

Abstract
This paper focuses on the basic principles of information technology (IT) organization within health sciences centers. The paper considers the placement of the leader of the IT effort within the health sciences administrative structure and the organization of the IT unit. A case study of the University of Missouri—Columbia Health Sciences Center demonstrates how a role-based organizational model for IT support can be effective for determining the boundary between centralized and decentralized organizations. The conclusions are that the IT leader needs to be positioned with other institutional leaders who are making strategic decisions, and that the internal IT structure needs to be a role-based hybrid of centralized and decentralized units. The IT leader needs to understand the mission of the organization and actively use change-management techniques.
Information technology (IT) organizations have been discussed in the literature of the Integrated Advanced Information Management System (IAIMS) grants since the inception of the IAIMS concept and the initial IAIMS grants. 1 If IAIMS plans are to be truly integrated across an entire health care institution, then the IT organization must be flexible enough to deal with computing cultures that are both centralized and decentralized, both liberal and conservative. This is a large challenge for most health care institutions. This article considers the basic principles of IT organization within the health sciences center, a topic that continues to be timely, although the trends and issues are more clearly defined than they were at the inception of the IAIMS concept.
Lorenzi and Riley 2,3 have written two books about organizational theory and leadership in health care IT.
They point out that health care institutions differ from many businesses in several respects, including personnel structure, life-and-death issues, alternative ownership characteristics, shareholders, exploding technologies and knowledge, rising costs and unique payment structure, and regulatory and accreditation requirements. The health care industry has tended to emphasize the uniqueness of its culture and mission, while ignoring its similarities to other large organizations. The result has often been an IT culture that is resistant to innovations and cross-fertilization from other institutions. This is a mistake. The health care industry has many important lessons to learn from the banking industry, the manufacturing industry, and other areas of U.S. business about how to organize IT and how to use it to compete more effectively.
Basic Principles of IT Organization
Two important aspects of IT organization that should be considered include the place of the IT organization in the health care institution and the internal structure of the IT organization. With regard to the first issue, it is my opinion that every health care institution and every integrated delivery system needs a chief information officer (CIO). (The specific titles of CIOs differ in various health science centers, but the title needs to be one that commands respect and is recognized as having top-level authority.) A CIO's responsibilities include 1) leadership of the IT organization and its policies, 2) technical management and services, 3) translation of institutional goals into IT efforts, 4) blending academic and business efforts, and 5) blending developmental efforts with traditional business software acquisition. In a health care institution, the CIO should be charged with bringing information to the point of decision making in all areas of education, research, patient care, and administration. The CIO must organize the existing patchwork quilt of IT groups that have evolved independently in most health centers into a unit that is capable of supporting the central mission of the health sciences center. The CIO's job is to determine how best to use technology to achieve institutional missions such as cutting costs, measuring patient outcomes, attaining research grants, educating students, and operating efficiently.
The questions invariably asked are what the scope of the central IT core group support should be and/or what units should be part of the central IT core group. There is no single correct answer. Each health care institution will have a variety of units supported by the central IT core organization. These units may be academic (e.g., the School of Medicine), business (e.g., the hospitals and clinics), or both. The central IT core organization may extend beyond traditional computing with such units as the telecommunications, printing services, multimedia production, or the health sciences library. The mixture of units supported and central core IT units will depend on the vagaries of each institution, its history, and its politics. The IT core group does not need to encompass all individuals with IT titles in all departments or units, but it must have a well-defined relationship with all IT personnel in all units of the institution. However, to maximize the potential for IT in achieving strategic goals, the IT leader needs to report to the key strategic leaders of the health care enterprise, to be in the meetings and discussions where strategic decisions are made, and to be recognized as setting the direction that must be followed by all other IT individuals and groups.
To turn to the principles of internal IT organization is to revisit the theme of centralized versus decentralized IT organizations. This theme is common across many years of literature, and the pendulum has swung in both extreme directions. The pendulum is now settling down in the middle. The Gartner Group, a national consulting firm specializing in IT issues, has stated, “By 1998, more than 70% of large enterprises will have radically restructured their IT. The result will be a blend of centralized and distributed computing.” 4 This is one of the basic tenets of a successful and flexible organization. The blend will depend on the roles and functions of the various types of computing support tasks.
