

Abstract
Candy cane syndrome is a rare complication reported in bariatric patients following Roux-en-Y gastric bypass. It occurs when there is an excessive length of roux limb proximal to gastrojejunostomy, creating the possibility for food particles to lodge and remain in the blind redundant limb. Patients present with non-specific symptoms such as abdominal pain associated with nausea and vomiting. Most remain undiagnosed as the disease process is poorly described. We report three cases of candy cane syndrome treated successfully at our institution.
BACKGROUND
Laparoscopic Roux-en-Y gastric bypass (LRYGB) surgery is the most common surgery performed in USA for weight loss. Even though, it is considered one of the safest surgical procedure, rare complication such as candy cane syndrome can occur, leading to debilitating symptoms which are difficult to diagnose and manage [1]. Pathophysiology in candy cane syndrome is related to redundant roux length at the time of creation of gastrojejunosotmy which serves as a blind pouch for the food to stay. Treatment is centered on minimizing the redundancy and shorting the excessive length of roux limb proximal to gastrojejunosotmy.
CASE SERIES PRESENTATION
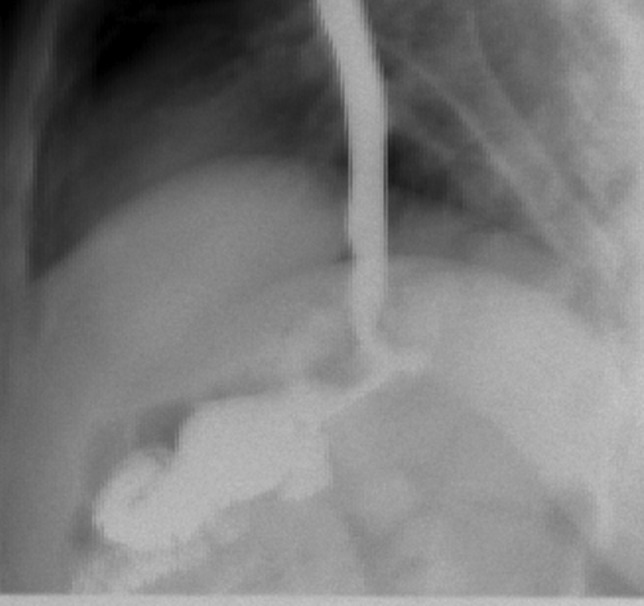
A 44-year-old female with BMI 25.5 with history of hepatic cirrhosis, upper GI bleed, GERD underwent LRYGB in March 2016, ventral hernia repair 2016. She presented to the clinic 1 year post 81 pounds weight lost since surgery with chronic colicky abdominal pain associated with nausea and vomiting. Vital signs were stable. On physical exam, she had tenderness in the right side of her abdomen and epigastric area. All the labs findings were unremarkable. Prior to this visit patient had an esophagogastroduodenoscopy (EGD) which was also negative. CT scan of abdomen shows hepato-splenomegaly with periappendiceal fat stranding and dilated appendix. Patient was taken to the operating room for diagnostic laparoscopy and appendectomy in April 2017 and was found to have candy cane syndrome. We resected excessive redundant (4 cm length) of the long blind jejunal loop of gastrojejunostomy anastomosis using Endo GIA Tri-Stapler device. Post-operative patient had upper GI which was normal (Figs 1 and 2). Post-operative course was uneventful. The patient was discharged to home on post-operative Day 2 and returned to clinic 2 weeks for follow up and tolerating diet and completely pain free.
