
Figure 4:
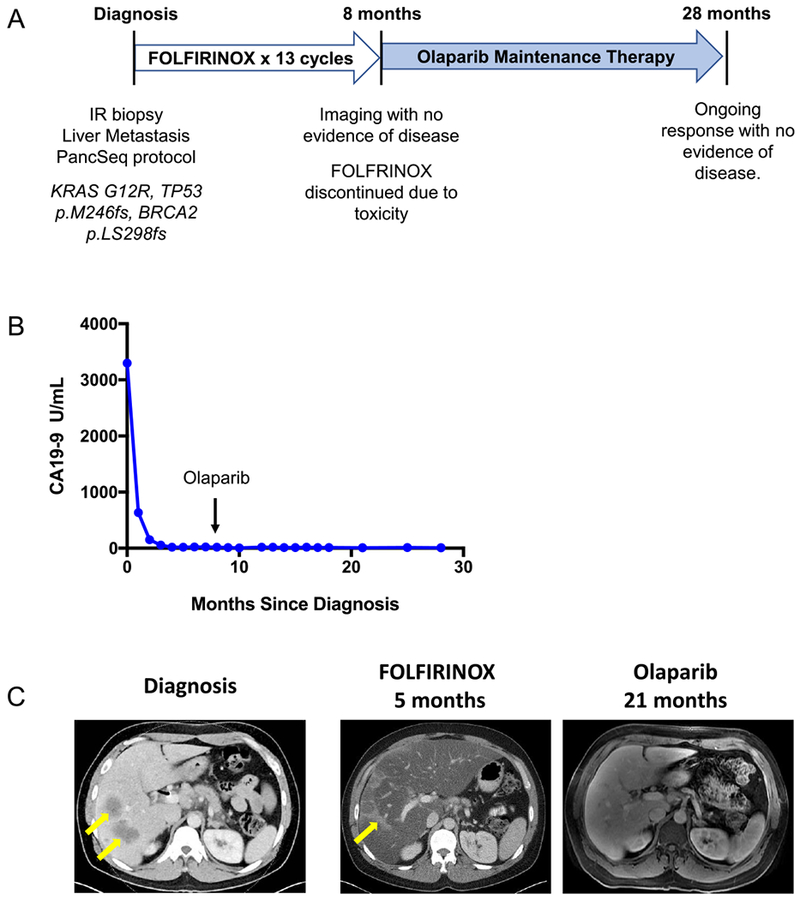
Patient with somatic BRCA2-mutant PDAC demonstrates a radiographic complete response to platinum chemotherapy and subsequent olaparib maintenance therapy. A) 45 year-old man presented with jaundice and abdominal pain and was diagnosed with metastatic PDAC involving the liver and lymph nodes and underwent the depicted treatment course. B) Serum CA19–9 measurements from diagnosis throughout the patient’s treatment course. The arrow indicates transition from FOLFIRINOX chemotherapy to Olaparib (PARP inhibitor) maintenance therapy. C) Computed Tomography (CT) scans are shown at diagnosis demonstrating liver metastases (left panel, yellow arrows) and at the time of cessation of FOLFIRINOX chemotherapy (middle panel) with resolution of liver metastases. Hepatic toxicity of FOLFIRINOX resulted in fatty infiltration of the liver, as noted by severe diffuse attenuation of the liver parenchyma seen in the five month scan. Areas of focal fat sparing in this scan represent treatment effect at the site of liver metastases (middle panel, yellow arrow), denoting a complete response to therapy. The follow-up magnetic resonance imaging (MRI) scan at 21 months after diagnosis, on olaparib maintenance therapy for 13 months, is shown with complete regression of liver metastases (right panel). The patient remains on olaparib therapy without evidence of disease now 28 months after diagnosis.