
Figure 3.
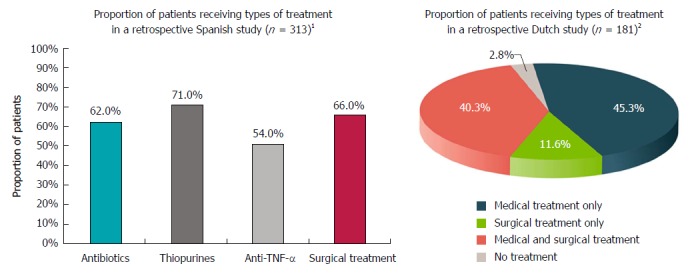
Treatment choices. 1Retrospective multicentre study (study period or median follow-up time were not reported) enrolling patients with Crohn’s disease (CD) and PFs; 80% had complex perianal fistulas (CPF). The graph presents treatment selection for patients with any fistula. Patients could have received multiple treatments (proportion of patients who received combination therapy was not reported). The most common surgical intervention was fistulotomy (37%), followed by placement of setons (32%)[18]. 2Retrospective single-centre study enrolling patients with CD and any perianal fistula [n = 232 patients, of which 181 (78%) had CPF]; patient identification: 1980-2000, follow-up through January 1, 2010; median follow-up was 10.0 yr (range, 0.5-37.5 yr). The graph presents treatment choices for 181 patients with CD and CPF. The most common type of surgery (alone or in combination with medical treatment) was faecal diversion (stoma; 63.6% of 94 patients with CPF who underwent surgery; 33.1% of all 181 patients with CPF), followed by colectomy (55.3% of patients with CPF who underwent surgery; 28.7% of all patients with CPF), fistulectomy (42.6% of patients with CPF who underwent surgery; 22.1% of all patients with CPF), and rectum amputation (proctectomy; 25.5% of patients with CPF who underwent surgery; 13.3% of all patients with CPF)[13].