
Figure 1.
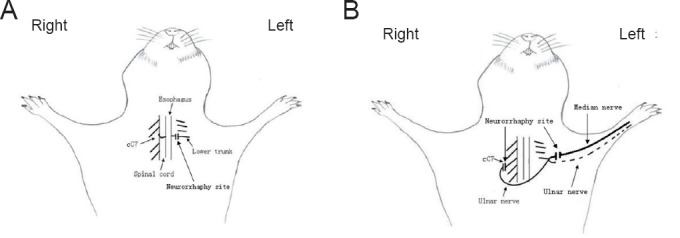
Schematic diagrams of contralateral C7 (cC7) root transfer to the lower trunk vs. the median nerve for the repair of total brachial plexus injury.
(A) Modified cC7 root transfer to the lower trunk: the C7 nerve root was separated and cut off at the division-to-cord level. The prespinal route was made along the anterior vertebral body by bluntly dissecting the sternocleidomastoid muscle and carotid sheath along their medial margin and severing the right anterior scalene muscle. The cC7 root was passed through the tunnel to the injured side. The coaptation was made utilizing end-to-end neurorrhaphy. (B) Traditional cC7 root transfer to the median nerve: the left pedicular vascularized ulnar nerve grafts were dissected, and the distal end was severed at the wrist level, moved to the contralateral side through the ventral thoracic subcutaneous tunnel and connected to the proximal cC7 root. Four weeks later, the ulnar nerve graft and median nerve were dissected and cut off from an incision at the middle of the injured arm. The distal stump of the ulnar nerve graft was coapted to the distal end of the median nerve with end-to-end neurorrhaphy.