
Figure 1.
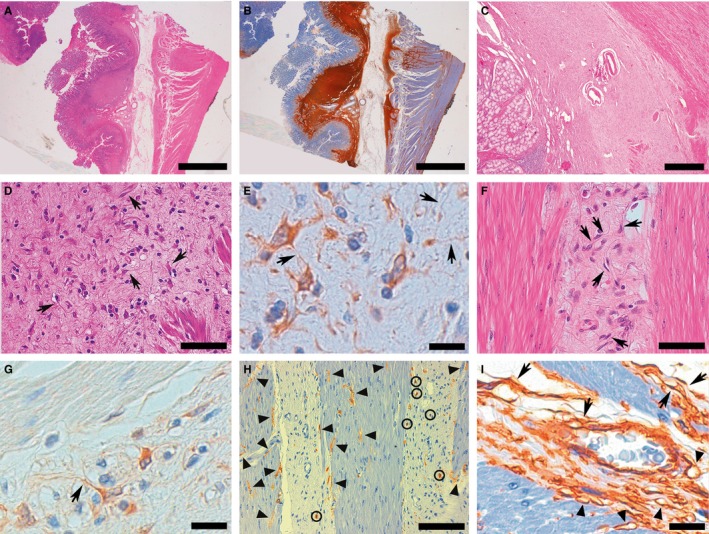
Representative examples of histological and immunohistochemical images of gastric TC hyperplasia found in PDGFRA‐mutant syndrome. A CD34+ stromal proliferation altered the structure of gastric wall, forming two thick bands along the inner and outer aspects of submucosa, sometimes forming ill‐defined nodules, and infiltrating the deeper wall layers with an interstitial pattern (A, H&E B, CD34). At times, the stromal proliferation obliterated submucosa (C). At higher magnification, the stromal proliferation consisted of spindle‐to‐polygonal PDGFRA+ TCs set in a variably collagenized background, often displaying slender, sometimes extremely long, cytoplasmic processes (telopodes), at times interconnecting with each other (arrows highlight some TCs whose telopodes are clearly evident due to the favourable intersection by the histological cutting surface) (D, H&E E, PDGFRA). The stromal proliferation with TCs (arrows, as in D and E) infiltrated muscularis propria with an interstitial pattern, separating smooth muscle fascicles, where no PDGFRA+ TCs are observed (F, H&E G, PDGFRA). CD117 demonstrated ICC‐IM, characteristically in close relation with smooth muscle fibres (arrowheads); mast cells (circled) were the only CD117+ cells populating the interstitial fibrosis (H). CD34 stained not only interstitial TCs (arrows), but also the endothelial lining of blood vessels: A small venule is evident at the centre of the picture; arrowheads indicate capillaries, identifiable because of their lumen (I). (Scale bars: A, B: 4 mm; C: 1 mm; D; 75 μm; E: 20 μm; F; 75 μm; G: 20 μm; H: 150 μm; I: 20 μm)