

Abstract
Abstract
Cartilage-perichondrium composite graft is used in middle ear surgery for tympanic membrane, ossicular and for soft wall reconstruction. The thickness of the cartilage is thought to interfere with the sound conduction. In our otology practice for tympanic membrane reconstruction, we prefer the sliced cartilage graft to achieve acoustic benefit. At times in the process of slicing, the cartilage gets wasted if not sliced with a precision slicing instrument. We have designed and developed a multi-purpose cartilage slicer for precise reduction of the thickness of the cartilage. To describe the design of our cartilage slicer and to report our preliminary experience with the cartilage slicer. Descriptive study. The technique of slicing with our new cartilage slicer and its usage has been described in detail. A total number of 689 cartilages in tympanoplasty and mastoidectomy have been sliced with it from 2013 to 2017. Our study reports the technique of slicing the tragal cartilage for tympanoplasty, highlighting its advantages and precision of the cartilages slices obtained. Our cartilage slicer is a good option for cartilage slicing in tympanoplasty.
Level of Evidence
Level 4.
Keywords: Tragal cartilage; Slicing; Cartilage slicer, Slice !t, cartilage tympanoplasty
Introduction
Since the introduction of tympanoplasty, many grafts have been used for the reconstruction of the tympanic membrane (TM). The most common ones are temporalis fascia and perichondrium. The success of temporalis fascia tympanoplasty varies from 70 to 90 percent in different hands [1]. In revision tympanoplasty, the results with fascia have not been gratifying. In such cases, a stronger and rigid graft material is needed to sustain the conditions of Eustachian tube dysfunction. Cartilage as a TM graft resists negative middle ear pressure to a much greater degree than fascia due to its inherent rigidity, thus preventing retractions and re-perforations [2]. It has been well demonstrated in both experimental as well as clinical studies that cartilage is well accepted by the middle ear as a graft, and has long-term survival [3, 4]. The sound conduction properties of cartilage replicate that of normal tympanic membrane and its tendency to resist retraction and conduction depend on the thickness and technique used [5, 6]. Cartilage also offers resistance to re-perforation in infection, atrophic tympanic membranes and in revision surgery [7]. Several techniques for cartilage tympanoplasty have been used, such as composite auto graft shield, cartilage palisade tympanoplasty, perichondrium island flap, cartilage butterfly inlay graft, Crowncork technique, cartilage mosaic tympanoplasty and cartilage reinforcement [1, 8, 9]. However, concerns are raised related to its sound conduction properties due to the obvious thickness. Using the Doppler interferometer, Zahnart et al. [10] suggested that acoustic benefit could be obtained by thinning the cartilage to 0.5 mm, but this advantage is offset by the unacceptable curling of the graft that occurs when the cartilage is thinned and perichondrium is left attached to one side [ 10, 11]. The thickness of the normal tympanic membrane is 0.1 mm. From 2002 to 2012 [12–17], the authors have been using the sliced tragal cartilage for TM and middle ear reconstruction. In 2013, we modified the previous existing cartilage slicers and developed a new cartilage slicer having multipurpose functions for cartilage tympanoplasty techniques [18–20]. Our cartilage slicer has been named under the registered trade mark of Slice !t. The aim of this study is to describe our newly developed cartilage slicer along with the technique of slicing and reporting our prelimnary experience with the cartilage slicer in middle ear surgery.
Materials and Methods
We have developed a new cartilage slicer, Slice !t (Figs. 1, 2, 3) in 2013. It has been applied for IPR to government of India under the Design Act. After designing the slicer, the precision of the slices produced was evaluated in cadaveric human tragal cartilages. After obtaining the satisfactory slices, the cartilage slicer was used for middle ear surgeries. This study consists of 689 tragal cartilages of patients operated in MIMER Medical College and in Sushrut ENT Hospital from October 2013 to December 2017. We have sliced 689 cartilages using slice !t till now. There were 366 males and 323 females. The patients ranged from 8 to 65 years with mean age of 39.34 years. Written consent was taken in all the patients. The details of the operative procedure was explained to the patients and to their parents (in case of paediatric patients). The Institutional review Ethics Committee has approved the study.
Fig. 1.
The Cartilage Slicer, Slice !t set
Fig. 2.

