

Abstract
Background
Malignant pleural mesothelioma (MPM) is a rare disease and management of localized disease is controversial. Radiotherapy has been shown to be useful after extrapleural pneumonectomy (EPP), as well as with less aggressive surgery. As no reports of the treatment of this disease have ever been published from Israel, we report our experience with MPM and intensity‐modulated radiotherapy (IMRT).
Methods
The complete medical records of patients treated for MPM at the Rabin Medical Center from 1 August 2007 to 31 March 2016 were reviewed. Twenty‐seven patients were treated with IMRT, either post‐EPP or without EPP. Patients received 54 Gy in 2 Gy fractions using the restricted field IMRT technique. Chemotherapy was administered sequentially in 26% of patients. Patients were followed up from the date of diagnosis to death or treatment failure.
Results
Seventy‐eight percent of patients had the epithelioid subtype. Nearly all patients were male (85%) and 90% of non‐surgical patients were administered chemotherapy compared to 56% of post‐EPP patients. All patients completed therapy and only 16% had grade 1–2 radiation pneumonitis, with no incidence of grade 3 or higher. The median follow‐up was 22 months and the mean overall survival was 34.9 months. The mean time to progression following radiation therapy was 26.7 months. The mean time to local and distant failure was 19 and 16 months, respectively.
Conclusions
IMRT for localized pleural mesothelioma is a tolerable and effective therapy both post‐EPP or without surgery. These results suggest that future investigation in this area is required.
Keywords: Mesothelioma, intensity‐modulated radiotherapy, extrapleural pneumonectomy
Introduction
Malignant pleural mesothelioma (MPM) is an uncommon thoracic malignancy, thus management remains a challenge. The appropriate therapy for locally advanced disease is controversial and has been widely debated. Trimodality treatment consisting of extrapleural pneumonectomy (EPP) combined with chemotherapy and radiotherapy (RT) has been widely reported with some long‐term survivors, but with morbidity and intensive selection bias.1
More recently, studies tend to recommend the use of lung sparing surgery, such as pleurectomy/decortication (P/D).2, 3 Some patients are ineligible for any surgical procedure and are primarily treated with systemic therapy alone, despite having local disease. The optimal therapy for these patients is unclear. In all of these settings – post EPP, intact lung, and operable – radiotherapy can play a role but lung tolerances must be carefully respected.4
In Israel, the outcome of therapy for mesothelioma has not been reported; therefore, we report our experience with intensity‐modulated radiotherapy (IMRT) for localized mesothelioma in both postoperative and inoperable settings. The aim of this study is two‐fold: to demonstrate that state of the art surgery and RT delivered in a small Middle Eastern country yields similar results to those published in the literature and to add to the growing data on the administration of IMRT in an intact lung in MPM patients.
Methods
The patient database at Davidoff Cancer Center, Rabin Medical Center was analyzed to locate MPM patients treated between 1 August 2007 and 31 March 2016. Twenty‐seven patients with complete medical records treated with RT were identified and reviewed with Helsinki committee approval (Table 1). The 27 patients were subsequently divided into two groups: post‐EPP (n = 16) and lung sparing treatment (n = 11). One patient in the lung‐sparing group was treated with PD.
Table 1.
Patient characteristics
| Patient characteristics | Patient population | |||||
|---|---|---|---|---|---|---|
| All | Surgical | Non‐surgical | ||||
| No. | % | No. | % | No. | % | |
| Age, years | ||||||
| Median (range) | 70 (51–85) | 67 (51–79) | 73 (55–85) | |||
| Gender | ||||||
| Male | 23 | 88% | 13 | 87% | 10 | 91% |
| Female | 3 | 12% | 2 | 13% | 1 | 9% |
| Ethnicity | ||||||
| Israel | 10 | 38% | 9 | 60% | 1 | 9% |
| Other | 16 | 62% | 6 | 40% | 10 | 91% |
| Asbestos exposure | ||||||
| Yes | 9 | 35% | 5 | 33% | 4 | 36% |
| No | 17 | 65% | 10 | 67% | 7 | 64% |
| ECOG at baseline | ||||||
| 0 | ||||||
| 1 | 7 | 4 | 3 | |||
| 2 | ||||||
| 3 | ||||||
| Location | ||||||
| Right | 16 | 62% | 8 | 53% | 8 | 73% |
| Left | 10 | 38% | 7 | 47% | 3 | 27% |
| Histology† | ||||||
| Epithelioid | 21 | 88% | 14 | 93% | 7 | 78% |
| Sarcomatoid | 1 | 4% | 0 | ‐ | 1 | 11% |
| Biphasic | 2 | 8% | 1 | 7% | 1 | 11% |
| Chemotherapy | ||||||
| Yes | 20 | 77% | 10 | 67% | 10 | 91% |
| No | 6 | 23% | 5 | 33% | 1 | 9% |
| Median (range) total IMRT dose, Gy | N/A | 50 (20 ‐ 56) | ||||
The histology in two patients was unknown.
