

Abstract
Diet restriction is one of the difficult parts of bowel preparation for colonoscopy, and many patients do not follow instructions properly. Few studies have evaluated the impact of dietary restriction in real clinical setting. The aim of this study was to study the effect of diet control on bowel preparation with detailed investigation of unacceptable food list in order to reveal what kind of foods are most problematic in clinical practice.
Prospective observational study was carried out at a university-affiliated hospital. Around 4 L polyethylene glycol solution was used for bowel preparation on the day of colonoscopy. Patients were allowed to have regular diet until lunch the day before colonoscopy and educated to control diet from 3 days before colonoscopy with information regarding an unacceptable foods list. Factors associated with inadequate bowel preparation were analyzed using univariate statistics and multivariate logistic regression analysis.
Of the 245 patients included in the study, 68 patients (27.8%) followed the diet instructions. Fiber-rich vegetables were the most commonly taken unacceptable foods (N = 143, 58.4%). Inadequate bowel preparation (fair and poor by Aronchick scale) was 47.3%. In multivariate analysis, diabetes [odds ratio (OR) 2.878, 95% confidence interval (CI) 1.242–6.671], preparation to colonoscopy interval (OR 1.003, 95% CI 1.000–1.005) and consumption of foods disturbing bowel preparation (OR 2.142, 95% CI 1.108–4.140) were independent predictors of inadequate bowel preparation.
We could identify substantially low compliance to diet instructions in real clinical practice. Consumption of any foods disturbing bowel preparation was significant factor predicting inadequate bowel preparation, even though we could not select specific food list compromising preparation significantly. Favorable bowel preparation was achieved in the subgroup compliant to diet restriction, suggesting that regular diet avoiding specific kinds of foods can be possible option for diet restriction before colonoscopy.
Keywords: bowel preparation, colonoscopy, polyethylene glycol, quality, regular diet
1. Introduction
Inadequate bowel preparation is known to prolong procedural time and decreases adenoma detection.[1] Despite of the various regime for bowel preparation, the rates of inadequate bowel preparation are reported to be between 20% and 30%.[2,3] Due to high rates of inadequate preparation, studies have been conducted to identify factors associated with inadequate bowel preparation, revealing several factors such as age, sex, diabetes, constipation, history of abdominal or gynecological surgery, compliance with preparation instructions, and time interval between bowel preparation and the start of colonoscopy.[4–9]
Diet is also important factor and we often encounter food materials such as grains and fruit seeds during colonoscopy in patients without any risk factors. Currently, several guidelines (AGA, ESGE) recommend low-residue or full liquids diet on the day before colonoscopy.[10,11] But few study focused on the effect of diet on the bowel preparation in real clinical setting,[12] even though there are several studies focusing on the comparison of low-residue diet (LRD) with clear liquid diet (CLD) under controlled circumstances.[11,13–15] In addition, in most studies of the risk factors of bowel preparation inadequacy, dietary factor is often omitted or usually considered as a component of adherence to the bowel preparation instructions making it difficult to assess exact impact of diet on the bowel preparation in clinical practice.[5,7,8,16] Also, the effect of regular diet until lunch on the day before colonoscopy on the bowel preparation is not well-known due to the lack of study.[17,18]
In this prospective observational study, we aimed to study impact of diet control (which is regular diet avoiding unacceptable foods) on the bowel preparation for colonoscopy with detailed investigation of unacceptable food list in order to reveal what kind of foods are most problematic in the real clinical practice, which can be used to optimize diet control in bowel preparation.
2. Methods
2.1. Subjects
We prospectively enrolled patients between 18 years and 85 years old who were scheduled for colonoscopy. This study was conducted at the gastrointestinal endoscopy unit of Korea University Anam Hospital in Seoul, Korea, between January 2013 and December 2013. Patients with following conditions were excluded: pregnancy, allergy to polyethylene glycol (PEG) and refusal to participate in this study. All patients provided written informed consent. This study was approved by the institutional review board.
2.2. Bowel preparation protocol
Patients were provided with standard bowel preparation instructions and educated by nurse to start diet restriction 3 days before colonoscopy with information of foods list to avoid (fiber-rich vegetables, seaweeds, whole grains, and seedy fruits). On the day before colonoscopy, patients were allowed to have regular diet for breakfast and lunch, a soft diet for diner and then only clear liquids until 2 hours before colonoscopy. All patients ingested 4 L of PEG solution (Colyte, Taejoon pharm Inc., Seoul, Korea) at least 6 hours before colonoscopy.
