
Fig. 3.
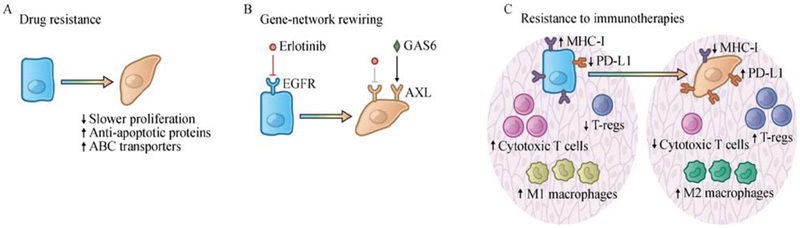
EMT confers therapeutic resistance. (A) EMT confers multidrug resistance on cancer cells. EMT-induced multidrug resistance involves a number of mechanisms, including a slow proliferation rate, elevated expression of anti-apoptotic proteins, and upregulation of ATP binding cassette (ABC) transporters that mediate drug efflux. (B) The E-to-M transition may induce cancer cells into novel phenotypic states and make certain therapeutic targets dispensable for continued cell viability. For example, the E-to-M transition switches the dependence of carcinoma cells from the EGFR to the AXL receptor tyrosine kinase in non-small-cell lung cancer cells, thereby yielding resistance to EGFR-targeted therapy. (C) The EMT program contributes to the establishment of an immunosuppressive tumor microenvironment and confers resistance to immunotherapies. In a cell-autonomous manner, induction of EMT program in carcinoma cells downregulates MHC-I molecules and β2-microglobulin while upregulating PD-L1. In addition, induction of EMT program leads to various non-cell-autonomous changes, remodeling the tumor microenvironment by recruiting M2 (pro-tumorigenic) macrophages and T-regs, and suppressing the infiltration of cytotoxic T cells.