

Abstract
Background
Popliteal artery aneurysms (PAAs) are generally complicated by thrombosis and distal embolization, whereas rupture is rare. The aim of this study was to describe the clinical characteristics and outcome in a cohort of patients who had surgery for ruptured PAA (rPAA).
Methods
Operations for rPAA were identified from the Swedish Vascular Registry, Swedvasc, 1987–2012. Medical records and imaging were reviewed. Comparison was made with patients treated for PAA without rupture.
Results
Forty‐five patients with rPAA were identified. The proportion with rupture among those operated on for PAA was 2·5 per cent. Patients with rPAA were 8 years older (77·7 versus 69·7 years; P < 0·001), had more lung and heart disease (P = 0·003 and P = 0·019 respectively), and a larger mean popliteal aneurysm diameter (63·7 versus 30·9 mm; P < 0·001) than patients with PAA treated for other indications. At time of surgery, 22 of 45 patients were already receiving anticoagulants, seven for concomitant deep venous thrombosis (DVT) in the affected leg. There was extensive swelling of the whole leg in 20 patients. In 27 patients, the initial diagnosis was DVT or a Baker's cyst. All patients underwent surgery, all but three by the open method. There were four amputations, all performed within 1 week of surgery. One year after surgery, 26 of the 45 patients were alive. Among these, the reconstructions were patent in 20 of 22 patients.
Conclusion
The diagnosis of rPAA is difficult, and often delayed. The condition affects old patients, who often are on anticoagulation treatment and have large aneurysms. The immediate surgical results are acceptable, but the condition is associated with a high risk of death within the first year after surgery.
Short abstract
Diagnosis often delayed
Introduction
Popliteal artery aneurysm (PAA) is the most common of the peripheral aneurysms, but is still rare. Trickett and colleagues1 screened 1070 men aged 65–80 years, identifying 11 (1·0 per cent) with a PAA diameter between 15 and 26 mm1. Contemporary population‐based prevalence data are lacking. The fact that the prevalence of abdominal aortic aneurysm (AAA) is decreasing2, 3 suggests that the prevalence of PAA could also be falling4, 5, as PAA is often associated with multianeurysm disease. The number of operations for PAA in Sweden has doubled from 1994–20016 to 2008–20127, although this may be a result of improved diagnosis.
Thrombosis and distal embolization are the most common complications of PAA, and can lead to severe limb‐threatening ischaemia6, 8. The proportion of ruptured popliteal aneurysms (rPAAs), among all patients operated on for PAA, is 2–5 per cent in larger series6, 7, 9, 10. Many centres use a diameter of 2 cm, with or without thrombus, as the indication for prophylactic surgery, supported by the American College of Cardiology/American Heart Association peripheral artery disease 2005 guidelines11. The risk of rupture of PAA with different diameters is virtually unknown.
Previous publications on PAA consist of case reports and small case series. The condition is often misdiagnosed as deep venous thrombosis (DVT), ruptured Baker's cyst or acute limb ischaemia7, 12, 13.
The aim of this study was to describe the clinical characteristics and outcome in patients with rPAA, and to compare them with those of patients who were treated for non‐ruptured PAA.
Methods
The Swedish Vascular Registry, Swedvasc, was created in January 1987 and since 1992 has registered more than 90 per cent of all open and endovascular procedures14. In 2008, a special module for PAA was added to the registry. Independent international validation has shown excellent external and internal validity15. There has also been a specific validation of the registration of patients treated for PAA in the Swedvasc. Ravn and colleagues4 took advantage of the fact that PAAs often are bilateral. Of the 146 bilateral procedures, 141 (96·6 per cent) had been reported to the registry.
Two cohorts were combined for the present study. In 2007, Ravn et al.6 used data from Swedvasc to study a nationwide cohort of 717 legs treated for PAA, of which 24 (3·3 per cent) were treated for rupture. In a recently published study7 using the same registry, 592 PAAs treated between 2008 and 2012 were described. Of these, 13 had been rPAAs (2·2 per cent). Another 12 separate patients with rPAA during 2002–2008 were added, as well as one operated on in 2001 but registered in 2002. The patients treated for rPAA during these three time intervals were merged into one data set. Prospectively entered registry data were supplemented with data from the case records and imaging, collected retrospectively from 20 different hospitals.