ECOG, Eastern Cooperative Oncology Group; IMRT, intensity‐modulated radiotherapy.
The predominant histology in both groups was epithelioid (21/27), with one sarcomatoid and two biphasic. The histological subtype in two patients was not otherwise specified.
The patients in the post‐EPP group were subsequently treated with IMRT to 54 Gy to the entire hemithorax. Patients who were non‐surgically managed received pleural IMRT (P‐IMRT) to 54 Gy to the entire hemithorax.
Target volumes
Post‐extrapleural pneumonectomy (EPP)
The clinical target volume (CTV) was defined as the entire pleural surface from the insertion into the diaphragm to the surface of the lung. The volume was outlined as described in Allen et al.4
No EPP
When the lung was intact the entire pleural lung surface was treated, based on anatomical boundaries. Fissures were often avoided to conserve the normal lung, except when gross disease was present. In addition, compromises on normal tissue constraints occasionally caused a 5–10% compromise in the lung CTV in intact lungs.
For both intact lungs and post‐EPP, four‐dimensional computed tomography (CT) was used to define the motion of the CTV and expanded accordingly. Although it is clear that an additional planning target volume (PTV) should be added when the setup is uncertain, we chose not to further expand the PTV because of concerns over toxicity.
Representative samples of contouring are shown in Figure 1.
Figure 1.
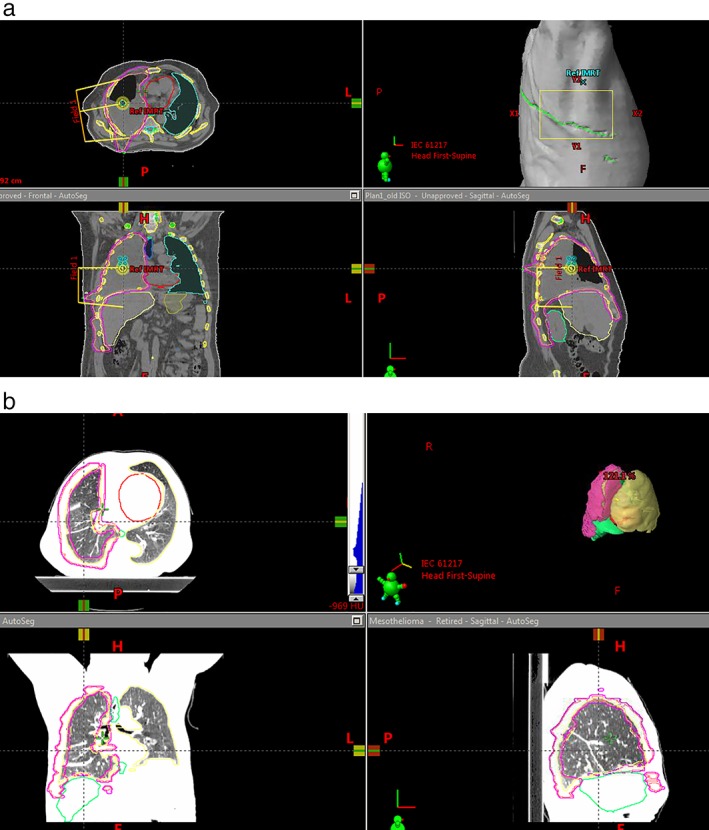
Showing contours: (a) post‐extrapleural pneumonectomy and (b) intact lung.
Intensity‐modulated radiotherapy (IMRT)/planning technique
For both post‐EPP and non‐surgical cases a 7–9 field arrangement is used with the restricted field technique, as previously described.5 Dose constraints are outlined in Tables 2 and 3.
Table 2.
IMRT dose constraints
| Structure & constraint | Value |
|---|---|
| Ipsilateral lung | |
| V20Gy, % | ≤ 10 |
| V5Gy, % | ≤ 60 |
| MD (Gy) | ≤ 9 |
| Contralateral lung | |
| V20Gy, % | ≤ 35 |
| V5Gy, % | ≤ 60 |
| MD (Gy) | ≤ 17 |
| Heart | |
| V30Gy, % | ≤ 50 |
| Esophagus | |
| MD (Gy) | ≤ 40 |
| V55Gy, % | ≤ 30 |
IMRT, intensity‐modulated radiotherapy; MD, mean dose.
