

Abstract
Introduction:
This study was conducted to evaluate the safety and efficacy of fixed-dose combination (FDC) of rosuvastatin and choline fenofibrate in comparison to rosuvastatin and fenofibrate FDC among Indian patients of mixed dyslipidemia. This would be a first study evaluating FDC of rosuvastatin and choline fenofibrate in Indian population.
Methods:
A multicenter, open-label, randomized, active controlled, comparative, parallel-design study was conducted at 12 centers spread all across India. Mixed dyslipidemic patients aged 18–70 years were randomized to FDC of rosuvastatin 10 mg and choline fenofibrate 135 mg (RCF group) and FDC of rosuvastatin 10 mg and fenofibrate 160 mg (RF group) once daily for approximately 180 days. The primary endpoint of study was percentage change in serum triglyceride level at the end of study from baseline.
Results:
Of 290 patients screened, 240 patients were enrolled in this study (120 patients in each group). At the end of 180 days, there was a significant reduction in triglyceride level in both the groups (−37.7% in RCF group and −37.8% reduction in RF group; P < 0.0001 for both); however, the difference between both the groups was not statistically significant (P = 0.94). Similarly, there was significant increase (P < 0.0001 for both) in high-density lipoprotein cholesterol (HDL-C) in both groups (+17.8% in RCF group and +14.9% in rosuvastatin fenofibrate RF group). Low-density lipoprotein cholesterol (LDL-C), very low-LDL (VLDL-C), and total cholesterol were also reduced significantly in both groups (P < 0.0001). However, the difference between two groups for increase in HDL-C and decrease in LDL-C, VLDL-C, and total cholesterol was not significant. Both the treatments were safe and well tolerated.
Conclusion:
Overall, FDC of rosuvastatin and choline fenofibrate is as safe and effective as rosuvastatin and fenofibrate combination in Indian patients with mixed dyslipidemia with added advantage improved patient compliance as it can be taken irrespective of intake of food.
Keywords: Choline fenofibrate, fenofibrate, Indian, mixed dyslipidemia, rosuvastatin
INTRODUCTION
Mixed or atherogenic dyslipidemia is characterized by abnormal lipid triad consisting of low levels of high-density lipoprotein cholesterol (HDL-C), high levels of triglycerides (TG), and low-density lipoprotein cholesterol (LDL-C), especially small and dense LDL-C particles which are more atherogenic in nature. It is widely prevalent in general population, especially in obese patients with metabolic syndrome and in patients with diabetes mellitus.
Although current lipid treatment guidelines target LDL-C as the primary substrate for cardiovascular risk reduction,[1] a substantial residual cardiovascular risk persists even when LDL-C reaches the recommended target levels. This residual risk may be attributed to presence of other lipid abnormalities of atherogenic dyslipidemia.
Rosuvastatin in combination with fenofibrate has demonstrated marked reductions in multiple lipid parameters in combined hyperlipidemia. Choline fenofibrate is a new (choline) salt of fenofibric acid (active moiety) which offers certain advantages such as better bioavailability and no interactions with food.
Earlier in a trial, we have demonstrated that choline fenofibrate is as effective and safe as micronized fenofibrate in mixed dyslipidemia among Indian population.[2] The present study was planned to evaluate the efficacy and safety of fixed dose combination (FDC) of choline fenofibrate and rosuvastatin in comparison to rosuvastatin and fenofibrate combination among Indian patients of mixed dyslipidemia.
METHODS
Study design
This multicenter, open-label, randomized, active-controlled, comparative, parallel group study was carried out at 12 centers spread all across India after obtaining approval from the Office of Drug Controller General (India) and respective ethics committee at each site. The study was conducted according to the study protocol following the ethical guidelines by ICMR. It was registered prospectively in (clinical trial registry-India/2014/02/004417).
Study population
A total of 240 patients with mixed dyslipidemia of either gender, aged 18–70 years having serum triglycerides levels between 150 mg/dl and 500 mg/dl, serum LDL-C >100 mg/dl and serum HDL-C <40 mg/dl for men and <50 mg/dl for women were enrolled in the study. The primary exclusion criteria included active liver disease, preexisting gallbladder disease, renal dysfunction, type 1 diabetes mellitus, thyroid dysfunction, and treatment with fenofibrate/choline fenofibrate in last 1 month.