2.3. Data collection
Before the procedure, all patients were interviewed by research assistant using a predetermined questionnaire and data were collected regarding the start time of PEG dose and the completion time of the last PEG dose, the amount of preparation solution taken, adverse events during preparation as well as their compliance with instructions for bowel preparation. Detailed answers of diet within 3 days before colonoscopy were acquired about unacceptable foods list (vegetables, seaweeds, whole grains, and seedy fruits). We also collected the following variables: age, gender, body mass index (BMI), hospital status, performance status, indications for colonoscopy, medical conditions (such as diabetes, hypertension and liver disease), current medications, constipation, prior history of abdomen and pelvic surgery, stool form after PEG preparation, and bowel movement frequency after intake of PEG. Preparation-to-colonoscopy (PC) interval was calculated, which is interval from the time of last PEG completion to the start of colonoscopy. Cecal intubation time, total colonoscopy time, and colonoscopic findings including polyps were also recorded.
2.4. Evaluation of adequacy of bowel preparation
Bowel cleansing was evaluated according to the Aronchick Bowel Preparation Scale as described previously by the colonoscopist who was unaware of the patients’ dietary information.[19] Preparations rated with excellent or good were categorized as ‘adequate preparation’, whereas those with fair or poor were categorized as “inadequate preparation.” All study procedures were performed by 5 experienced colonoscopists between 9 AM and 5 PM.
2.5. Statistical analysis
For univariable analysis, χ2- test was performed for categorical variables and unpaired t-test for continuous variables. Multivariate logistic regression analysis were performed to assess factors that predict inadequate bowel preparation. A P-value of < .05 was considered statistically significant. SPSS software (SPSS 18.0 version for Windows, SPSS Inc, Chicago, IL) was used for statistical analysis.
3. Results
3.1. Patients’ characteristics and bowel preparation assessment
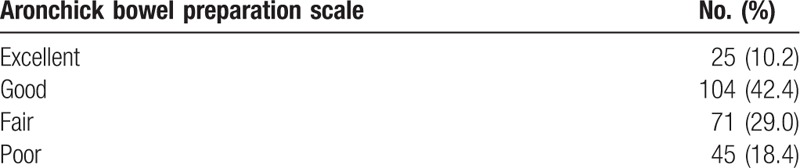
Totally, 306 patients who met the inclusion criteria were enrolled, 61 patients were excluded due to denial of participation or incomplete questionnaires and finally 245 patients were analyzed. The patient population consisted of 50.6% men and 49.4% women, with mean age 58.9 (range: 19–83) at the time of colonoscopy. Mean body mass index was 24.1 ± 3.6 kg/m2 (range: 15.62–37.39). 161 patients (65.7%) had comorbid disease, including hypertension (38.8%), diabetes (16.3%), liver disease (5.7%), thyroid disease (4.5%), psychiatric disease (2.0%), cardiovascular disease (4.5%), pulmonary disease (2.0%), and renal insufficiency (2.0%). 108 patients (44.1%) had previous abdominal or pelvic operation, which includes appendectomy (8.6%), colorectal resection (11.4%), gastrectomy (4.9%), hysterectomy (3.7%), and cholecystectomy (1.6%). The most common indication of colonoscopy was screening of malignancy (43.3%). Noncompliance to diet instructions was 72.2% totally, and for each unacceptable food category, fiber-rich vegetables are the most commonly taken unacceptable foods (Table 1). Regarding bowel preparation quality by Aronchick scale, “Excellent,” “Good,” “Fair,” and “Poor” were 10.2%, 42.4%, 29.0%, and 18.4%, respectively, of the study population (Table 2). No serious adverse event was occurred from the bowel preparation or colonoscopic procedure.
Table 1.
Baseline characteristics of study population.