The parts of Slice !t
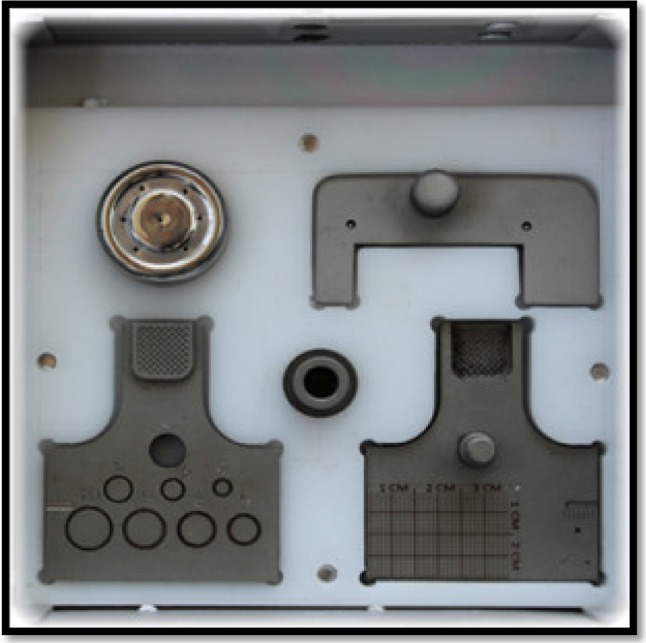
Fig. 3.

The Cartilage Holding Unit of Slice !t (both side View). a Opposing view with the measurement grid. b View of the predefined circles for cartilage island preparation. c Slots for prosthesis measurements
Description of the New Cartilage Slicer, Slice !T (Figs. 1, 2, 3)
The parts of the slice !t:
Modified Cartilage Holding Unit (2 pieces and Screw)
Cartilage Knife holding unit (2 Pieces And Screw)
Spacers (4 in number of 0.1. 0.2, 0.3 & 0.5 mm)
Cartilage Punch Rods (2 numbers of 0.8 mm & 1 mm)
A. The cartilage holding unit (Figs. 1, 2, 3): It consists of two parts. Both the parts of the cartilage holding unit are aligned with each other and tightened with a screw. It has gliding slits through which the razor blade passes. The additional features and functions (Fig. 3a–c) include:
Measurement grid for measuring the size of the grafts harvested (cartilage, fascia, perichondrium)
Wedge like vertical slot for measuring and trimming prosthesis to desired lengths.
Measurement guide for trimming the Teflon piston to the desired size.
Circumscribed well slots from 4 to 10 mm for fashioning of cartilage perichondrium islands in case of sliced perichondrium island.
B. The cartilage knife unit (Figs. 1, 2): It has 2 pieces with a screw for fastening and tightening a razor blade. The cartilage knife unit passes through the cartilage holding unit for precise cartilage slicing.
C. Metallic Spacers: The cartilage slicer is provided with 4 metallic spacers of thickness of 0.1 mm, 0.2 mm, 0.3 mm and 0.5 mm for precise slicing of the cartilage to obtain slices of respective thickness (Fig. 2). The metallic spacers provided are of the same shape and area as the recess of the lower part of the cartilage holding unit. The cartilage to be sliced is placed over the metallic spacer of desired thickness within the slot. With the sawing movements of the blade, the cartilage is sliced.
D. It is provided with 2 vertical cylindrical rods of length 3 cm and breadth 0.8 and 1 mm. These are used for punching into the cartilage for making slot. These slotted cartilage can be accommodated over the head of the stapes for ossiculoplasty.
All these units are meticulously placed in slotted compartments of the autoclavable stainless steel box (Fig. 1).
Technique of Slicing the Tragal Cartilage with Slice !t
After harvesting cartilage, it is placed into the cartilage-holding unit with the desired metallic thickness plate to get that particular slice of the cartilage. The thickness of the tragal cartilage is approximately 1 mm. The slot provided in the cartilage holding unit after it is aligned together is 1 mm. By placing the cartilage into the cartilage holding unit with a spacer of thickness (x), it gets raised by the same amount as the thickness of the spacers (x). When the knife is passed through it, it gives 2 slices (x) and (1 mm-x). When the cartilage is thicker than 1 mm then we do not use the spacer. Simply slicing without spacer gives 2 slices one of 1 mm and the other will be excess of 1 mm.
The peculiarity of the Cartilage Splitter is that it can produce precise cartilage slices of varied thickness ranging from 0.1 to 0.5 mm. For Type-I tympanoplasty, we use 0.5 mm (or less) spacer and slice the cartilage again to get the desired graft. For multiple pieces of sliced cartilage, one can use different spacers and/or combinations of spacers.
Results
We have been slicing the tragal cartilage with Slice !t (Figs. 4, 5b) for middle ear surgery since 2013. Our study consists of 689 tragal cartilages of patients operated in MIMER Medical College and in Sushrut ENT Hospital from October 2013 to December 2017. Of 689 ears, 409 cartilages were used in tympanoplasty and 280 cartilages in mastoidectomy (Fig. 5). The slices of the cartilages obtained with our slicer were structurally integral and functionally stable. There was no damage or undue breakage, crushing or wastage of the cartilage after slicing with our cartilage slicer. The thickness of the cartilages being reduced after slicing, makes its pliability, handling and placement comparable to the fascia (depending on the thickness of the metallic spacer used). The success of the sliced cartilage in terms of structural and functional outcome has already been published [19, 20].
