

Abstract
Introduction:
General practitioners’(GPs) role is important as they are easily accessible especially for elderly. Young GPs need to improve their attitudes toward the elderly so that they can be a part of solution for health problems of elderly in the future. The aim of this study is to determine attitudes of young GPs toward elderly by the University of California at Los Angeles Geriatrics Attitude Scale (UCLA-GAS).
Methods:
It is a cross-sectional study performed with questionnaires including UCLA-GAS. The study population was 260 young doctors (GP residents and GPs in their first 5 years after qualification). Statistical evaluation of the data included percentage, mean, and Kolmogorov–Smirnov test and analysis of variance test.
Results:
Of the participants, 58.1% (n = 151) were women, 35.4% (n = 94) of them were GPs, and the remaining were GP residents. The mean age was 31.30 ± 5.40 years (range = 24–55 years). The mean score of UCLA-GAS was 46.85 ± 5.63 (range = 30–61). Participants ≤30 years of age had significantly higher scores (47.70 ± 5.99) than age above 30 years (45.68 ± 4.89) (P = 0.003). There was no statistically significant difference between GP residents and GPs (P = 0.989) and between participants who had rotation in elderly healthcare service (n = 63) or not (n = 197) (P = 0.383). However, as the duration of work increased, the score of UCLA-GAS decreased significantly (r = −0.216, P < 0.001).
Conclusion:
Young doctors who were interested in elderly showed more positive attitude as expected. However, the ones who were older and worked longer had less positive attitude. It seems important to understand and prevent this unfavourable attitude with formal education system about elderly healthcare during residency.
Keywords: Elderly care, University of California at Los Angeles Geriatrics Attitude Scale, young doctors
Introduction
Population aging is a global phenomenon in recent years. Future projections show that population of age 65 years and older in 2025 will constitute 9.8% of total population all over the world, and in 2050, there will be 2 billion people over the age 60 of years and above.[1] According to the official figures of TUIK (2016) in Turkey, population of 65 years and older constitutes 8.2% of total population in 2015.[2] Population of age 65 and older in Turkey based on 2015 data will reach to 8,435,000 from 6,495,239. It is expected to be 19.5 million in 2050 and 24.7 million in 2075. The proportion of elderly population in the total population will be 20.8% in 2050 and 27.7% in 2075, respectively.
Aging leads to a decrease in the structure and function of the body leading to a decrease in the ability to maintain homeostasis and more vulnerable individuals to trauma, drugs, and environmental changes. By aging, many systems such as cardiovascular system and musculoskeletal system lose their ability to supply the need of the body as the person ages. As individuals live longer, they suffer from chronic illnesses more.[3] Nowadays, with the reality of living longer it becomes a necessity to create a healthy aging environment to decrease the risks and prevent complications of chronic diseases so that their quality of life can be improved. This need is driving a rising demand for primary healthcare services that are more cost-effective and accessible for elderly population and therefore that increases the responsibility of primary healthcare providers.
Nevertheless, there are few studies that elicit the attitude of young healthcare providers and students. In a study by Hobbs et al., they addressed the change in attitudes of physiotherapy students during graduation program. According to the results of the study, over the time of training, positive attitudes of the students have improved.[4] In another study on medical students, it was shown that the attitude of medical students is associated with the knowledge and experiences of the students,[5] and the education and training in this topic is crucial to increase the positive attitude.
As provision of the healthcare services to the elderly in Turkey is performed either by the GP in primary healthcare or the internal medicine physician or the geriatrician in secondary or tertiary care, elderly health education in the curriculum of medical faculty and nursing faculty becomes crucial. Determination of attitude of healthcare providers in primary healthcare, especially GPs toward elderly, is more important for the initial assessment of current education programs and for planning future ones. Because they are the first contact and the most accessible ones who deal with the elderly population in their own routine. Notwithstanding, there was not much information about the attitude of young GPs.