Figure 1:
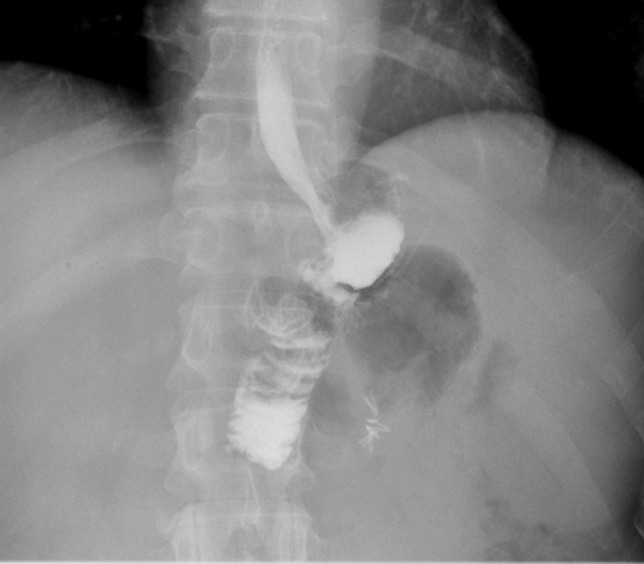
Post-op upper GI, was normal.
Figure 2:

Post-op upper GI after resection of redundant limb.
Second patient is a 35-year-old female with BMI 32.3 of with history of diabetes mellitus, hyperlipidemia who underwent LRYGB in June 2014, laparoscopic cholecystectomy 2014 was seen in the clinic for 1 year follow up. After having lost 54 pounds with right sided abdominal pain associated with nausea and vomiting. Patient had an upper GI which was negative and subsequently still continue to have the abdominal pain and undergone an EGD which was normal as well. At that point patient was lost to follow up for over a year as she moved to Florida and states while in Florida had CT scan of abdomen which showed questionable internal hernia at the anastomosis. Patient was seen and evaluated in our emergency room with complaints of right sided abdominal pain with nausea and vomiting. Vital signs were stable. On physical exam, tenderness in the epigastric area. All the labs findings were unremarkable. CT scan of abdomen did not show any abnormality. However, due to possibility for an internal hernia, patient was admitted and was taken to the operating room for diagnostic laparoscopy on November 2017. She was found to have long candy cane limb. We resected excessive redundant 4 cm length of the long blind jejunal loop of gastrojejunostomy anastomosis using Endo GIA Tri-Stapler device, Intra-op EGD was performed showing 4 cm gastric pouch. Post-operative course was uneventful. The patient was discharged to home on post-operative Day 4 and returned to clinic 1 week for follow up and tolerating diet and completely asymptomatic and pain free. Three weeks post laparoscopy patient had upper GI which was found to be normal (Figs 3 and 4).
Figure 3:
Patient post-op upper GI was normal after resection.
Figure 4:
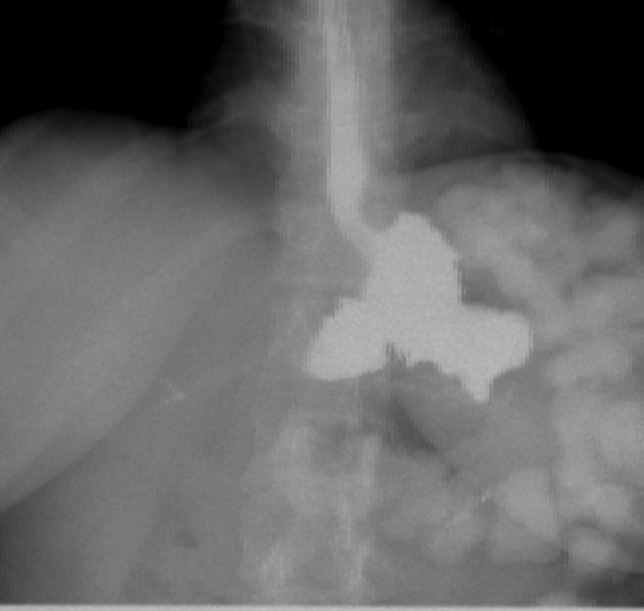
Patient post-op upper GI after resection.