In all, 50 patients treated for rPAA were identified but, when the case records were scrutinized, one was registered twice and four patients had been treated for post‐traumatic pseudoaneurysms. Thus, 45 patients treated for rPAA remained for study.
Characteristics of the patients with rPAA were compared with those of patients with PAA treated for other indications, using original data from the two previously published nationwide studies6, 7. In the nationwide studies, there was some difference in the data collected. The earlier cohort had data on size and other aneurysm disease6. The latter had data on background disease7.
The Ethics Committee of the Uppsala region approved the study.
Statistical analysis
The distribution of continuous variables was assessed by histogram and Q‐Q plots. Independent‐samples t test was used to evaluate differences in continuous variables between groups, and Pearson correlation coefficient to estimate the correlation between patient age and rPAA size. Differences in proportions were evaluated using Fisher's exact test. All statistical analyses were performed using the software package SPSS version 23.0 (IBM, Armonk, New York, USA).
Results
To calculate the proportion of patients who had surgery for rPAA, the time intervals 1987–2002 and 2008–2012 were used, for which complete data were available on the total number of repairs (1304) as well as the number of operations for rPAA (33); the proportion was 2·5 per cent.
Patients with rPAA were older (P < 0·001) and had more lung and heart disease (P = 0·003 and P = 0·019 respectively) than with those with PAA treated for other indications (Table 1). Among the patients with non‐ruptured PAA, there were no significant differences in this regard between those treated urgently or electively. The maximum diameter of the rPAA was assessed in 38 patients, by CT (17), ultrasonography (16), MRI (2) and perioperative measurement (3) (Fig. 1). The mean maximum rPAA diameter was 63·7 (range 25–200) mm (Table 2). There was no correlation between patient age and rPAA diameter (Pearson r = 0·046, P = 0·777).
Table 1.
Clinical characteristics of patients who had surgery for ruptured or non‐ruptured popliteal artery aneurysm
| Rupture (n = 45) | Other indications (n = 579† or 693‡) | P § | |
|---|---|---|---|
| Mean age (years)* | 77·7 (59–96) | 69·7 (42–102)† | < 0·001¶ |
| Male sex | 43 of 45 (96) | 554 of 579 (95·7)† | 1·000 |
| Heart disease | 18 of 44 (41) | 131 of 542 (24·2)† | 0·019 |
| Hypertension | 22 of 43 (51) | 365 of 544 (67·1)† | 0·063 |
| Respiratory disease | 12 of 43 (28) | 60 of 529 (11·3)† | 0·003 |
| Diabetes | 3 of 44 (7) | 77 of 574 (13·4)† | 0·250 |
| Cerebrovascular disease | 9 of 43 (21) | 59 of 537 (11·0)† | 0·079 |
| Smoker | |||
| Never | 6 of 25 (24) | 89 of 440 (20·2)† | 0·686 |
| Former | 14 of 25 (56) | 229 of 440 (52·0)† | |
| Active | 5 of 25 (20) | 122 of 440 (27·7)† | |
| PAA diameter (mm)* | 63·7 (25–200) | 30·9 (10–150) | < 0·001¶ |
| (n = 38) | (n = 513)‡ | ||
| Concomitant AAA | 14 of 39 (36) | 236 of 687 (34·4)‡ | 0·863 |
| Bilateral PAA | 19 of 37 (51) | 388 of 687 (56·5)‡ | 0·611 |
Values in parentheses are percentages unless indicated otherwise:
values are mean (range). The clinical subgroups refer to legs, not patients.
Original data from 579 patients with non‐ruptured popliteal artery aneurysm (PAA) treated between 2008 and 2012;
original data from 693 legs with non‐ruptured PAA treated between 1987 and 2002. AAA, abdominal aortic aneurysm.
Fisher's exact test, except
independent‐samples t test.
Figure 1.
