
Figure 4.
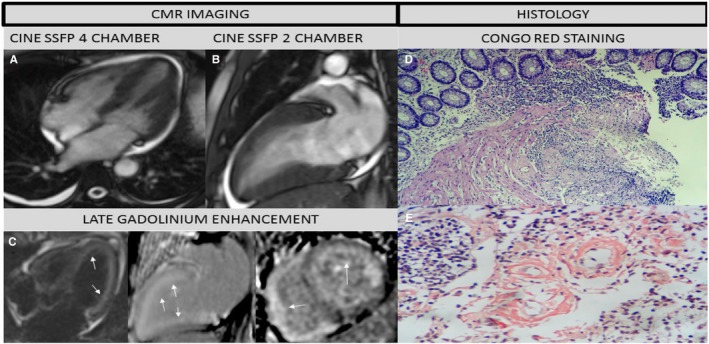
Fifty‐two‐year‐old personal trainer who complained of shortness of breath and fatigue. Previous echocardiogram showed hypertrophy. Cardiologist referral suspicious of Fabry's Disease. CMR study: (A) 4 chamber, (B) 2 chamber cine steady free precession revealed pleural and pericardial effusion, left ventricle hypertrophy and mild systolic dysfunction and (C) Contrast CMR (LGE: 4, 2, and short axis views) showed diffuse sub‐endocardial enhancement in both ventricles (white arrows), suggestive of Cardiac Amyloidosis (most likely type AL). Labial salivary gland biopsy revealed (D) Hematoxylin‐eosin stain, panoramic view: amyloid tissue infiltrating the muscularis mucosae and blood vessels, (E) Congo red stain, original magnification ×8: Type AL positive Congo red staining. Currently patient is receiving chemotherapy and continues follow‐up in heart failure clinic. Biopsy images shared by courtesy of Dr Jose Luis Arenas Gamio, Pathology Service, Guillermo Almenara Irigoyen Hospital, Lima—Peru. AL indicates amyloid light‐chain; CMR, cardiac magnetic resonance; LGE, late gadolinium enhancement.