Fig. 4.

Precise Slices of cartilages obtained from single tragal cartilage with Slice !t
Fig. 5.
a Sliced cartilage used for TM and attic reconstruction. b Reinforcement in the previous patient with only perichondrium obtained after placing 0.1 mm spacer of Slice !t
Discussion
The use of cartilage as a graft material in middle ear surgery has been increasing in the last few decades. Cartilage was first used in in middle ear surgery in 1959 by Utech [1]. In 1963, Salen and Jansen described cartilage–perichondrial composite graft for TM reconstruction [9]. Heermann was the main advocate and proponent of cartilage and used it as cartilage palisade technique since 1960 [9]. However, all the techniques mentioned and described in the literature are the ones using the full thickness cartilage. Controversy remains for the use of thick and rigid cartilage in tympanoplasty. The thickness and rigidity of the cartilage, though prevents retraction, re-perforation, it interferes with sound conduction raising a concern about the hearing. Studies by Huttenbrink and Zahnart [10] have suggested the acoustic transfer characteristics of cartilage with varying thickness. It was noted that cartilage graft with a thickness of less than 0.5 mm gave least acoustic transfer loss. The cartilage slicing techniques mentioned in the literature include random trimming of the cartilage with a razor or with cartilage slicers. The disadvantage of using a surgical blade for splitting the cartilage often wastes the remaining cartilage which cannot be used for further reconstruction. At present the cartilage slicers available include Kurz precise cartilage knife and Huttenbrink Cartilage Guide. The Huttenbrink Cartilage Guide has 2 cylinders one inserted into the other. Our cartilage slicer, Slice !t is a modification of the previous slicers.
How Slice !t is Different From Other Previous Slicers
Structurally, the cartilage holding unit (Figs. 1, 2, 3) is broader than the routine available slicers and has a multi-utility role. It is provided with additional spacer of 0.5 mm. Functionally, our Slice!t has multi-utility functions with varied applications in middle ear surgery. It is more beneficial and cost effective compared to other cartilage slicers as it combines functions of cartilage slicer, measurement grid, prosthesis trimming device, Teflon piston cutting device and also allows preparation of slicing islands.
Benefits of Slice !T (Figs. 4, 5)
Produces precise slices of the cartilages without damaging or breaking the cartilage structurally.
The slices produced are pliable making its handling, placement comparable to the fascia and perichondrium (depending on the thickness of the metallic spacer) in cases of tympanic membrane reconstruction.
By placing the spacer of 0.1 mm, perichondrium can be harvested separately.
Allows precise slicing of cartilage (tragal, conchal or septal) 0.1–0.5 mm for tympanic membrane reconstruction as Shield sliced cartilage, composite perichondium-cartilage shield, sliced island, sliced mosaic, sliced shield or mosaic.
Can be used for slicing cartilage for Ossiculoplasty
Support for the Titanium prosthesis (precise slice piece over TORP or PORP)
Sliced cartilage can be used in Soft Canal wall reconstruction
Slices for Attic reconstruction and reinforcement for posterosuperior area
Measurements of length for titanium prosthesis TORP & PORP
Cutting TORP & PORP with decided length
Crimping of Kurz prosthesis at desired length
Cutting of stapes Teflon piston at desired length
Cartilage islands and palisades
Measurement of cartilage graft measurements for Rhinoplasty
Conclusion
Our modified cartilage slicer is a multi-utility device combining functions of cartilage slicer, measurement grid for graft measurement, fashioning island grafts, piston and prosthesis trimming. With little practice, the slicing techniques can be mastered within a short span of time.