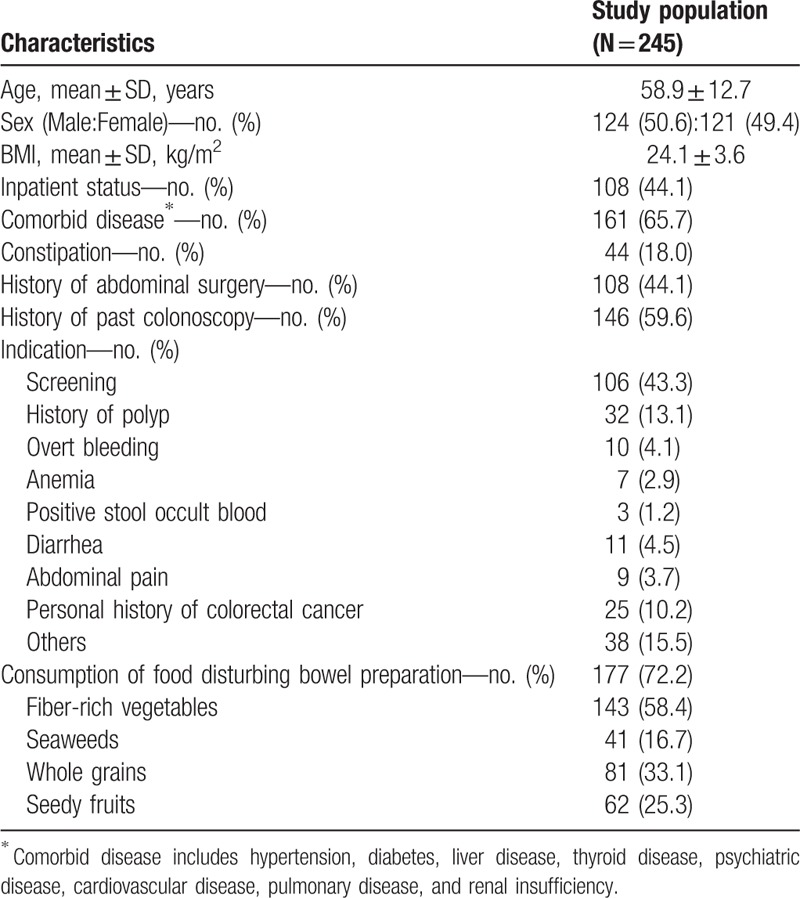
Table 2.
Aronchick bowel preparation scale of study population.
3.2. Factors associated with inadequate bowel preparation and impact of diet restrictions on bowel preparation
Factors affecting Aronchick bowel preparation scale were evaluated. We divided bowel preparation status into two groups: adequate bowel preparation (Excellent and Good) and inadequate bowel preparation (Fair and Poor). In univariate analysis, age, diabetes, PC interval, and consumption of foods disturbing bowel preparation were significantly associated with bowel preparation adequacy (Table 3). Among unacceptable food categories, only whole grains uptake was differed statistically significantly, and other food categories did not show significant difference between adequate and inadequate bowel preparation group (Table 3).
Table 3.
Univariate analysis of factors associated with inadequate bowel preparation.
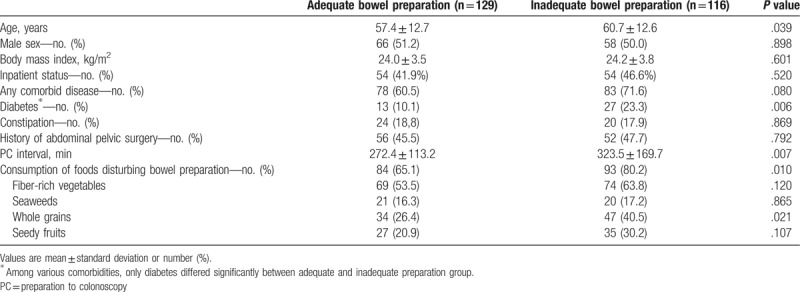
Figure 1 shows the distribution of bowel preparation scale according to the consumption status of unacceptable foods category. Figure 1A illustrates the increasing tendency of portion of inadequate bowel preparation when subjects consume any foods disturbing bowel preparation. Generally, consumption of each category of unacceptable food tends to disturb bowel preparation, but statistically, only consumption of whole grains showed significant difference in the distribution of Aronchick scale (Fig. 1B).
Figure 1.
