
Figure 3.
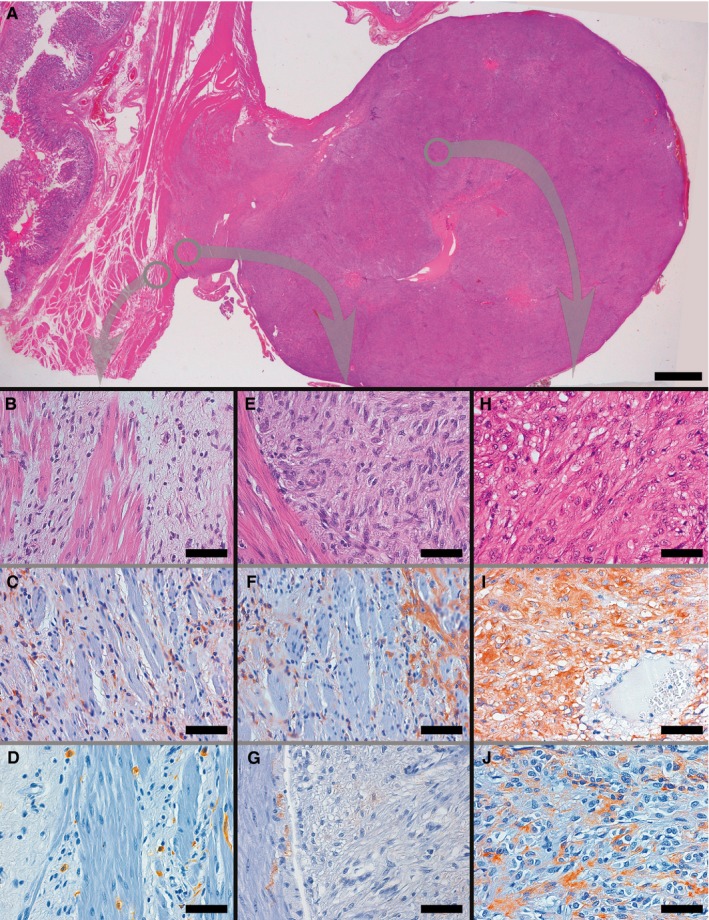
Representative examples of histological and immunohistochemical transition between TC hyperplasia and GIST found in PDGFRA‐mutant syndrome. The panoramic view shows a GIST originating from muscularis propria, whose smooth muscle bundles appear variously dissociated by the presence of interstitial TC hyperplasia, bulging on the external side of the gastric wall (A). As in Figure 2, higher magnification panels refer to areas encircled in grey in panel A, so as to underline the topographic location of the illustrated microscopic fields to better appreciate the transition between TC hyperplasia and GIST; corresponding areas are connected by arrows. Thin fibrous bands, populated by PDGFRA+ TCs, separate smooth muscle bundles near the periphery of GIST (B, H&E C, PDGFRA; D, CD117, highlighting ICC‐IM and mast cells). GIST (right) at the interface with muscularis propria (left) showed a relatively spindled cell cytology (E: H&E), and displayed an intense PDGFRA positivity (F), but only a weak and focal CD117 staining (G), thereby immunophenotypically resembling the neighbouring hyperplastic TCs rather than ICC‐IM. At a relative distance from the muscularis propria the GIST assumed a wholly epithelioid cytology (H, H&E), maintaining the intense PDGFRA immunoreactivity (I) and sometimes acquiring a comparatively strong positivity for CD117 (J). (Scale bars: A: 2 mm; B‐J: 65 μm)