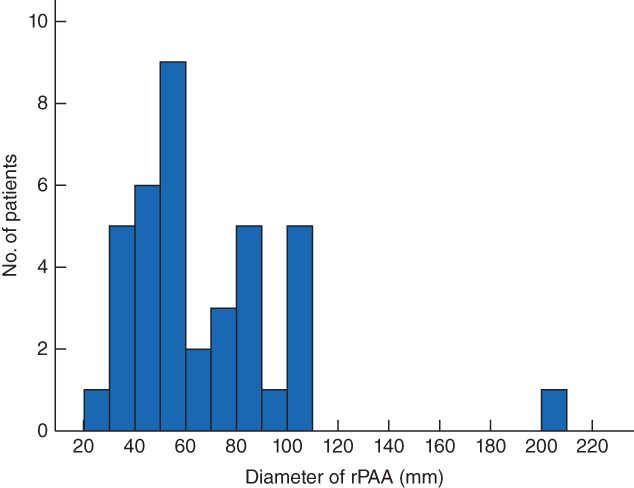
Ruptured popliteal artery (rPAA) diameter
Table 2.
Surgical technique and outcome in 45 patients treated for ruptured popliteal aneurysm
| No of patients (n = 45) | |
|---|---|
| Surgical approach | |
| Endovascular | 3 |
| Open, medial | 35 |
| Open, posterior | 3 |
| Open, ligation only | 3 |
| Open, direct anastomosis | 1 |
| Graft material (n = 38) | |
| Venous | 22 |
| Prosthetic | 14 |
| Composite | 2 |
| Outflow vessels (n = 33) | |
| 0 | 5 |
| 1 | 12 |
| 2 | 4 |
| 3 | 12 |
| Fasciotomy | 12 |
| 30‐day outcomes | |
| Patency | 35 of 39 |
| Amputation | 4 of 45 |
| Survival | 40 of 45 |
| 1‐year outcomes | |
| Patency | 20 of 22 |
| Amputation | 4 of 44* |
| Survival | 26 of 45 |
The total number of amputations did not increase but one of the patients alive at 1 year was lost to follow‐up.
Treatment
Most patients had open surgery by a medial approach. The surgical techniques and outcomes are described in Table 2. Fasciotomy was performed in 12 of 45 patients and four legs were amputated within 30 days. At 1 year, 26 patients were alive. The cause of death was uncertain in most patients who died within 1 year after surgery, owing to a low autopsy rate, but three were known to have died from aortic rupture/dissection and two from cancer.
Twenty‐two of 45 patients were being treated with anticoagulants at the time of surgery for rPAA, 19 with oral anticoagulants and three with low molecular weight heparins. Among these, seven had the treatment started within 2 months before being diagnosed with rPAA because of suspicion of DVT. The remaining 15 patients were receiving chronic anticoagulation treatment, mostly for atrial fibrillation or pulmonary embolism. Seven patients presented with critical leg ischaemia. One patient was hypotensive on admission, but quickly stabilized; another had fainted at home, but was stable on admission. No patient was in severe shock at presentation. Almost half of the patients (18 of 42) presented on the day their symptoms started and another 11 (in all 29 of 42) within 1 week. It was sometimes difficult to identify the exact date of the rupture, as most ruptures were contained, and the diagnosis was often delayed.
The initial diagnosis was rPAA in only eight of the 45 patients, half of whom were known to have a PAA. Twenty‐seven patients had a preliminary diagnosis of DVT or a Baker's cyst. Bleeding because of minor trauma or anticoagulation was suspected in seven patients and no preliminary diagnosis could be identified in the remaining three. All patients had swelling, and in 20 the whole leg was affected. Two patients, with known PAAs, had sepsis; their aneurysms became infected and ruptured.
Discussion
Patients with rPAA were 8 years older than those treated for non‐ruptured PAA. The aneurysms were larger and the initial clinical picture misleading, resulting in frequent delays in diagnosis. The immediate outcome after surgery was good; however, there was a high risk of death within 1 year, not just explained by old age and frequent cardiopulmonary co‐morbidities. There were at least three cases of fatal aortic rupture/dissection. CT angiography of the aorta should be considered in patients who present with rPAA.