Furthermore, young GPs’ role is more important as their positive attitudes toward the elderly can lead them to be a part of solution for elderly's health problems.
In this article, “Young Doctor” term is used for the residents or the qualified GPs in their first 5 years after qualification by World Organization of National Colleges, Academies and Academic Associations of General Practitioners/Family Physicians.[6]
In this study, it is aimed to address the attitudes of young GP residents and GPs in their 5 years of qualification toward elderly population in Turkey.
Materials and Method
At the time of the study, there were 850 GP residents and 1500 GPs within their first 5 years after qualification in Turkey. The study has a cross-sectional descriptive design using a sociodemographic questionnaire in addition to the University of California at Los Angeles Geriatrics Attitude Scale (UCLA-GAS). The questionnaires were applied to participants through online method, and the convenience sample of study population was 260 young GPs.
The sociodemographic questionnaire included questions such as age, gender, working position, years of work, affiliation, elderly education history, and past history of work experience in an elderly facility.
In addition, the 14-question UCLA-GAS that is the most frequent used scale that assesses attitude toward elderly was used. The scale was designed to assess general impressions about the elderly, perceived value of the elderly, and distributive justice of societal resources toward them. Its reliability and validity were proven by Reuben et al.,[7] and Turkish validity and reliability of UCLA-GAS were studied in pregraduate and postgraduate healthcare providers by Sahin et al. and the Cronbach's alpha score was found to be 0.67 (2012).[8]
Items of the scale were assessed with the scale of 5-point Likert types with options of “I don’t agree absolutely,” “I don’t agree,” “I am indecisive,” “I agree,” and “I absolutely agree.” Total four aspects are seen as being “social values, medical care, compassion, resources distribution.” Total attitude score comprises these four aspects. The highest score is 70 and it is understood that as the score increases, individual has more positive attitude.
Analysis of data was performed in SPSS 15.0 statistical software program. In the beginning, compliance test for normal distribution with Kolmogorov–Smirnov test was applied to dependent variables (UCLA-GAS scores) and consistency with parametric test criteria was assessed. For statistical analysis, P < 0.05 value was accepted as statistically significant. The results were expressed as mean ± standard deviation. The associations between the scores of the scale and the sociodemographic characteristics of the participants were analyzed with t-test and analysis of variance.
Results
Of the participants, 58.1% (n = 151) was women and 41.9% (n = 109) of them was male. About 60.4% (n = 157) of the participants were residents, 36.2% (n = 94) were qualified GPs in their 5 years, and 3.5% (n = 9) of them were half-time residents. The mean age of the participants was 31.30 ± 5.40 years (range = 24–55 years) and the mean working duration was 21.95 ± 18.95 months.
The percentage of the population who had elderly health education during residency was 24.3% (n = 63) and the percentage who did not have was 75.7% (n = 197). Furthermore, when the number of participants who had taken additional voluntary education was questioned, the study showed that 8.8% (n = 23) of the population had voluntary education and 91.2% (n = 237) did not have any.
The mean score of UCLA-GAS was 46.85 ± 5.63 (range = 30–61) and Cronbach's alpha value is calculated as 0.626 in our study.
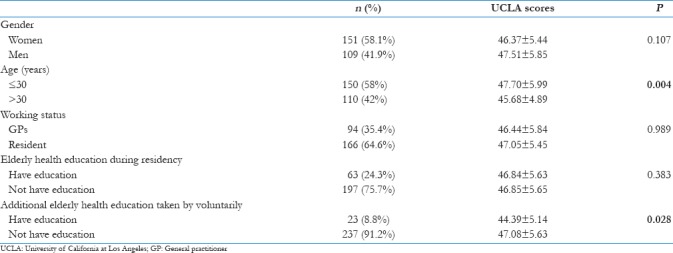
According to Table 1, although men got higher UCLA scores than women (47.51 ± 5.85 and 46.37 ± 5.44, respectively), it was not statistically significant (P = 0.107). On the other hand, people age 30 years and below got higher scores (47.70 ± 5.99) compared to those over 30 (45.68 ± 4.89) years, and it was statistically significant (P = 0.004). The residents got higher scores (47.05 ± 5.45) than the GPs (46.44 ± 5.84), but it was statistically insignificant (P = 0.989). Likewise, participants who had no elderly health education during residency got higher UCLA scores (46.85 ± 5.65) than who had education (46.84 ± 5.63). However, it was statistically insignificant either (P = 0.383). When having additional education voluntarily and UCLA score were analyzed, it was found that participants who did not have education got higher scores (47.08 ± 5.63) compared to participants who had education (44.39 ± 5.14) and it was statistically significant (P = 0.028).