Most importantly, the IT organization should fit the institution's strategic plan for using IT to accomplish its business priorities. In many health care institutions, education and research are business priorities just as much as clinical care is. The internal IT model that is rapidly emerging in the corporate world and the organizational literature in the 1990s is a group that is focused on service to the organization and distinguishes the service needed based on the technology role being delivered. Thus, the emerging model for IT is a blend of centralized and decentralized elements, called a structural hybrid organization.
A Case Study : The University of Missouri-Columbia Health Sciences Center
This report stems from a survey of many health sciences centers, many of which have formally received IAIMS grants, but it focuses on how the basic principles are brought to bear upon the IT organization of the University of Missouri—Columbia Health Sciences Center (MU-HSC). At MU-HSC, the IT organization has recently been repositioned in the organizational hierarchy. The primary internal IT groups (academic informatics research and support, hospital and clinics information services, and faculty practice plan data processing) have been merged to form one large IT support entity. The resulting unit, Integrated Technology Services, is headed by a chief information officer with an associate dean title who reports directly to the highest executive of the health sciences center (the dean of the School of Medicine and the director of Clinical Services). Integrated Technology Services provides services to the entire enterprise, including academic departments, hospitals, clinics, the physicians' practice plan, and affiliated providers. The services are those of infrastructure, user support, programming, application selection and support, data analysis, evaluation, architecture, research, and information resources.
The specific example of IT support for workstations, networks, and programmers may clarify the concept of role-based organizations. At the MU-HSC, a 1995 study of IT support showed that 45 people were directly involved in supporting the computer networks and electronic mail, although time-wise there were only 12 FTEs supporting networks and 4.5 FTEs supporting electronic mail. However, when the network went down, there was not a single person or group to contact to fix the network, since everyone was responsible but no single group was accountable. On further examination, it was found that many of the same 45 people were performing the roles of workstation support and computer programming. Half of these individuals were employed by individual academic departments and were not connected to the core IT units. There were, of course, some differences between the support and staffing in the hospital and clinics versus the academic school structures. As a result of this situation, the academic department chairs were unhappy because programming tasks were never finished. Even special critical projects remained unfinished. The principal reason was that the same person was responsible for the network and the electronic mail, which always took precedence over the programming projects because so many people needed networks and electronic mail to accomplish their jobs.
The role-based organizational model treats each of these roles separately. At MU, the roles are being separated and treated according to their enterprise-wide functions. The network and electronic mail have been declared mission-critical functions and moved to the top level of the enterprise. A completely centralized group that is responsible and accountable for these components has been created.
Workstation support is managed well as a shared-service hybrid function with joint funding between departments and the central IT group. The individual workstation-support specialists, who are based in the units they support, receive their priorities from their departments, yet are coordinated and trained as a group. The departments and the central IT group are jointly accountable for the performance of the individual, with the departmental group determining whether the individual is useful functionally and the central IT group determining whether the person's technical skills are adequate. Figure 1 shows an organizational chart for a shared-service hybrid relationship that was developed according to the model of the Gartner Group. 5
Figure 1.
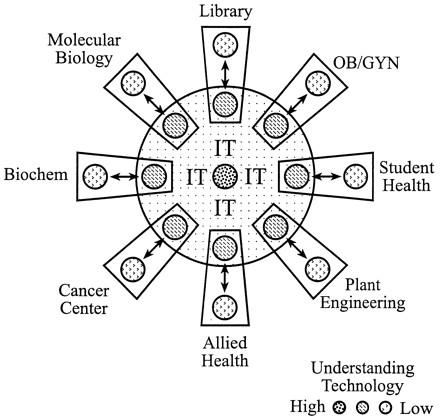
Organizational model for information technology support. This graph represents a shared-services hybrid organization between the central information technology group and departmental persons who are jointly funded to provide workstation support.
A coordinated model is used for the role of support for computer programmers (Figure 2). The central IT programming group focuses on computer programming and some core technologies (Oracle, C++, Java script, World Wide Web, Perl). This group takes on the enterprise-wide tasks as well as the responsibility to allow access to institutional data. This central group also assists all programmers in other units to understand the institutional data models or provides tips on the use of specific supported software or techniques. Direct programming responsibilities and funding remain in the decentralized units with accountability to the department or unit leaders unless the programming task is enterprise-wide or crosses unit or departmental boundaries.