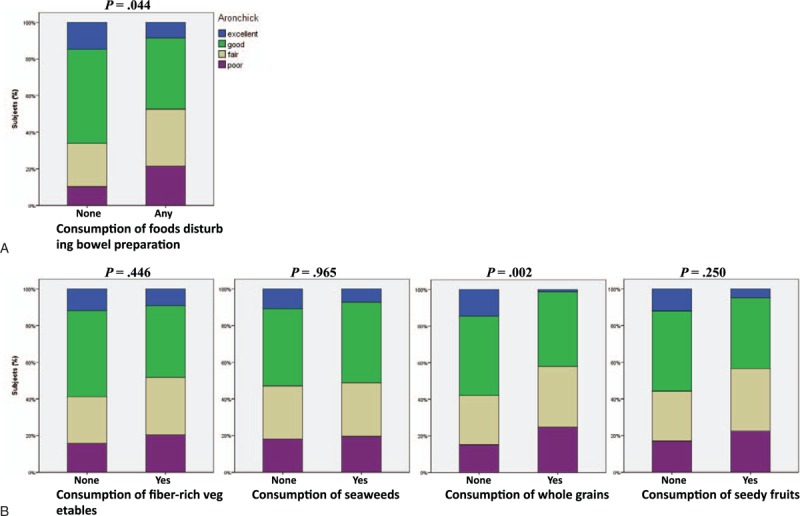
Bowel preparation status according to the consumption status of unacceptable food category. Distribution of Aronchick scale was different according to the consumption status of unacceptable foods (A), especially for consumption of whole grains (B). P-value for each graph is assessed by Fisher's exact test (2 × 4).
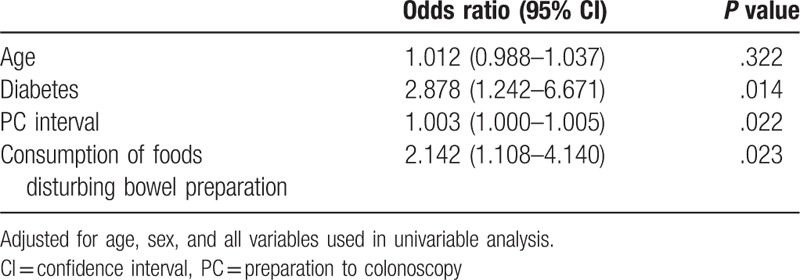
In multivariable analysis, consumption of food disturbing bowel preparation was significant risk factor for inadequate bowel preparation after controlling variables used in univariable analysis (age, sex, BMI, inpatient status, comorbidity, constipation, history of abdominopelvic surgery, PC interval) (Table 4). But each food category (i.e., fiber-rich vegetables, seaweeds, whole grains and seedy fruits) did not show statistical significance in multivariable analysis (data not shown).
Table 4.
Multivariable analysis of risk factors for inadequate bowel preparation.
3.3. Adverse events, tolerability and clinical outcomes according to the diet restriction
As secondary outcomes, we assessed the adverse events, bowel preparation tolerability and clinical outcomes according to the diet restriction status. Adverse events during bowel preparation were not different between the group compliant to diet instructions and noncompliant group (Table 5). The proportion of subjects who ingested more than 3L PEG solution was not different between two groups (Table 6). Cecal insertion was achieved in nearly all patients with success rate of 98% and this was not different between two groups. Cecal insertion time (minute) was longer in noncompliant group (9.08 ± 5.69 vs 11.23 ± 8.30). Polyp detection rate was about 40% and was not different between the 2 groups. Aronchick bowel preparation scale was different significantly between the 2 groups (Table 6 and Fig. 1A).
Table 5.
Adverse events.