Table 1.
UCLA scores of the participants
Discussion
This study determined attitudes of young GPs toward elderly by UCLA-GAS as it can be an important basis for present and future education and practice planning of GPs. However, there are limited numbers of study on this topic including GPs, and therefore the issue was discussed with the results of other healthcare professionals.
It was determined that residents had higher scores than GPs in our study, but it was not significant. This case can be associated with dealing with elderly population in primary healthcare centers more than residency period. Increased amount of elderly consultations, facing with comorbidities, and having difficulties to deal with them may result in less positive attitude toward elderly. Another reason could be burn-out of GPs who already worked with elderly people longer than the residents.
A significant association was found between ages of young GPs and their attitude toward the elderly in our study. It was determined that as the ages of doctors increase, their attitudes were found to be more negative. It will be related to education because education about elderly healthcare is a new topic in Turkey and most of the older GPs did not have the chance to be educated on this topic. Contrary to this, the study about the attitudes of healthcare providers in China toward the elderly during the period of pregraduation was determined as more positive for upper classes of students of physiotherapy, diet, nursing, and medical faculty and the ones with geriatrics education.[4,9,10] This might be related to the extent of questions of UCLA scale. As age and level of education increase, these students might feel more confident in dealing with elderly population.
No association was found between gender of GPs and their attitude toward the elderly. There are different results reported about this subject. While Shahidi and Devlen[11] and Usta et al.[12] identified a relation with positive attitude of woman and living with an old person, Cankurtaran et al.[5] did not find such a relation.
In some studies, it was found that students of school of nursing including both gender have more positive attitudes than students of medical faculty and it is related to the fact that students of nursing school meet elderly more and spend more time with them during their training.[10,11,12] Also, in some studies including nursing students, it was determined that attitudes of the ones living with old relative are more positive.[5,12,13,14]
One of the limitations of our study is not to ask participants whether they were living with an old relative and have an opportunity to learn how to deal with them. Attitude score was found significantly higher for the group with education than the group with no education in many studies.[5,12,13,14] But in our study, there was no significant difference between educated and non-educated ones. Beside this, participants who did not have education voluntarily had higher scores in our study compared to the voluntary ones. An explanation for that could be in Turkish GP training curriculum; there is not a standardized education toward elderly care, and on the other side, there is a geriatric population with complicated problems. Due to this, it is obvious that non-formal education attempts were unsuccessful to create an elderly care-friendly environment for GPs.
Physicians who were older had less positive attitude. It seems important to understand and prevent this unfavorable attitude with formal education system about elderly healthcare during residency. According to further analysis between UCLA and other sociodemographics, it seems that there are other factors affecting the positive attitude among elderly population.
Conclusion
Overall, unfortunately, beside the aging population with comorbidities, there is no formal rotation in elderly healthcare services in Turkey that exist in many countries such as the Netherlands and Denmark to understand the importance of elderly life. There is an obvious necessity to elicit the problems in the current voluntary educations to keep the positive attitude of the young doctors. In future, some improvements to better understand the relationship of positive attitude toward elderly with other factors and structured education interventions should be studied. Additionally, some international studies on attitudes of young doctors and other healthcare givers also should be addressed to discuss the global view, and common programs should be created to give the best care to the elderly population in aging world.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.World Health Organization. World report on ageing and health. World Health Organization. 2015 [Google Scholar]
- 2.Elderly Statistics, 2016 [Internet]. Turkish Statistical Institute; 2017 [cited 2017 Jun 20]. Report No. 24644. [Last accessed on 2017 Mar 05]. Available from: http://www.turkstat.gov.tr/PreHaberBultenleri.do?id=24644 .