Figure 2.
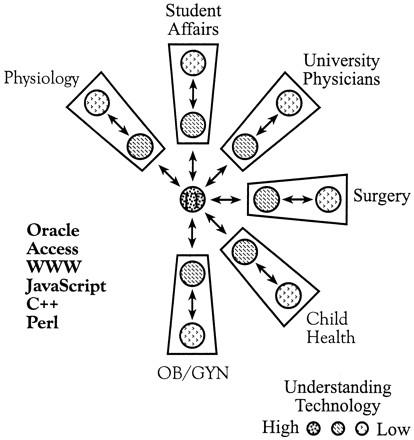
Organizational model for programming support. This graph represents a coordinated hybrid organization between the central information technology (IT) group and departmental programmers. The organizational model is more loosely coupled than the model for workstation support and illustrates the role-based approach to organization of IT.
The internal IT organization is hierarchical, but supports the institution as an integrated matrix (Figure 3), with each row in the matrix determining a different method of providing services to the units and departments depending on the specific role, as described above. Overall, the IT organization interacts and connects with every component of the health sciences center, with some roles totally centralized (networks), some roles pulled into shared services (workstation support), and some roles left primarily decentralized but with central coordination (unit programming).
Figure 3.
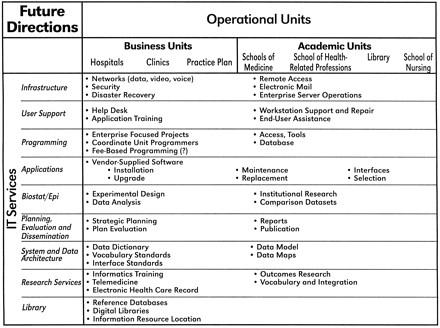
Matrix organization of information technology (IT) services provided by the central IT group to the operational units of the health sciences center. This chart represents the core services provided (infrastructure, user support, etc) and the components of the support that are provided to all of the units of the health sciences enterprise.
Other Issues
Other major issues are essential to an effective IT organization and are discussed elsewhere in this supplement, but need to be lightly touched upon here. The institution must determine how to fund this essential IT effort. The first step is to determine how much is currently allocated to IT activities. This amount is usually much more than anticipated. Then the leadership needs to determine how best to use this ongoing investment to support the IT plans and the institutional mission. A second major issue is to consider how best to manage change in the organization as it moves to a new organizational and work paradigm. A third challenge is to find an IT leader who understands the dynamics and the mission of the organization. Currently, few educational programs concentrate on IT leadership positions, and thus most leaders emerge from unusual, nontraditional career paths. A fourth major issue concerns communication both within and beyond the IT organization, since communication is essential but seldom adequate. A fifth issue relates to management across the subcultures that have arisen in health care organizations and how to blend these cultures into a cohesive IT unit. These are all issues identified by previous IAIMS conferences and the current one as “make it or break it” issues with which all institutions must grapple.
Conclusion
The overriding issues of the IT organization are : 1) the importance of IT to the future of a health care institution must be recognized by the institutional leaders ; 2) the IT leader must be positioned appropriately in the institution, with each organization being unique in some respects ; and 3) the internal IT organization must evolve into a blend of centralized, decentralized, and cooperative structures based on the specific IT function or role. The IT organization is not an end in and of itself. Rather, it must reflect the organization's mission. The IT leader needs to understand the organization's mission and how to use technology to achieve that mission. The IT leader also needs to manage the organizational changes needed to use technology and information resources as a strategic asset.
Presented in part at the IAIMS Consortium Symposium, Vanderbilt University, Nashville, TN, September 23, 1996.
Supported in part by National Library of Medicine Grant Number G08 LM05415-03.
References
- 1.Planning for Integrated Academic Information Management Systems : Proceedings of a symposium sponsored by the National Library of Medicine, October 17, 1984. Bethesda, MD : The Library, 1985.
- 2.Lorenzi NM, Riley RT. Organizational Aspects of Health Informatics : Managing Technological Change. New York : Springer-Verlag, 1995.
- 3.Lorenzi NM, Riley RT, Ball MJ, Douglas JV. Transforming Health Care through Information. New York : Springer-Verlag, 1995.
- 4.Gartner Group Research Note, May 1996.
- 5.Gartner Group Research Note, August 1996.