
Figure 2.
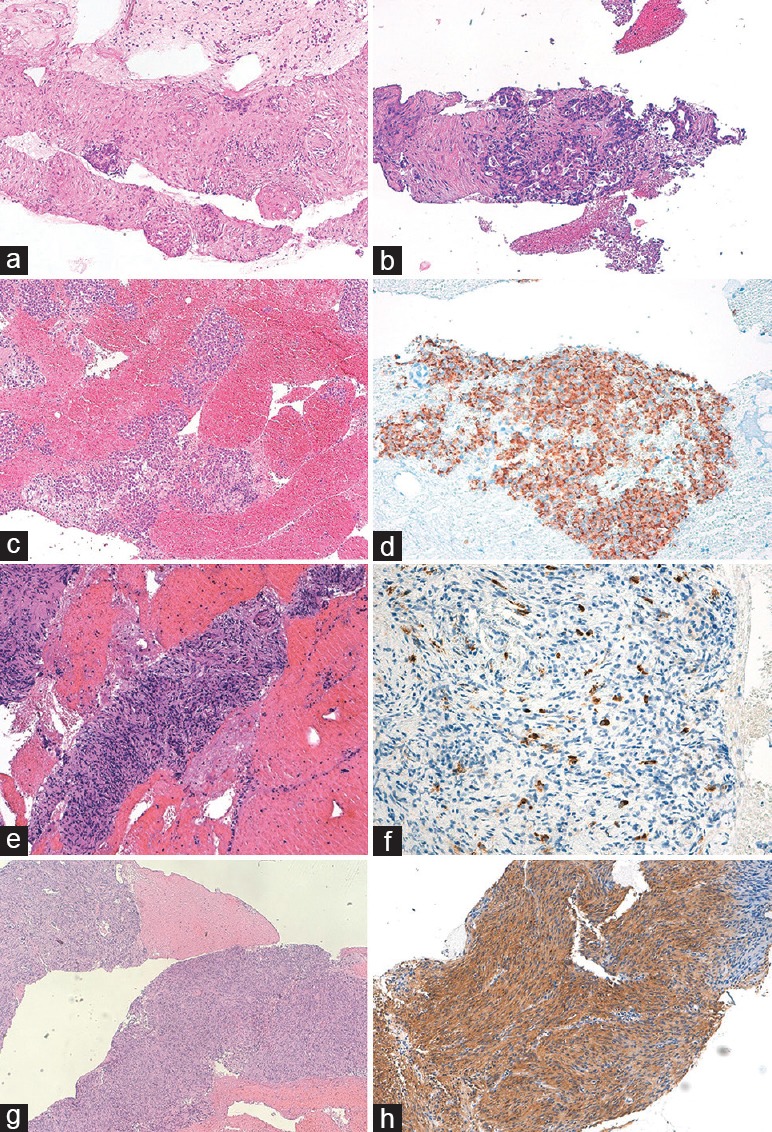
Histological samples from endoscopic ultrasound-guided fine-needle biospy of solid pancreatic lesions. (a) Abundant tissue fragments showing large areas of fibrosis with focal residual endocrine islets suggestive of chronic pancreatitis, (b) infiltration of ductal adenocarcinoma characterized by irregular glands with cribriform architecture, and marked nuclear pleomorphism, (c) groups of monomorphic epithelioid cells positive for chromogranin A at immuhistochemistry, (d) diagnostic for a well-differentiated neuroendocrine neoplasm, (e) abundant tissue fragments with large areas of fibrosis with residual ductal structures and chronic lymphocytic infiltrate, characterized by an elevated number of IgG4 + plasma cells at immunohistochemistry, (f) suggestive for autoimmune pancreatitis, (g) tissue fragments showing solid monomorphic spindle cells proliferation, positive at immunohistochemistry for CD117, and (h) diagnostic for gastrointestinal stromal tumor