
Figure 5.
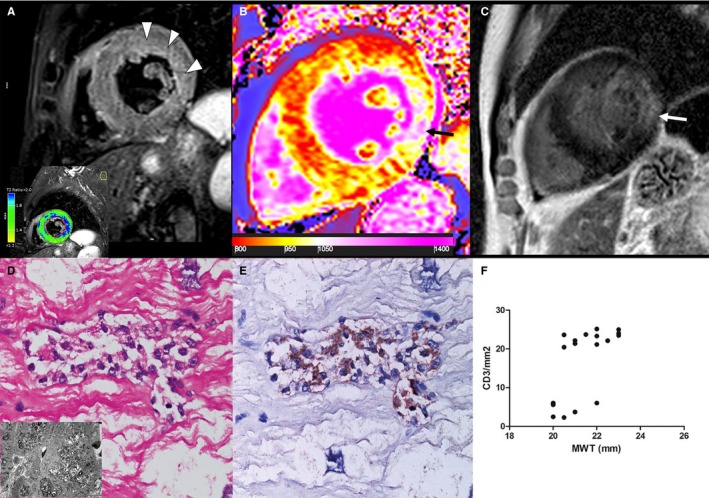
Group 4 patient. A 65‐year‐old man with Fabry disease cardiomyopathy (FDCM) and severe hypertrophy (maximal wall thickness [MWT]: 22 mm). A, T2‐weighted short τ inversion recovery shows a diffuse hyperintense signal of subendocardial midwall layers of lateral wall (arrowheads), as detected by the comparison with skeletal muscle signal (blue color, T2 ratio ≥2.0), reflecting myocardial edema. Native T1 map (B) and a late gadolinium–enhanced (LGE) image (C) demonstrate a severe decrease of myocardial T1 (septum: 867±42 ms), reflecting lipid accumulation and an LGE area at inferolateral wall (arrows), as a distinctive cardiac magnetic resonance hallmark of FDCM, corresponding to fibrous replacement (nT1: 1131±64 ms). D, Inflammatory infiltrate (hematoxylin and eosin, ×200), mainly of CD3+lymphocytes (E), was associated with necrosis of adjacent glycolipid‐laden myocytes. Insert in D shows vacuoles consisting of myelin bodies. F, Correlation between MWT and CD3 count (P<0.001, ρ=0.67) in all group 4 patients (n=18).