Treatment groups
Patients meeting eligibility criteria were enrolled in the study and randomized in 1:1 ratio to receive once daily treatment with either FDC of rosuvastatin 10 mg and choline fenofibrate 135 mg or FDC of rosuvastatin 10 mg and fenofibrate 160 mg as per computer-generated randomization sheet. There were total six visits for each patient as follows: screening visit, randomization visit, 3 follow-up visits (visit 3–45 ± 4 days, visit 4–90 ± 4 days, and visit 5–135 ± 4 days) and end of study visit (180 ± 4 days).
Enrolled patients were provided allocated study medications at randomization and then during follow-up visits. Hematology, clinical chemistry, lipid profile, urine analysis, serum pregnancy test (for female patients), and standard 12-lead electrocardiogram recording were performed at screening and at study completion or exit from the study to assess safety of the patients. Lipid parameters at screening visit were considered as baseline values. In addition, lipid profile (Total cholesterol, LDL-C, TG, HDL-C, and VLDL-C); and serum AST (aspartate aminotransferase), ALT (alanine aminotransaminase) and CPK (creatine phosphokinase) were performed at visit 3, 4, and 5.
Primary and secondary endpoints
The primary endpoint was percentage change in serum triglycerides at the end of study as compared to baseline. The secondary efficacy endpoints were percentage changes in serum HDL-C, serum LDL-C, serum VLDL-C, and total cholesterol at the end of study as compared to baseline. The following safety parameters were also evaluated: Any adverse events that were reported voluntarily, observed, and enquired during the study; any clinically significant change in the value of laboratory results, vital signs, and physical examination during the study compared to baseline.
Statistical analysis
The sample size was determined based on the triglyceride reduction in the rosuvastatin 10 mg/fenofibrate group from baseline to week 24 reported by Durrington et al.[3] It was estimated that the planned sample size of 100 patients per treatment arm would provide >80% power to detect a difference of 12% with a standard deviation of 30 in the serum triglyceride considering two-sided pooled t-test with significance level 0.05 between two groups. This study was planned to enroll approximately 240 patients assuming 20% dropout. Electronic case report forms were used to collect information during the trial. Mean percentage change in serum triglycerides, HDL-C, and LDL-C at the end of treatment from baseline were statistically evaluated within groups and between the groups by student's t-test/Wilcoxon test depending on the distribution of data. Within-group and between-group comparisons for other laboratory results were analyzed using Chi-square (χ2) test or Fisher exact test. The occurrence of commonly reported (>1% of patients) adverse events were analyzed using Chi-square test for between groups statistical significance. Statistical significance was considered at 0.05 level. Efficacy analysis was carried out on primary and secondary efficacy endpoints, and safety analysis was carried on safety parameters using SAS® Version 9.3 (SAS Institute Inc., USA).
RESULTS
Out of 290 patients screened across all the sites, a total of 240 patients were enrolled in the study (120 patients in each arm) which was included in safety analysis [Figure 1]. Of these, 228 patients who received at least one dose of study medication and completed one or more follow-up assessments were included for modified intention to treat principle analysis (117 patients in rosuvastatin choline fenofibrate (RCF) group and 111 patients in rosuvastatin fenofibrate [RF] group). A total of 215 patients who completed the study (110 patients in RCF groups and 105 patients in RF group) were included in per protocol analysis.
Figure 1.