Conflict of interest
Application for IPR to the Government of India under the Design act in the name of Dr. Mubarak Khan. And “SLICE !t” is tradename secured for this. Dr Sapna Parab has helped in preparing the manuscript and evaluated the use of the Cartilage slicer actively during various cartilage tympanoplasties independently and along with second author.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional committee and with the 1964 helsinski declaration and its later amendments or comparable ethical standards Institutional Ethics Committee has approved the study.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
References
- 1.Ben Gamra O, Mbarek C, et al. Cartilage graft in type I tympanoplasty: audiological otological outcome. Eur Arch Otorhinolaryngol. 2008;265:739–742. doi: 10.1007/s00405-008-0645-5. [DOI] [PubMed] [Google Scholar]
- 2.Dornhoffer JL. Cartilage tympanoplasty. Otolaryngol Clin N Am. 2006;39:1161–1176. doi: 10.1016/j.otc.2006.08.006. [DOI] [PubMed] [Google Scholar]
- 3.Loeb L. Autotransplantation and homotransplantation of cartilage in the guinea pig. Am J Pathol. 1926;2:111–122. [PMC free article] [PubMed] [Google Scholar]
- 4.Kerr AG, Byrne JE, Smyth GD. Cartilage homografts in the middle ear: a long-term histological study. J Laryngol Otol. 1973;87(12):1193–1200. doi: 10.1017/S0022215100078166. [DOI] [PubMed] [Google Scholar]
- 5.Murbe D, Zahnert T, Bornitz M, Huttenbrink KB. Acoustic properties of different cartilage reconstruction techniques of the tympanic membrane. Laryngoscope. 2002;112:1769–1776. doi: 10.1097/00005537-200210000-00012. [DOI] [PubMed] [Google Scholar]
- 6.Lee CF, Chen JH, Chou YF, Hsu LP, Chen PR, Liu TC. Optimal graft thickness for different sizes of tympanic membrane perforation in cartilage myringoplasty: a finite element analysis. Laryngoscope. 2007;117:725–730. doi: 10.1097/mlg.0b013e318031f0e7. [DOI] [PubMed] [Google Scholar]
- 7.Bernal-Sprekelsen M, Romaguera Lilso MD, Sanz Gonzalo JJ. Cartilage palisades in type III tympanoplasty: anatomic and functional long term results. Otol Neurotol. 2003;24:38–42. doi: 10.1097/00129492-200301000-00009. [DOI] [PubMed] [Google Scholar]
- 8.Uslu C, Tek A, Tatlipinar A, et al. Cartilage reinforcement tympanoplasty: otological and audiological results. Acta Otolaryngol. 2010;130:375–383. doi: 10.3109/00016480903145346. [DOI] [PubMed] [Google Scholar]
- 9.Yung M. Cartilage tympanoplasty: literature review. J Laryngol Otol. 2008;122:663–672. doi: 10.1017/S0022215108001813. [DOI] [PubMed] [Google Scholar]
- 10.Zahnert T, Huttenbrink KB, Murbe D, Bornitz M. Experimental investigations of the use of cartilage in tympanic membrane reconstruction. Am J Otol. 2000;21:322–328. doi: 10.1016/S0196-0709(00)80039-3. [DOI] [PubMed] [Google Scholar]
- 11.Dornhoffer JL. Hearing results with cartilage tympanoplasty. Laryngoscope. 1997;107:1094–1099. doi: 10.1097/00005537-199708000-00016. [DOI] [PubMed] [Google Scholar]
- 12.Khan MM, Parab SR. Primary cartilage tympanoplasty: our technique and results. Am J Otolaryngol. 2011;32(5):381–387. doi: 10.1016/j.amjoto.2010.07.010. [DOI] [PubMed] [Google Scholar]
- 13.Khan MM, Parab SR (2013) Reinforcement of sliced tragal cartilage perichondrium composite graft with temporalis fascia in type I tympanoplasty: our techniques and results. J Rhinolaryngo.-Otologies 1:57–62. https://pdfs.semanticscholar.org/bf87/b72ac380b8f2d3bfd22fc56e6b3825c3e7ae.pdf
- 14.Khan MM, Parab SR. Day care ear surgery: our experience of 4 years. Indian J Otolaryngol Head Neck Surgery. 2012;64(3):280–284. doi: 10.1007/s12070-011-0303-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Khan MM, Parab SR (2014) Sliced island tragal cartilage perichondrial composite graft: early results and experience. J Rhinolaryngo-Otologies 2:4–9. https://pdfs.semanticscholar.org/99d9/f92402e6fe88186dd53c26e8e50e4282dcdc.pdf
- 16.Khan MM, Parab SR. Comparative study of sliced tragal cartilage and temporalis fascia in type I tympanoplasty. J Laryngol Otol. 2015;129(1):16–22. doi: 10.1017/S0022215114003132. [DOI] [PubMed] [Google Scholar]
- 17.Khan MM, Parab SR. Average thickness of tragal cartilage for slicing techniques in tympanoplasty. J Laryngol Otol. 2015;129(05):435–439. doi: 10.1017/S0022215115000055. [DOI] [PubMed] [Google Scholar]
- 18.Khan MM, Parab SR. Novel concept of attaching endoscope holder to microscope for two handed endoscopic tympanoplasty. Indian J Otolaryngol Head Neck Surgery. 2016;68(2):230–240. doi: 10.1007/s12070-015-0916-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Khan MM, Parab SR. Endoscopic cartilage tympanoplasty: a two-handed technique using an endoscope holder. Laryngoscope. 2016;126:1893–1898. doi: 10.1002/lary.25760. [DOI] [PubMed] [Google Scholar]
- 20.Parab SR, Khan MM. Minimal invasive endoscopic ear surgery: a two handed technique Indian. J Otolaryngol Head Neck Surg. 2018 doi: 10.1007/s12070-018-1411-7. [DOI] [PMC free article] [PubMed] [Google Scholar]