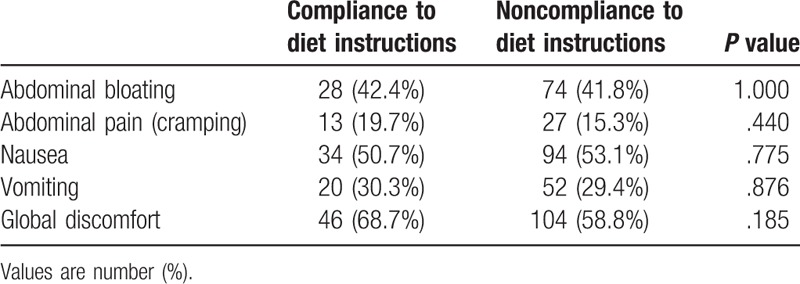
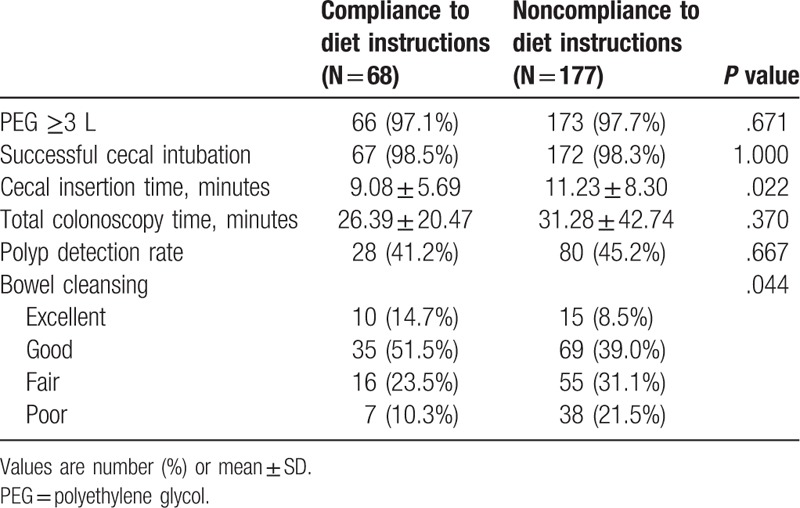
Table 6.
Clinical outcomes according to the diet restriction.
4. Discussion
Adequate bowel preparation is essential to find out significant lesions and perform safe procedures in colonoscopy. Several predictors of poor bowel preparation have been reported so far including age, sex, diabetes, constipation, history of abdominal surgery, and compliance with instructions.[4,5,7–9] Diet control is important component for adequate bowel preparation and current guidelines recommend low residue or full liquids diet on the day before colonoscopy.[10,11] Several studies have evaluated the efficacy of diet liberalization to LRD on the bowel preparation compared to CLD.[14,18,20,21] In these studies, diet liberalization did not adversely affect bowel preparations and improved patient willingness to repeat the bowel preparation and tolerability of preparation solutions. Still, data regarding the effect of regular diet (RD) on the bowel preparation is lacking and RD on the day before colonoscopy is not recommended yet.[10,17] In actual clinical practice, patients are very reluctant to follow diet restriction of LRD or CLD,[12] so RD avoiding some unacceptable food lists is often recommended instead of strict diet restriction in Korea.[17]
In this prospective observational study, we recommended RD until lunch of the day before colonoscopy, and figured out the effect of RD avoiding unacceptable foods on bowel preparation while controlling other factors associated with inadequate bowel preparation. Consumption of foods disturbing bowel preparation was significant factor affecting adequacy of bowel preparation in both univariable and multivariable analysis. Specifically, whole grains uptake was significantly associated with inadequate bowel preparation among forbidden food categories (fiber-rich vegetables, seaweeds, whole grains, and seedy fruits), even though statistical significance was disappeared in multivariable analysis. In literature review, data showing comparable outcome of LRD on the bowel preparation with CLD are easily available,[14,15,21,22] but studies evaluating the effect of RD are very limited.[17,18,23] Jung et al[17] showed similar rate of adequate bowel preparation between RD and CLD (83.3% vs 83.5%) in healthy outpatients, recommending RD avoiding fiber-rich foods as possible diet instructions prior to colonoscopy. Even though the consumption of unacceptable foods in RD group was not evaluated in this study, compliance of diet instruction seems to be high considering high rate of adequate bowel preparation.[17] Surprisingly, the compliance of diet restriction was very low (27.8%) in this study. This rate of compliance is significantly lower than reported compliance rate (70–80%) of previous studies which are performed under controlled circumstances (i.e., randomized controlled trials).[13,20] It was difficult to figure out the compliance rate of diet restriction in real clinical situation due to the lack of data, but two studies revealed similar low rate of compliance (27.8% and 44.2%) of the diet restriction.[12,24] This high rate of noncompliance in diet restriction may contribute to the high rate of inadequate bowel preparation rate in this study (47.4%, Table 2). The rate of inadequate bowel preparation is lowered to 33.8% when we analyzed subjects who followed the diet restriction (Table 6), which is similar to previous reports (20–30%).[2,25–27] High proportion of inpatient subjects (44.1%), high proportion of comorbidity, and nonsplit dosage regimen may also contribute to poor bowel preparation state.