Table 3.
Dosimetric data
| Post‐EPP | Intact lungs | |
|---|---|---|
| MLD (median, range) | 4.6 Gy (2–7.3) | 15.6 Gy (21.5–13.6) |
| V20 | 0.9% (0–9.5) | 31% (18.6–47) |
| V5 | 32.2% (1.69–60) | 63.2% (27–83) |
EPP, extrapleural pneumonectomy; MLD, mean lung dose.
IMRT quality assurance
In our department, each IMRT plan undergoes quality assurance (QA) before delivery to the patient. The majority of the specific patient QA is performed using ArcCheck (Sun Nuclear Corporation, Melbourne, FL, USA) and/or electronic portal dosimetry. For plans with large beam fields above 21 cm, ArcCheck is preferred. In order to check large fields we irradiate half of the field each time on a different side of the ArcCheck and then combine the dose maps with SNC patient software to a single dose file. The tolerance is set for a Gamma 3 mm/3% > 90.
Systemic therapy
Cisplatinum‐pemetrexed chemotherapy was administered to 18 of the 27 patients. Of the post‐EPP patients, 9 out of 16 (56%) were administered sequential chemotherapy and IMRT. In the non‐surgically managed group, 10 out of 11 (90%) patients were administered sequential chemotherapy and IMRT. A multidisciplinary tumor board reviewed all patients prior to therapy. In addition, the patients were followed up for overall survival (OS) and toxicity until death.
Statistical analysis
The statistical analysis for this paper was generated using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Continuous variables are presented as mean ± standard deviation. Categorical variables are presented as number or percentage. The Kaplan–Meier model with the log‐rank test was used to assess OS. Time to failure, with death without failure as a competing risk, was assessed using the Cox proportional hazards model with Fine and Gray methodology. Two‐sided P values < 0.05 were considered statistically significant. Toxicity was graded according to Common Terminology Criteria for Adverse Events version 4.0.
Results
Of the 27 patients analyzed, 60% had right side tumors. The histologic types were: epithelial in 88%, sarcomatoid in 4%, and mixed in 8%. Twenty percent of the patients had stage I, 15% had stage II, 55% had stage III, and 5% had stage IV disease. Nine (33%) of the 27 patients had been exposed to asbestos.
Sixteen patients (57%) were administered chemotherapy prior to radiation treatment (mainly cisplatin and pemetrexed), of which only two received preoperative chemotherapy, 58% underwent EPP before IMRT, and 42% did not undergo resection.
Toxicity
All patients were able to complete the complete prescribed dose of RT without treatment breaks. The median dose of RT was 54 Gy. Acute toxicity included grade 1 weight loss (23%), grade 1 fatigue (30%), and grade 1–2 radiation pneumonitis (16%). Importantly, none of the patients demonstrated signs of grade 3 or higher radiation pneumonitis.
Outcome
Eight (30%) of the 27 patients developed local progression in the thorax: 3 patients (19%) in the post‐EPP cohort and 5 in the non‐EPP cohort (45%). Distant failure was observed in 13 (48%) patients. Similar percentages of patients in the EPP group (48%) failed distantly compared to the non‐EPP group (45%), as was expected.
The median follow‐up period of our patient sample was 22 months. The mean OS was 34.9 months and the mean time to progression following RT was 26.7 months. The mean time to local and distant failure was 19 and 16 months, respectively.
In univariate analysis only the location of the tumor was found to have a significant impact on OS (hazard ratio 0.211, confidence interval 0.063–0.705; P = 0.011), favoring left side disease. Biphasic histology was found to have an almost seven‐fold likelihood of progression following RT (hazard ratio 6.930, confidence interval 1.34–35.72; P = 0.02). All other tested variables were non‐significant.
Dosimetric details
Intensity‐modulated RT planning was highly successful in most cases for achieving the planning constraints. The complete lung dose‐volume histogram parameters can be seen in Table 2.