Third patient is a 26-year-old female with BMI 25.1 of with history of morbid obesity who underwent LRYGB in June 2017 was seen in the clinic for 6 month follow-up after having lost 87 pounds with right upper quadrant abdominal pain associated with on/off nausea and vomiting. Prior to this visit, patient had visited outside hospital where they did CT scan of abdomen which was negative. In addition patient also had abdomen US, showed acalculus cholecystitis with gallbladder wall edema. Patient was taken to the operating room for diagnostic laparoscopy and cholecystectomy February 2018 with Intra-op EGD showing long candy cane limb. We resected excessive 5 cm length of the long blind jejunal loop of gastrojejunostomy anastomosis using Endo GIA Tri-Stapler device and cholecystectomy with Intra-op EGD show no ulcers and smaller stomach pouch. Post-operative course was uneventful. The patient was discharged to home on post-operative Day 3 and returned to clinic 1 week for follow up and tolerating diet and without symptoms.
DISCUSSION
Since the first laparoscopic gastric bypass in 1993 several studies have proven the safety of this procedure. Candy Cane limb syndrome is a difficult diagnosis to make after a patient undergoes LRYGB surgery. With good history and physical exam along with diagnostic work up is preponderant to treating this syndrome upper gastrointestinal study and endoscopy (EGD) are the diagnostic studies used to diagnose this syndrome. The symptoms that could be suspicious for candy cane syndrome are reported from as early as 3 months to up to 11 years [2, 3]. All of our patients presented with chronic abdominal pain, the cause of which was negative on routine imaging studies. A high level of suspicion is required to diagnose a candy cane syndrome. The length of the blind loop is reported to be between 3 and 22 cm [4]. Re-operations after bariatric surgery are usually necessary due to failure of weight loss, weight regain or secondary to complications. LRYGB fails in between 15 and 33% of the cases [1, 4]. Of the failures only up to 20% will require second operation [5]. In order to avoid occurrence of candy cane syndrome, bariatric surgeons should decrease the length of the blind loop and reposition by directing towards right side by allowing gravitational drainage and obviate the problems in the jejunojejunal anastomosis which cause backward enlargement of the Roux-en-Y limb [6].
CONCLUSION
Candy cane or afferent limb syndrome is an under-reported complication of Roux-en-Y gastric bypass. A high level of suspicion is required to diagnose a candy cane syndrome. Keeping the redundancy afferent limb shorter in primary LRYGB can prevent candy cane syndrome. Prompt diagnosis and laparoscopic resection of afferent blind limb can lead to favorable outcome to treat ‘Candy Cane’ syndrome and can provide symptomatic relief for the patient [2]. Having excessive length >4 cm of afferent limb should undergo surgical resection.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
- 1. Lee M, Lyass S ‘Candy Cane’ Redundant Roux Syndrome After Gastric Bypass. UT Southwestern Medical Center, Dallas, Cedars Sinai Medical Center. SAGES.
- 2. Aryale AH, Fayezizadeh M, Wen Y, Alshehri M, Abbas M, Khaitan L. Candy cane syndrome. An underappreciated cause of abdominal pain and nausea after Roux en Y gastric bypass surgery. Surg Obes Relat Dis 2017;13:1501–5. 10.1016/j.soard.2017.04.006. [DOI] [PubMed] [Google Scholar]
- 3. Dallal RM, Cottam D. ‘Candy cane’ Roux syndrome—a possible complication after gastric bypass surgery. Surg Obes Relat Dis 2007;3:408–10. [DOI] [PubMed] [Google Scholar]
- 4. Kellogg TA. Revisional bariatric surgery. Surg Clin North Am 2011;91:1353–71. [DOI] [PubMed] [Google Scholar]
- 5. Edholm D, Svensson F, Näslund I, Karlsson FA, Rask E, Sundbom M Long term results 11 years after primary gastric bypass in 384 patients. Surg Obes Rel Dis, 2013; 9: 708–13. [DOI] [PubMed] [Google Scholar]
- 6. Romero-Mejía C, Camacho-Aguilera JF, Paipilla-Monroy O. ‘Candy cane’ Roux syndrome in laparoscopic gastric by-pass. Cir Cir 2010;78:347–51. Spanish. [PubMed] [Google Scholar]