In multivariable analysis, diabetes and PC interval were significant factors predicting inadequate bowel preparation in addition to the consumption of foods disturbing bowel preparation. These are consistent with previous findings of factors affecting bowel preparation,[4,7] but other factors such as BMI, inpatient status and constipation showed inconsistent result to previous studies.[9,12,28] These inconsistency can be due to the difference of study population and bowel preparation method but ethnic and cultural difference including food intake can be important another confounder. Even though various factors have been proposed as predictors of bowel preparations so far, there are still conflicting results, which need to be validated more.[7,8,29]
We also evaluated adverse events during ingestion of PEG solution and clinical outcomes of colonoscopy. There was no difference in adverse events between the group compliant to diet instructions and noncompliant group. High proportion of subjects (97%) could ingest PEG solution more than 3L in both groups, similar to previous reports which is about 90–95%.[17,30] Cecal insertion time was prolonged in noncompliant group, and this can be due to poorer bowel preparation in this group.[31] Polyp detection rate was not different between two groups. Several factors are known to be associated with adenoma detection rate (ADR) including quality of bowel preparation, but there is still controversy and some studies have shown no relationship between quality of bowel preparation and ADR.[32,33] In this study, we did not calculated ADR but we assume polyp detection rate will show similar results.[12]
This study has several limitations. First, this is prospective observational study. We could not randomly assigned subjects to diet restriction and nonrestriction group due to ethical problem, but due to its uncontrolled nature, we could represent real-life clinical situation of diet restriction. Second, food intake was assessed on the day of colonoscopy right before the procedure which is based on the patients’ memory, possibly leading to recall bias. Third, we collected data for unacceptable food categories but did not measure the amount of foods consumed. We could confirm the importance of avoiding unacceptable foods for adequate bowel preparation in this study, but could not select specific food categories affecting bowel preparation. Evaluating the combination of category and amount of foods consumed may give more specific results regarding the diet restrictions. Fourth, this study was performed in single center of tertiary care hospital. Large proportion of study subjects had one or more comorbidity and were inpatient state, making it difficult to generalize these findings to healthy subjects for screening colonoscopy performed in primary care hospital or out-patient department.[17]
This study focused on the effect of diet restriction on the bowel preparation state in real clinical practice. We could identify surprisingly low compliance to diet instructions, even though we have recommended RD. Consumption of foods disturbing bowel preparation was significant factor predicting inadequate bowel preparation and the only factor controllable in clinical setting except PC interval. We could not select any specific food category compromising bowel preparation significantly, but could achieve adequate bowel preparation comparable to previous studies in the group compliant to diet restriction even they consumed RD. In consideration of high impact but low compliance of diet restrictions, diet education should be emphasized more, and we need to develop effective way to improve diet restriction, for example, by using pre-packaged low residual meals or telephone-based re-education.[20,25,34] In addition, RD avoiding some unacceptable foods can be acceptable diet restriction before colonoscopy.
Author contributions
Conceptualization: Young Jin Kim, Bora Keum, Jae Min Lee, Hyuk Soon Choi, Hoon Jai Chun.
Data curation: Seung-Joo Nam, Young Jin Kim, Bora Keum, Jae Min Lee, Hyuk Soon Choi, Eun Sun Kim, Yeon Seok Seo, Yoon Tae Jeen, Hong Sik Lee, Hoon Jai Chun, Soon Ho Um, Chang Duck Kim.
Formal analysis: Seung-Joo Nam, Eun Sun Kim, Yoon Tae Jeen, Hong Sik Lee, Soon Ho Um, Chang Duck Kim.
Investigation: Seung-Joo Nam, Young Jin Kim, Bora Keum, Jae Min Lee, Seung Han Kim, Hyuk Soon Choi, Eun Sun Kim, Yeon Seok Seo, Yoon Tae Jeen, Hong Sik Lee, Hoon Jai Chun, Soon Ho Um, Chang Duck Kim.
Methodology: Seung-Joo Nam, Young Jin Kim, Jae Min Lee, Seung Han Kim, Hyuk Soon Choi, Eun Sun Kim, Yeon Seok Seo, Yoon Tae Jeen, Hoon Jai Chun, Soon Ho Um, Chang Duck Kim.
Supervision: Hoon Jai Chun.
Writing – original draft: Seung-Joo Nam, Young Jin Kim.
Writing – review & editing: Seung-Joo Nam, Bora Keum.
Seung-Joo Nam orcid: 0000-0002-0349-0901.