Discussion
Trimodality therapy was first introduced in 1982. A combination of surgery, chemotherapy, and radiation were used to treat MPM. Since that time, advances in therapeutics and radiation and surgical techniques have increased survival in these patients.6 Recent studies have indicated that the use of IMRT following EPP provides increased local control. In addition, the majority of patients experienced disease recurrence at a distant location, while only 5% failed locally.7, 8 Therefore, we would expect to have increased local control when using IMRT in a trimodality protocol. Furthermore, with the increased ability to control the placement of radiation, we expect the toxicity to decrease. Krug et al. showed that if all three modalities were completed,9 median survival of 29.1 months and two‐year survival of 61.2% were achievable. This has been shown to be the case in a number of articles discussing the use of EPP combined with IMRT. In a study conducted at the MD Anderson Cancer Center, 63 consecutive patients received both EPP and IMRT (median dose 45 Gy) and were found to have a 13% failure rate within the radiation field.8 Miles et al. reported a local failure rate of 46% (median dose 45 Gy),10 while Gupta et al. reported a local failure rate of 40%.9 Rice et al. reported median survival of 14 months,7 while Patel et al. reported median survival of 23.2 months.11
Our data presents similar findings as previous studies in terms of median survival, at 22 months. Our patients had better local control with a 19% failure rate (3/16 patients). In addition, there were no fatalities and toxicity was limited to grade 2 pneumonitis. This has not been the case in other studies where toxicity and local control remained at suboptimal levels.4, 9, 11 Our study is important as it demonstrates the ability to translate these results to a smaller center with a Middle Eastern patient population and is the first report of MPM from the State of Israel.
EPP versus pleurectomy/decortication
In recent years, studies have demonstrated the inefficiency of EPP compared to P/D. A meta‐analysis demonstrated that EPP was associated with severe morbidity and increased 30‐day mortality.12 Flores et al. showed a significant benefit of P/D compared to EPP (P < 0.001). In multivariate analysis, EPP has been shown to be significantly inferior to P/D.2 In their meta‐analysis, Taioli et al. concluded that P/D should be performed whenever possible.3
With this data in mind, many institutions have begun performing P/D, thus leading to the increased need for a radiation technique to take an intact lung into account. We have not made the switch to P/D in our institution, although it should be strongly considered based on the data available.
Non‐operable IMRT with chemotherapy
The Memorial Sloan Kettering Cancer Center reported the first published data of outcomes in patients treated with definitive IMRT with chemotherapy rather than surgery. The data of 16 patients who did not undergo surgery was analyzed. They were treated with non‐concurrent chemotherapy and an average of 46.8 Gy using IMRT. OS at one and two years was 69% and 28%, respectively, with median survival of 17 months. At one year, the local and distant failure rates were 63% and 29%, respectively. The median interval from completion of IMRT to local recurrence was four months. There were four cases of grade 3 or higher pneumonitis (three grade 3, one grade 4), but no fatalities.13
Based on these encouraging results, a phase II study was conducted to analyze the use of IMRT within multimodality treatment. Patients were treated with IMRT to 50.4 Gy with at least four cycles of pemetrexed + platinum. The one and two year survival rates in the non‐operative group were 74% and 25%, respectively. In the entire cohort, only two patients developed grade 3 pneumonitis and they both recovered.14
Our results also indicate that non‐operable patients had comparable responses to chemotherapy and IMRT. Our results showed a median time to progression of 12 months and median OS of 13.5 months (range: 8–49). It should also be noted that no patients experienced grade 3 or higher pneumonitis.
Although our results are not as strong as the data published from Memorial Sloan Kettering, which could be explained by the lack of cytoreductive surgery (P/D), they are encouraging. Our findings demonstrate an improvement in progression‐free survival and encouraging median OS when compared to single modality treatment with chemotherapy.15 This is particularly important for patients who present with low volume pleural disease, as chemotherapy can be delayed until required. Further analysis with larger groups and prospective studies are required.
When the elderly or non‐curable population is involved in treatment, a medical ethics debate often ensues as to whether the investment of resources is efficacious. To justify the use of aggressive therapy, chemotherapy, and radiation in these patients, the use of prognostic markers may be beneficial. De Rienzo et al. discuss the use of a gene expression test to determine the prognosis of patients with mesothelioma using samples taken prior to surgery.16 When comparing their data to an independent cohort, they found that the gene expression score was a significant predictor of survival in both univariate and multivariate analysis. Therefore, by using the gene expression score we can predict which patients will have better outcomes and can tailor treatment accordingly.
Lung constraints
Allen et al. demonstrated the importance of using appropriate lung constraints during treatment with IMRT.4 Mean lung dose, V20, and V5 (volume of lung that received ≥ 5 Gy) constraints of 17 Gy, 35%, and 60%, respectively, were all met. Specifically, the median V5 was 32% and V20 was 0.4%. Although our constraints were more liberal than those used by Allen et al. we report better outcomes as a result of our ability to stay well below these constraints.
Limitations
As with all retrospective studies, further prospective analysis is warranted to analyze our conclusions. In addition, the small series and use of EPP as opposed to P/D further limited the study.
