
Figure 2.
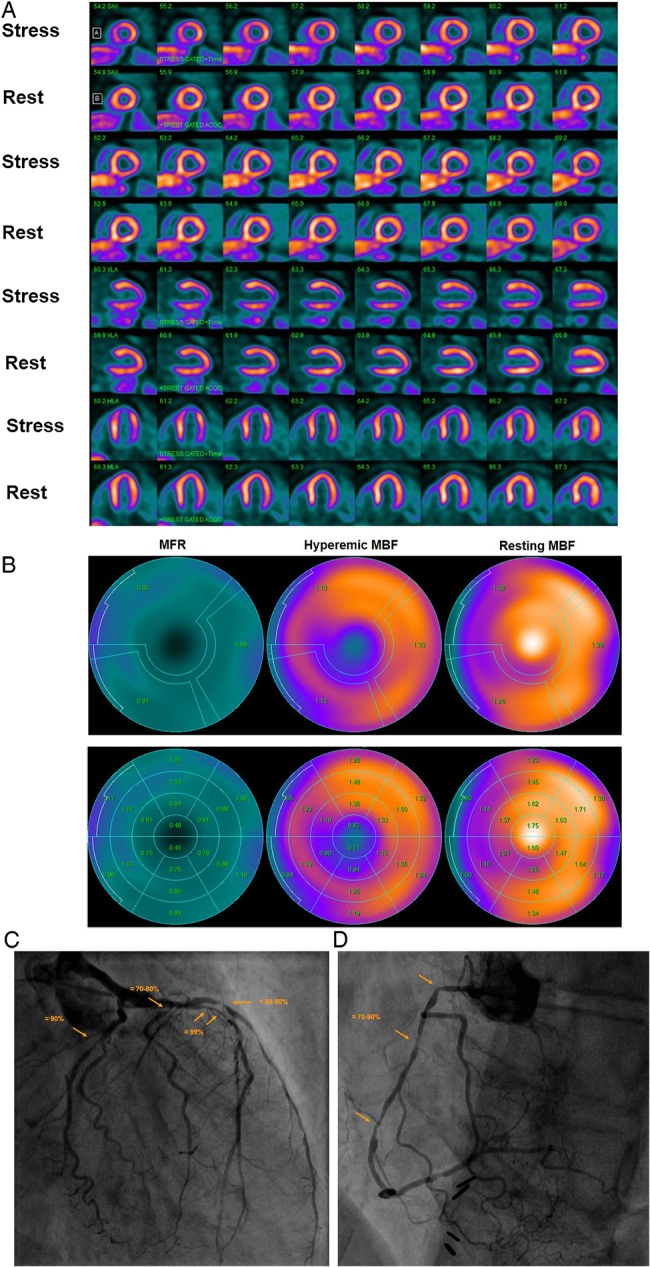
Abnormal stress-rest myocardial perfusion and MBF study with 13N-ammonia PET/CT in a 58-year-old man with typical, effort-induced chest pain. (A) Regadenoson-stress and rest 13N-ammonia PET/CT images in corresponding short-axis (top), vertical long-axis (middle), and horizontal long-axis (bottom) slices. On stress images, a moderate-to-severe decrease in myocardial perfusion, involving the antero-septo-apical and apical wall, is realized that becomes reversible on rest images and thus signifies ischaemia in the LAD distribution. (B) Regional MBF quantification demonstrates abnormally reduced hyperaemic MBFs and MFR in all three major coronary artery territories of the LAD, LCx, and RCA, respectively (upper panel). Segment MBF analysis unravels a decrease in MBF from the mid- to distal segments with a mean longitudinal MBF gradient during hyperaemic flow in the LAD (0.12 mL/g/min), LCx (0.19 mL/G/min), and RCA (0.30 mL/g/min) (lower-middle panel). (C) Invasive coronary angiography of the left coronary artery in this patient demonstrated a long 99% stenosis in the mid-LAD that accounted for the observed stress-induced perfusion defect antero-apical and apical on 13N-ammonia PET/CT perfusion images. In addition, large calibre diagonal branches of the LAD present a ≈70–80% and ≈80–90% stenosis, respectively. The proximal LCx has a proximal ≈80–90% stenosis. Invasively measured FFR of the proximal LCx lesion was abnormally reduced with 0.68 signifying also downstream flow-limiting effects of this lesion. (D) Invasive coronary angiography of the right coronary artery demonstrates serial epicardial lesion from the proximal to mid-segments of ≈70–90%, respectively.