
Figure 1.
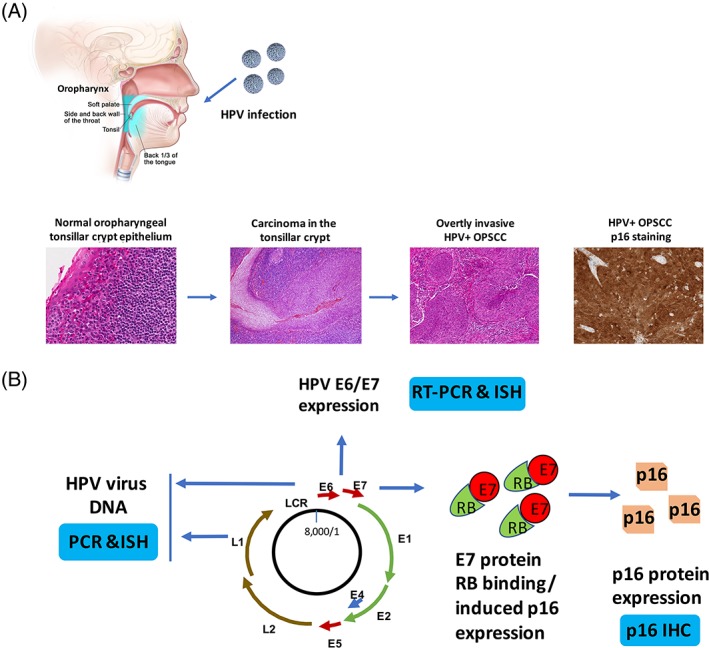
HPV‐associated carcinogenesis of head and neck cancer and molecular diagnostic tests. (A) The process of HPV‐related head and neck cancer development. HPV is contracted and introduced to the oral cavity and oropharynx. The susceptibility of the reticulated tonsillar crypt epithelium leads to the development of persistent viral infection and carcinogenesis, with neoplastic transformation of squamous cells in the epithelium that then expand the surface and eventually invade into the surrounding stroma and lymphatics, metastasizing to LNs early in the disease course. The tumor cells are strongly and diffusely positive for p16 by IHC with both nuclear and cytoplasmic staining. The top figure depicts the anatomy of oropharynx, including soft palate, lateral and posterior walls of the oropharynx (side and back wall of the throat), palatine tonsil (tonsil), and base of tongue (back 1/3 of the tongue). The histological images represent normal oropharyngeal tonsillar crypt epithelium (×300, left), carcinoma in the tonsillar crypt (×200, second left), overtly invasive HPV+ OPSCC (×100, second right), and HPV + OPSCC p16 IHC staining (×200, right). (B) Illustration of molecular diagnostic tests based on the HPV genome, E6/E7 gene expression and overexpression of p16 protein. The HPV viral genome is presented that the viral DNA can be detected by PCR or ISH (left). When HPV virus in its transcriptionally active form, the E6 or E7 gene can be detected by RT‐PCR or RNA ISH (top). HPV viral gene expression leads to abundant E7 protein overexpression with binding to Rb and mediating to its degradation. This allows for massive overexpression of p16 protein which is then detectable by IHC (right bottom). E: early genes; L: late genes; LCR: Long control region.