
Figure 4.
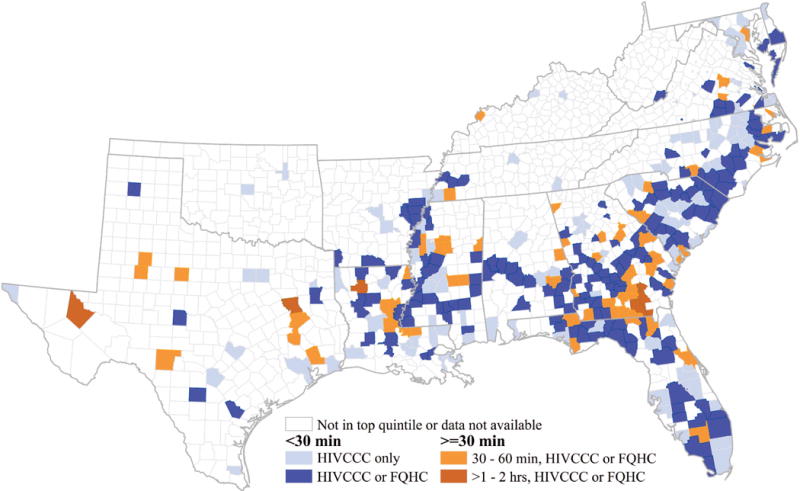
Reductions in travel time if federally qualified health centers (FQHCs) could offer HIVCCC in high-HIV burden Southern counties: an illustrative example
This county-level map of the US South shows changes in travel time when including federally qualified health centers, or FQHCs, as a potential source of HIV care for counties in the top HIV prevalence quintile. If comprehensive, coordinated HIV care were available at all FQHCs in the top HIV prevalence quintile either directly or through an alternative care model (e.g., telepartnership with an existing Ryan White clinic), an additional 170 counties in the top HIV prevalence quintile (shown in bright blue, ■) would have travel times to care under 30 minutes, a commonly used threshold. This represents a more than 230% increase in the number of counties (shown in light blue, ■) meeting the 30-minute travel time threshold. However, even when FQHCs are a potential source of HIV care, a small number of counties still have travel times that do not meet the optimal threshold, with travel times between 30 and 60 minutes shown in light orange (■) and >60 minutes shown in dark orange (■). Abbreviations: FQHC = federally qualified health center; HIVCCC = comprehensive, coordinated HIV care.