Rupture of PAA is an uncommon event in an uncommon disease. In other aneurysm disease, the major concern is the risk of rupture, which also guides the indication for treatment. In patients with PAA, however, the most common complication is ischaemia, and little is known about the few aneurysms that rupture. The largest cohorts before this investigation were published in 195316 and 196217, including 16 and 11 patients respectively. In neither of these studies were the specific characteristics of patients with rPAAs described, and pseudoaneurysms after trauma were also included. Roggo and co‐workers10 reported on 252 patients treated for PAA, of which six (2·4 per cent) were ruptured. Sie and colleagues9 analysed 89 patients who had surgery for 124 PAAs, and the six with rPAAs (4·8 per cent) were described in detail. The main finding was that the clinical presentation varied, with different and often incorrect preliminary diagnoses, a finding verified in the present study.
Here, the mean rPAA diameter of 63·7 mm was twice that of PAAs in patients who had surgery for other indications. It was tricky to measure the diameter of some of the largest rPAAs owing to difficulty in defining the wall of the aneurysm in a large haematoma. PAAs may reach a diameter over 10 cm without rupturing, and yet six ruptured in the present series despite having a diameter of only 30–40 mm. It is known that even small‐diameter PAAs sometimes rupture, and the risk was estimated recently among patients with AAAs and internal iliac artery aneurysms (IIAAs). In Finland, 8 per cent of ruptured AAAs were below 55 mm in diameter18. In a multinational study19, 6 per cent of IIAAs were smaller than 40 mm at the time of rupture. Thus, factors other than size influence the risk of rupture. In the present study, a known PAA ruptured during treatment for sepsis in two patients, suggesting that the aneurysms could have been infected, resulting in rapid expansion and rupture. The findings during surgery in both patients, and positive culture in one, confirmed the diagnosis of a mycotic aneurysm. Infection has been associated with a high risk of rupture of AAA20, 21.
Almost half of the patients were on an anticoagulant at the time of rupture. This was an unexpected and novel finding. Most had been treated for a long time and the anticoagulation may explain why the aneurysms grew so large without thrombosis or embolization. In others, swelling of the leg associated with a contained rupture may have been misinterpreted as a DVT. This was suspected in four of the seven patients who had anticoagulation treatment initiated within 2 months of the diagnosis and treatment of rPAA.
PAAs usually rupture into the popliteal space, confined by muscles and tendons. The main symptoms are pain and swelling, and the patients were often evaluated initially by specialists in internal medicine or orthopaedics. Twenty‐seven of the 45 patients in the present study had a preliminary diagnosis of DVT or Baker's cyst. Compression of the popliteal vein22 and development of DVT23 are well known complications of large PAAs, but 20 of the patients with an rPAA presented with swelling of the entire leg, which should not be expected when a DVT develops secondary to compression from a PAA. Pressure from a large PAA, or the haematoma in the event of rupture, can also cause neurological pain24, 25, adding further complexity to the challenge of reaching the correct diagnosis (Fig. 2).
Figure 2.
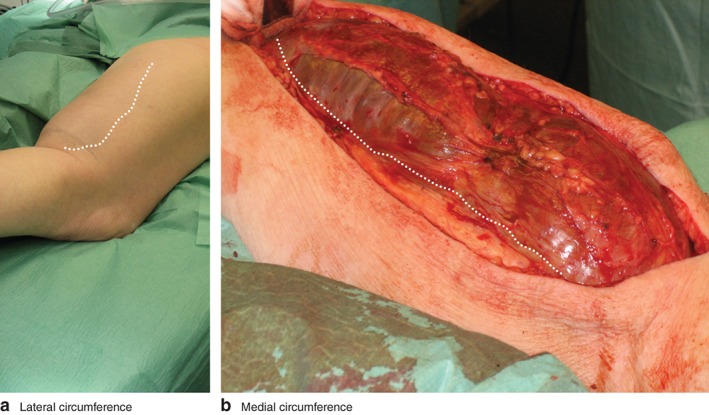
Ruptured popliteal artery aneurysm in the right leg. Note the bluish discoloration on top of the bulge just above the hollow of the knee. The dotted line delineates the a lateral and b medial circumference of the haematoma (courtesy of S. Acosta, Vascular Centre Malmö, Malmö, Sweden, and S. Mathiesen, Hamar Hospital, Hamar, Norway)
The results of surgery were acceptable, given the challenge of this rare condition. Among those who survived 1 year, all but two reconstructions were patent. Of four patients who needed an amputation, three presented with both ischaemia and rupture.