In the first national report of MPM patients treated with RT, we found the modern IMRT technique to be feasible and effective. The low levels of toxicity and encouraging local control and survival rates suggest RT for localized MPM is an important treatment option for patients.
Disclosure
No authors report any conflict of interest.
References
- 1. Sugarbaker DJ, Garcia JP, Richards WG et al Extrapleural pneumonectomy in the multimodality therapy of malignant pleural mesothelioma. Results in 120 consecutive patients. Ann Surg 1996; 224: 288–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Flores RM, Pass HI, Seshan VE et al Extrapleural pneumonectomy versus pleurectomy/decortication in the surgical management of malignant pleural mesothelioma: Results in 663 patients. J Thorac Cardiovasc Surg 2008; 135: 620–6. [DOI] [PubMed] [Google Scholar]
- 3. Taioli E, Wolf AS, Flores RM. Meta‐analysis of survival after pleurectomy decortication versus extrapleural pneumonectomy in mesothelioma. Ann Thorac Surg 2015; 99: 472–80. [DOI] [PubMed] [Google Scholar]
- 4. Allen AM, Czerminska M, Jänne PA et al Fatal pneumonitis associated with intensity‐modulated radiation therapy for mesothelioma. Int J Radiat Oncol Biol Phys 2006; 65: 640–5. [DOI] [PubMed] [Google Scholar]
- 5. Allen AM, Schofield D, Hacker F, Court LE, Czerminska M. Restricted field IMRT dramatically enhances IMRT planning for mesothelioma. Int J Radiat Oncol Biol Phys 2007; 69: 1587–92. [DOI] [PubMed] [Google Scholar]
- 6. PM MC, Nagasaki F, Hilaris BS, Martini N. Surgical treatment of pleural mesothelioma. J Thorac Cardiovasc Surg 1982; 84: 834–42. [PubMed] [Google Scholar]
- 7. Ahamad A, Stevens CW, Smythe WR et al Promising early local control of malignant pleural mesothelioma following postoperative intensity modulated radiotherapy (IMRT) to the chest. Cancer J 2003; 9: 476–84. [DOI] [PubMed] [Google Scholar]
- 8. Rice DC, Stevens CW, Correa AM et al Outcomes after extrapleural pneumonectomy and intensity‐modulated radiation therapy for malignant pleural mesothelioma. Ann Thorac Surg 2007; 84: 1685–92. [DOI] [PubMed] [Google Scholar]
- 9. Gupta V, Krug LM, Laser B et al Patterns of local and nodal failure in malignant pleural mesothelioma after extrapleural pneumonectomy and photon‐electron radiotherapy. J Thorac Oncol 2009; 4: 746–50. [DOI] [PubMed] [Google Scholar]
- 10. Miles EF, Larrier NA, Kelsey CR et al Intensity‐modulated radiotherapy for resected mesothelioma: The Duke experience. Int J Radiat Oncol Biol Phys 2008; 71: 1143–50. [DOI] [PubMed] [Google Scholar]
- 11. Patel PR, Yoo S, Broadwater G et al Effect of increasing experience on dosimetric and clinical outcomes in the management of malignant pleural mesothelioma with intensity‐modulated radiation therapy. Int J Radiat Oncol Biol Phys 2012; 83: 362–8. [DOI] [PubMed] [Google Scholar]
- 12. Papaspyros S, Papaspyros S. Surgical management of malignant pleural mesothelioma: Impact of surgery on survival and quality of life‐relation to chemotherapy, radiotherapy, and alternative therapies. ISRN Surg 2014; 2014: 817203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. KEm R, Zauderer MG, Laser B et al Pleural intensity‐modulated radiotherapy for malignant pleural mesothelioma. Int J Radiat Oncol Biol Phys 2012; 83: 1278–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Rimner A, Zauderer MG, Gomez DR et al Phase II study of hemithoracic intensity‐modulated pleural radiation therapy (IMPRINT) as part of lung‐sparing multimodality therapy in patients with malignant pleural mesothelioma. J Clin Oncol 2016; 34: 2761–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Vogelzang NJ, Rusthoven JJ, Symanowski J et al Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J Clin Oncol 2003; 21: 2636–44. [DOI] [PubMed] [Google Scholar]
- 16. De Rienzo A, Cook RW, Wilkinson J et al Validation of a gene expression test for mesothelioma prognosis in formalin‐fixed paraffin‐embedded tissues. J Mol Diagn 2017; 19: 65–71. [DOI] [PMC free article] [PubMed] [Google Scholar]