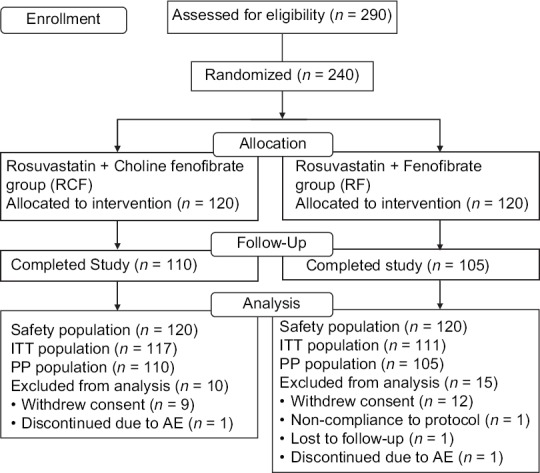
Study flow diagram
Baseline characteristics
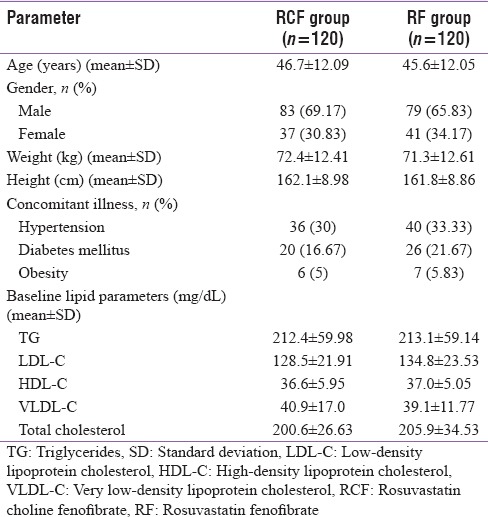
Patients from both groups had matching baseline characteristics in terms of age, gender, weight, height, concomitant illness, and baseline lipid parameters [Table 1].
Table 1.
Baseline characteristics
Primary endpoint
There was a significant reduction in serum TG levels at all timepoints throughout the study period in both groups with respect to baseline value (P < 0.0001). Serum TG level was reduced by approximately 37.7% in RCF group as compared to 37.8% reduction in RF group at the end of study. However, the difference between groups was not statistically significant (P = 0.94). With both investigational products, a large percentage of reduction was evident at day 45 after initiation of therapy. This reduction was increased till the end of study in both treatment groups [Figure 2].
Figure 2.
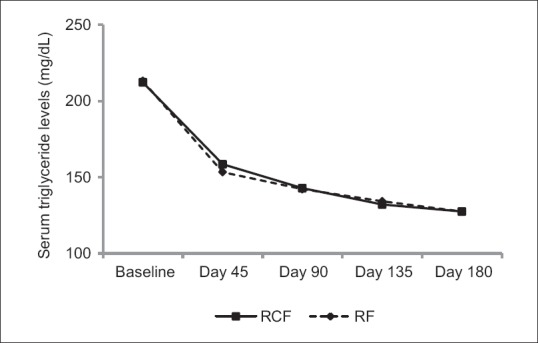
Change in serum triglyceride level in both study groups
Secondary endpoints
There was a significant increase in serum HDL-C levels at all timepoints throughout the study in both the groups as compared to their baseline values (P < 0.0001). Serum HDL-C level was increased by approximately 17.8% in RCF group as compared to 14.9% increased in micronized fenofibrate group at the end of study; however, the difference between groups was not statistically significant (P = 0.39) [Figure 3]. Rise in serum HDL-C level was observed as early as on day 45 and incremental effect was recorded throughout the study period in both groups.
Figure 3.
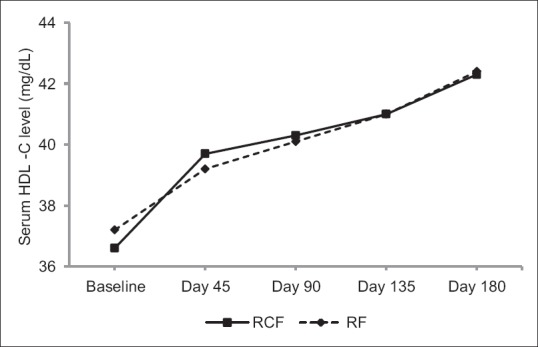
Change in serum HDL-C levels in both study groups. HDL-C: High-density lipoprotein cholesterol, mg/dL: milligram per deciliter
LDL-C, VLDL-C, and total cholesterol also reduced significantly in both the groups (P < 0.0001); however, the difference between both groups was not statistically significant [Table 2].
Table 2.