This study has limitations. The small numbers of rPAAs make the investigation prone to type II statistical error. However, it was possible to identify several differences between the small cohort of patients with rPAA and the larger cohort treated for non‐ruptured PAA. Furthermore, a long time interval was studied. The findings might have been different if a modern patient cohort alone had been investigated. Imaging and clinical pathways may have improved over time, although no such improvement could be detected in this small cohort.
Editor's comments

Acknowledgements
The authors are grateful to all vascular surgeons at the 20 hospitals who registered patients in Swedvasc; the local Swedvasc representatives who helped with patients records, especially R. Hultgren (Karolinska University Hospital) and S. Acosta (Skåne University Hospital, Malmö); and the Steering Committee of Swedvasc: L. Blomgren (chairman), B. Kragsterman, M. Jonsson, J. Starck, K. Björses, K. Djavani Gidlund, A. Daryapeyma and K. Mani.
Disclsoure: The authors declare no conflict of interest.
References
- 1. Trickett JP, Scott RA, Tilney HS. Screening and management of asymptomatic popliteal aneurysms. J Med Screen 2002; 9: 92–93. [DOI] [PubMed] [Google Scholar]
- 2. Svensjö S, Björck M, Gürtelschmid M, Djavani Gidlund K, Hellberg A, Wanhainen A. Low prevalence of abdominal aortic aneurysm among 65‐year‐old Swedish men indicates a change in the epidemiology of the disease. Circulation 2011; 124: 1118–1123. [DOI] [PubMed] [Google Scholar]
- 3. Jacomelli J, Summers L, Stevenson A, Lees T, Earnshaw JJ. Impact of the first 5 years of a national abdominal aortic aneurysm screening programme. Br J Surg 2016; 103: 1125–1131. [DOI] [PubMed] [Google Scholar]
- 4. Ravn H, Wanhainen A, Björck M. Risk of new aneurysms after surgery for popliteal artery aneurysm. Br J Surg 2008; 95: 571–575. [DOI] [PubMed] [Google Scholar]
- 5. Leake AE, Avgerinos ED, Chaer RA, Singh MJ, Makaroun MS, Marone LK. Contemporary outcomes of open and endovascular popliteal artery aneurysm repair. J Vasc Surg 2016; 63: 70–76. [DOI] [PubMed] [Google Scholar]
- 6. Ravn H, Bergqvist D, Björck M; Swedish Vascular Registry . Nationwide study of the outcome of popliteal artery aneurysms treated surgically. Br J Surg 2007; 94: 970–977. [DOI] [PubMed] [Google Scholar]
- 7. Cervin A, Tjärnström J, Ravn H, Acosta S, Hultgren R, Welander M et al Treatment of popliteal aneurysm by open and endovascular surgery: a contemporary study of 592 procedures in Sweden. Eur J Vasc Endovasc Surg 2015; 50: 342–350. [DOI] [PubMed] [Google Scholar]
- 8. Ravn H, Björck M. Popliteal artery aneurysm with acute ischemia in 229 patients. Outcome after thrombolytic and surgical therapy. Eur J Vasc Endovasc Surg 2007; 33: 690–695. [DOI] [PubMed] [Google Scholar]
- 9. Sie RB, Dawson I, van Baalen JM, Schultze Kool LJ, van Bockel JH. Ruptured popliteal artery aneurysm. An insidious complication. Eur J Vasc Endovasc Surg 1997; 13: 432–438. [DOI] [PubMed] [Google Scholar]
- 10. Roggo A, Brunner U, Ottinger LW, Largiader F. The continuing challenge of aneurysms of the popliteal artery. Surg Gynecol Obstet 1993; 177: 565–572. [PubMed] [Google Scholar]
