334–377.. [DOI] [PubMed] [Google Scholar]
- 8.Brown CL, Garrison NA, Hutchison AA.Error reduction when prescribing neonatal parenteral nutrition. Am J Perinatol. 2007;24:417–427.. [DOI] [PubMed] [Google Scholar]
- 9.Revised Standards for Quality Improvement Reporting Excellence (SQUIRE).
- 10.Bunting KD, Mills J, Phillips S, et al. Pediatric Nutrition Reference Guide. Houston, TX, 20109th ed Texas Children’s Hospital; [Google Scholar]
- 11.Standardized ordering and administration of total parenteral nutrition reduces errors in children’s hospital. 2008. Seattle Children’s Hospital. AHRQ website. [Google Scholar]