Change in other lipid parameters from baseline

Safety
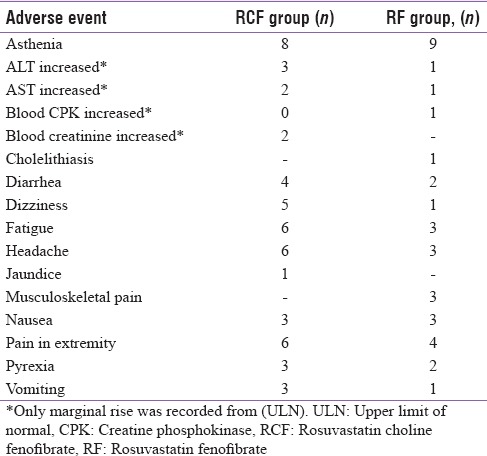
A total of 130 adverse events were recorded during entire study; out of which, 114 adverse events were mild in nature. Most commonly reported adverse events during the conduct of study were asthenia, pain in extremity, fatigue, headache, and dizziness [Table 3]. Three serious adverse events (SAEs) requiring hospitalization of patients were reported during study; however, all three SAEs were resolved without any sequelae.
Table 3.
Frequently observed/important adverse events during study
DISCUSSION
Addition of fenofibrate to statin therapy offers the prospective for overall lipid control in patients with mixed dyslipidemia.[3,4,5] Although FIELD and ACCORD studies were not able to demonstrate significant reduction in the rate of coronary heart disease with fenofibrate, subgroup analysis of patients with triglyceride level ≥204 mg/dL and HDL-C level ≤34 mg/dL from five major fibrate versus placebo trials (including FIELD and ACCORD) demonstrated up to 35% reduction in cardiovascular events.
Fenofibrate is poorly soluble in water, which adversely affects their absorption from the intestine and thereby, its bioavailability. In addition, fenofibrate 160 mg tablets are recommended to be given along with fat-rich food to facilitate their absorption.[6] However, current lipid treatment guidelines recommend low-fat food for patients with dyslipidemia.[1] Further, change in fat content of diet may lead to inconsistent, unpredictable, and suboptimal bioavailability.
Choline fenofibrate is water soluble in nature which does not have such interaction with food.[7] It rapidly dissociates in intestine and release fenofibric acid (active moiety) which is well absorbed throughout all the gastrointestinal regions, and thereby, improving its bioavailability.[8] Therefore, compared to rosuvastatin and micronized fenofibrate combination, FDC of rosuvastatin, and choline fenofibrate can be considered as a better alternative with consistent and superior bioavailability.
Therefore, the present study was initiated to evaluate the efficacy and safety of FDC of rosuvastatin and choline fenofibrate. The results of study indicated that rosuvastatin and choline fenofibrate combination provides significant reduction in the serum triglycerides levels similar to rosuvastatin and micronized fenofibrate combination (37.7% vs. 37.8%, respectively). Similarly, increase in HDL-C as well as reduction in LDL-C, VLDL-C, and total cholesterol was also similar in both the groups.
A study evaluating safety and efficacy of fixed-dose combination of rosuvastatin 10 mg and choline fenofibrate 135 mg demonstrated changes in triglyceride, LDL-C, and HDL-C levels upto −44.6%, −46.0%, and +14.0%, respectively.[9] Similarly, in a phase III, clinical trial evaluating safety and efficacy of concomitant use of rosuvastatin 10 mg and choline fenofibrate 135 mg, changes in triglyceride, LDL-C, and HDL-C was noted −47.1%, −37.2, and +20.3, respectively.[10] However, the possible explanation for higher reduction achieved in this study for triglyceride and LDL-C can be the higher baseline values in this published trial compared to our study.
Majority of adverse events reported in study were mild in nature. Few patients reported rise in liver enzymes (AST or ALT), CPK, and serum creatinine. However, the values of same were only marginally increased from upper limit of normal and have no substantial clinical effects. One patient developed cholelithiasis in RF group and one developed jaundice requiring hospitalization in RCF group; however, both serious adverse events were considered to be not related to study drugs as per investigator assessment since they occurred with short duration of treatment, not proving temporal relationship. Overall, both the combinations were safe and tolerated.
CONCLUSION
Overall, results of the current study concluded that FDC of rosuvastatin and choline fenofibrate is as safe and effective as rosuvastatin and micronized fenofibrate combination in Indian patients with mixed dyslipidemia. Both study drugs were well tolerated and provided comprehensive improvement in abnormal lipid profile of mixed dyslipidemia. The FDC of rosuvastatin and choline fenofibrate offers a better alternative to patients with mixed dyslipidemia.