Footnotes
Abbreviations: ADR = adenoma detection rate, BMI = body mass index, CLD = clear liquid diet, LRD = low-residue diet, PC interval = preparation-to-colonoscopy interval, PEG = polyethylene glycol, RD = regular diet.
SJN and YJK contributed equally to this work.
The authors have no funding and no conflicts of interest to disclose.
References
- [1].Froehlich F, Wietlisbach V, Gonvers JJ, et al. Impact of colonic cleansing on quality and diagnostic yield of colonoscopy: the European Panel of Appropriateness of Gastrointestinal Endoscopy European multicenter study. Gastrointest Endosc 2005;61:378–84. [DOI] [PubMed] [Google Scholar]
- [2].Parente FR, Repici A, Crosta C, et al. Overall acceptability and efficacy of commonly used bowel preparations for colonoscopy in Italian clinical practice. A multicentre prospective study. Digest Liver Dis 2014;46:795–802. [DOI] [PubMed] [Google Scholar]
- [3].Soh JS, Kim KJ. Combination could be another tool for bowel preparation? World J Gastroenterol 2016;22:2915–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Hassan C, Fuccio L, Bruno M, et al. A Predictive Model Identifies Patients Most Likely to Have Inadequate Bowel Preparation for Colonoscopy. Clin Gastroenterol H 2012;10:501–6. [DOI] [PubMed] [Google Scholar]
- [5].Wong MC, Ching JY, Chan VC, et al. Determinants of bowel preparation quality and its association with adenoma detection: a prospective colonoscopy study. Medicine (Baltimore) 2016;95:e2251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Sim JS, Koo JS. Predictors of inadequate bowel preparation and salvage options on colonoscopy. Clin Endosc 2016;49:346–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Chung YW, Han DS, Park KH, et al. Patient factors predictive of inadequate bowel preparation using polyethylene glycol: a prospective study in Korea. J Clin Gastroenterol 2009;43:448–52. [DOI] [PubMed] [Google Scholar]
- [8].Ness RM, Manam R, Hoen H, et al. Predictors of inadequate bowel preparation for colonoscopy. Am J Gastroenterol 2001;96:1797–802. [DOI] [PubMed] [Google Scholar]
- [9].Borg BB, Gupta NK, Zuckerman GR, et al. Impact of obesity on bowel preparation for colonoscopy. Clin Gastroenterol Hepatol 2009;7:670–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Johnson DA, Barkun AN, Cohen LB, et al. Optimizing adequacy of bowel cleansing for colonoscopy: recommendations from the US multi-society task force on colorectal cancer. Gastroenterology 2014;147:903–24. [DOI] [PubMed] [Google Scholar]
- [11].Hassan C, Bretthauer M, Kaminski MF, et al. Bowel preparation for colonoscopy: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy 2013;45:142–50. [DOI] [PubMed] [Google Scholar]
- [12].Wu KL, Rayner CK, Chuah SK, et al. Impact of low-residue diet on bowel preparation for colonoscopy. Dis Colon Rectum 2011;54:107–12. [DOI] [PubMed] [Google Scholar]
- [13].Butt J, Bunn C, Paul E, et al. The White Diet is preferred, better tolerated, and non-inferior to a clear-fluid diet for bowel preparation: A randomized controlled trial. J Gastroenterol Hepatol 2016;31:355–63. [DOI] [PubMed] [Google Scholar]
- [14].Nguyen DL, Jamal MM, Nguyen ET, et al. Low-residue versus clear liquid diet before colonoscopy: a meta-analysis of randomized, controlled trials. Gastrointest Endosc 2016;83:499.e1–507.e1. [DOI] [PubMed] [Google Scholar]
- [15].Song GM, Tian X, Ma L, et al. Regime for bowel preparation in patients scheduled to colonoscopy: low-residue diet or clear liquid diet? Evidence from systematic review with power analysis. Medicine (Baltimore) 2016;95:e2432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Dik VK, Moons LM, Huyuk M, et al. Predicting inadequate bowel preparation for colonoscopy in participants receiving split-dose bowel preparation: development and validation of a prediction score. Gastrointest Endosc 2015;81:665–72. [DOI] [PubMed] [Google Scholar]