- 3.Chatterji S, Byles J, Cutler D, Seeman T, Verdes E. Health, functioning, and disability in older adults—Present status and future implications. Lancet. 2015;385:563–75. doi: 10.1016/S0140-6736(14)61462-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hobbs C, Dean CM, Higgs J, Adamson B. Physiotherapy students’ attitudes towards and knowledge of older people. Aust J Physiother. 2006;52:115–9. doi: 10.1016/s0004-9514(06)70046-0. [DOI] [PubMed] [Google Scholar]
- 5.Cankurtaran M, Halil M, Ulger Z, Dagli N, Yavuz BB, Karaca B, et al. Influence of medical education on students’ attitudes towards the elderly. J Natl Med Assoc. 2006;98:1518. [PMC free article] [PubMed] [Google Scholar]
- 6.Europe W. The European Definition of General Practice/Family Medicine. Barcelona: WONCA Europe; 2002. [Google Scholar]
- 7.Reuben DB, Lee M, Davis JW, Eslami MS, Osterweil DG, Melchiore S, et al. Development and validation of a geriatrics attitudes scale for primary care residents. J Am Geriatr Soc. 1998;46:1425–30. doi: 10.1111/j.1532-5415.1998.tb06012.x. [DOI] [PubMed] [Google Scholar]
- 8.Sahin S, Mandiracioglu A, Tekin N, Senuzun F, Akcicek F. Attitudes toward the elderly among the health care providers: Reliability and validity of Turkish version of the UCLA Geriatrics Attitudes (UCLA-GA) scale. Arch Gerontol Geriatr. 2012;55:205–9. doi: 10.1016/j.archger.2011.08.015. [DOI] [PubMed] [Google Scholar]
- 9.Yen C-H, Liao WC, Chen Y-R, Kao MC, Lee MC, Wang CC. A Chinese version of Kogan's attitude toward older people scale: Reliability and validity assessment. Int J Nurs Stud. 2009;46:38–44. doi: 10.1016/j.ijnurstu.2008.05.004. [DOI] [PubMed] [Google Scholar]
- 10.Wang T, Lu C, Chen I, Yu S. Sexual knowledge, attitudes and activity of older people in Taipei, Taiwan. J Clin Nurs. 2008;17:443–50. doi: 10.1111/j.1365-2702.2007.02003.x. [DOI] [PubMed] [Google Scholar]
- 11.Shahidi S, Devlen J. Medical students’ attitudes to and knowledge of the aged. Med Educ. 1993;27:286–8. doi: 10.1111/j.1365-2923.1993.tb00270.x. [DOI] [PubMed] [Google Scholar]
- 12.Usta YY, Demir Y, Yönder M, Yildiz A. Nursing students’ attitudes toward ageism in Turkey. Arch Gerontol Geriatr. 2012;54:90–3. doi: 10.1016/j.archger.2011.02.002. [DOI] [PubMed] [Google Scholar]
- 13.Fajemilehin BR. Attitudes of students in health professions toward caring for older people: Needed curricula revisions in Nigeria. Educ Gerontol. 2004;30:383–90. [Google Scholar]
- 14.Rejeh N, Heravi-Karimooi M, Montazeri A, Foroughan M, Vaismoradi M. Psychometric properties of the Iranian version of the Kogan's attitudes toward older people scale. Jpn J Nurs Sci. 2012;9:216–22. doi: 10.1111/j.1742-7924.2012.00204.x. [DOI] [PubMed] [Google Scholar]