Financial support and sponsorship
This study was funded by Intas Pharmaceuticals Limited, Ahmedabad.
Conflict of Interest
Dr. Hanmant Barkate and Dr. Piyush Patel are the employees of Intas Pharmaceuticals Limited. Dr. Falgun Vyas and Dr. Dimple Shah are the employees of Lambda Therapeutic Research Limited.
Acknowledgment
We would like to acknowledge the contribution of the following investigators in conduct of this research study: Dr. Anil R. Jain, Dr. Rajan V. Modi, Dr. Vinay Bhomia, Dr. Uday Narayan Sarkar, Dr. Chopda Manojkumar Bhavarilal, Dr. Bhatia Girish Gokuldas, Dr. Chetan Shridhar Patil, Dr. Mullasari Ajit, Dr. Ezhilan Janakiraman, Dr. N Vijaya Kumar, Dr. Laxmikant Goyal, Dr. J. Damodharan, Dr. Aditya Kapoor and Dr. Abhay Gupta.
REFERENCES
- 1.Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:2889–934. doi: 10.1016/j.jacc.2013.11.002. [DOI] [PubMed] [Google Scholar]
- 2.Patel P, Barkate H. Comparison of efficacy and safety of choline fenofibrate (fenofibric acid) to micronized fenofibrate in patients of mixed dyslipidemia: A randomized, open-label, multicenter clinical trial in Indian population. Indian J Endocrinol Metab. 2016;20:67–71. doi: 10.4103/2230-8210.172243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Durrington PN, Tuomilehto J, Hamann A, Kallend D, Smith K. Rosuvastatin and fenofibrate alone and in combination in type 2 diabetes patients with combined hyperlipidaemia. Diabetes Res Clin Pract. 2004;64:137–51. doi: 10.1016/j.diabres.2003.11.012. [DOI] [PubMed] [Google Scholar]
- 4.Athyros VG, Papageorgiou AA, Athyrou VV, Demitriadis DS, Kontopoulos AG. Atorvastatin and micronized fenofibrate alone and in combination in type 2 diabetes with combined hyperlipidemia. Diabetes Care. 2002;25:1198–202. doi: 10.2337/diacare.25.7.1198. [DOI] [PubMed] [Google Scholar]
- 5.Grundy SM, Vega GL, Yuan Z, Battisti WP, Brady WE, Palmisano J, et al. Effectiveness and tolerability of simvastatin plus fenofibrate for combined hyperlipidemia (the SAFARI trial) Am J Cardiol. 2005;95:462–8. doi: 10.1016/j.amjcard.2004.10.012. [DOI] [PubMed] [Google Scholar]
- 6.TRICOR Laboratoires Fournier, S.A 21300 Chenôve, France. 2014. [Last accessed on 2016 Jul 25]. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2014/021203s005lbl.pdf .
- 7.TRILIPIX AbbVie Inc. North Chicago, IL 60064, U.S.A. 2015. [Last accessed on 2016 Jul 25]. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/022224Orig1s011lbl.pdf .
- 8.Zhu T, Ansquer JC, Kelly MT, Sleep DJ, Pradhan RS. Comparison of the gastrointestinal absorption and bioavailability of fenofibrate and fenofibric acid in humans. J Clin Pharmacol. 2010;50:914–21. doi: 10.1177/0091270009354995. [DOI] [PubMed] [Google Scholar]
- 9.Roth EM, McKenney JM, Kelly MT, Setze CM, Carlson DM, Gold A, et al. Efficacy and safety of rosuvastatin and fenofibric acid combination therapy versus simvastatin monotherapy in patients with hypercholesterolemia and hypertriglyceridemia: A randomized, double-blind study. Am J Cardiovasc Drugs. 2010;10:175–86. doi: 10.2165/11533430-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 10.Jones PH, Davidson MH, Kashyap ML, Kelly MT, Buttler SM, Setze CM, et al. Efficacy and safety of ABT-335 (fenofibric acid) in combination with rosuvastatin in patients with mixed dyslipidemia: A phase 3 study. Atherosclerosis. 2009;204:208–15. doi: 10.1016/j.atherosclerosis.2008.09.027. [DOI] [PubMed] [Google Scholar]