- [17].Jung YS, Seok HS, Park DI, et al. A clear liquid diet is not mandatory for polyethylene glycol-based bowel preparation for afternoon colonoscopy in healthy outpatients. Gut Liver 2013;7:681–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Avalos DJ, Sussman DA, Lara LF, et al. Effect of diet liberalization on bowel preparation. South Med J 2017;110:399–407. [DOI] [PubMed] [Google Scholar]
- [19].Aronchick CA, Lipshutz WH, Wright SH, et al. A novel tableted purgative for colonoscopic preparation: efficacy and safety comparisons with Colyte and Fleet Phospho-Soda. Gastrointest Endosc 2000;52:346–52. [DOI] [PubMed] [Google Scholar]
- [20].Park DI, Park SH, Lee SK, et al. Efficacy of prepackaged, low residual test meals with 4L polyethylene glycol versus a clear liquid diet with 4L polyethylene glycol bowel preparation: a randomized trial. J Gastroenterol Hepatol 2009;24:988–91. [DOI] [PubMed] [Google Scholar]
- [21].Walter J, Francis G, Matro R, et al. The impact of diet liberalization on bowel preparation for colonoscopy. Endosc Int Open 2017;5:E253–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Soweid AM, Kobeissy AA, Jamali FR, et al. A randomized single-blind trial of standard diet versus fiber-free diet with polyethylene glycol electrolyte solution for colonoscopy preparation. Endoscopy 2010;42:633–8. [DOI] [PubMed] [Google Scholar]
- [23].Scott SR, Raymond PL, Thompson WO, et al. Efficacy and tolerance of sodium phosphates oral solution after diet liberalization. Gastroenterol Nurs 2005;28:133–9. [DOI] [PubMed] [Google Scholar]
- [24].Dae Hyung W, Kyeong Ok K, Da Eun J, et al. Prospective analysis of factors associated with inadequate bowel preparation for colonoscopy in actual clinical practice. Intest Res 2018;16:293–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Liu X, Luo H, Zhang L, et al. Telephone-based re-education on the day before colonoscopy improves the quality of bowel preparation and the polyp detection rate: a prospective, colonoscopist-blinded, randomised, controlled study. Gut 2014;63:125–30. [DOI] [PubMed] [Google Scholar]
- [26].Kazarian ES, Carreira FS, Toribara NW, et al. Colonoscopy completion in a large safety net health care system. Clin Gastroenterol H 2008;6:438–42. [DOI] [PubMed] [Google Scholar]
- [27].Clark BT, Protiva P, Nagar A, et al. Quantification of adequate bowel preparation for screening or surveillance colonoscopy in men. Gastroenterology 2016;150:396–405. quiz e314-395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Yadlapati R, Johnston ER, Gregory DL, et al. Predictors of inadequate inpatient colonoscopy preparation and its association with hospital length of stay and costs. Dig Dis Sci 2015;60:3482–90. [DOI] [PubMed] [Google Scholar]
- [29].Lebwohl B, Wang TC, Neugut AI. Socioeconomic and other predictors of colonoscopy preparation quality. Dig Dis Sci 2010;55:2014–20. [DOI] [PubMed] [Google Scholar]
- [30].Stolpman DR, Solem CA, Eastlick D, et al. A randomized controlled trial comparing a low-residue diet versus clear liquids for colonoscopy preparation: impact on tolerance, procedure time, and adenoma detection rate. J Clin Gastroenterol 2014;48:851–5. [DOI] [PubMed] [Google Scholar]
- [31].Bernstein C, Thorn M, Monsees K, et al. A prospective study of factors that determine cecal intubation time at colonoscopy. Gastrointest Endosc 2005;61:72–5. [DOI] [PubMed] [Google Scholar]
- [32].Park JH, Kim SJ, Hyun JH, et al. Correlation between bowel preparation and the adenoma detection rate in screening colonoscopy. Ann Coloproctol 2017;33:93–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Jover R, Zapater P, Polania E, et al. Modifiable endoscopic factors that influence the adenoma detection rate in colorectal cancer screening colonoscopies. Gastrointest Endosc 2013;77:381.e1–9.e1. [DOI] [PubMed] [Google Scholar]
- [34].Delegge M, Kaplan R. Efficacy of bowel preparation with the use of a prepackaged, low fibre diet with a low sodium, magnesium citrate cathartic vs. a clear liquid diet with a standard sodium phosphate cathartic. Aliment Pharmacol Ther 2005;21:1491–5. [DOI] [PubMed] [Google Scholar]