- 11. Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL et al; American Association for Vascular Surgery; Society for Vascular Surgery; Society for Cardiovascular Angiography and Interventions; Society for Vascular Medicine and Biology; Society of Interventional Radiology; ACC/AHA Task Force on Practice Guidelines Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease; American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter‐Society Consensus; Vascular Disease Foundation. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter‐Society Consensus; and Vascular Disease Foundation. Circulation 2006; 113: e463–e654. [DOI] [PubMed] [Google Scholar]
- 12. Illig KA, Eagleton MJ, Shortell CK, Ouriel K, DeWeese JA, Green RM. Ruptured popliteal artery aneurysm. J Vasc Surg 1998; 27: 783–787. [DOI] [PubMed] [Google Scholar]
- 13. Ihlberg LH, Roth WD, Albäck NA, Kantonen IK, Lepäntalo M. Successful percutaneous endovascular treatment of a ruptured popliteal artery aneurysm. J Vasc Surg 2000; 31: 794–797. [DOI] [PubMed] [Google Scholar]
- 14. Troëng T, Malmstedt J, Björck M. External validation of the Swedvasc registry: a first‐time individual cross‐matching with the unique personal identity number. Eur J Vasc Endovasc Surg 2008; 36: 705–712. [DOI] [PubMed] [Google Scholar]
- 15. Venermo M, Lees T. International vascunet validation of the Swedvasc Registry. Eur J Vasc Endovasc Surg 2015; 50: 802–808. [DOI] [PubMed] [Google Scholar]
- 16. Gifford RW Jr, Hines EA Jr, Janes JM. An analysis and follow‐up study of one hundred popliteal aneurysms. Surgery 1953; 33: 284–293. [PubMed] [Google Scholar]
- 17. Friesen G, Ivins JC, Janes JM. Popliteal aneurysms. Surgery 1962; 51: 90–98. [PubMed] [Google Scholar]
- 18. Laine MT, Vänttinen T, Kantonen I, Halmesmäki K, Weselius EM, Laukontaus S et al Rupture of abdominal aortic aneurysms in patients under screening age and elective repair threshold. Eur J Vasc Endovasc Surg 2016; 51: 511–516. [DOI] [PubMed] [Google Scholar]
- 19. Laine MT, Björck M, Beiles CB, Szeberin Z, Thomson I, Altreuther M et al Few internal iliac artery aneurysms rupture under 4 cm. J Vasc Surg 2017; 65: 76–81. [DOI] [PubMed] [Google Scholar]
- 20. Sörelius K, Mani K, Björck M, Sedivy P, Wahlgren CM, Taylor P et al; European MAA Collaborators. Endovascular treatment of mycotic aortic aneurysms: a European multicenter study. Circulation 2014; 130: 2136–2142. [DOI] [PubMed] [Google Scholar]
- 21. Sörelius K, Wanhainen A, Furebring M, Björck M, Gillgren P, Mani K; Swedish Collaborator Group for Mycotic Abdominal Aortic Aneurysms. Nationwide study of the treatment of mycotic abdominal aortic aneurysms comparing open and endovascular repair. Circulation 2016; 134: 1822–1832. [DOI] [PubMed] [Google Scholar]
- 22. Haaverstad R, Fougner R, Myhre HO. Venous haemodynamics and the occurrence of leg oedema in patients with popliteal aneurysm. Eur J Vasc Endovasc Surg 1995; 9: 204–210. [DOI] [PubMed] [Google Scholar]
- 23. Huang Y, Gloviczki P, Noel AA, Sullivan TM, Kalra M, Gullerud RE et al Early complications and long‐term outcome after open surgical treatment of popliteal artery aneurysms: is exclusion with saphenous vein bypass still the gold standard? J Vasc Surg 2007; 45: 706–715.e1. [DOI] [PubMed] [Google Scholar]
- 24. Beaudry Y, Stewart JD, Errett L. Distal sciatic nerve compression by a popliteal artery aneurysm. Can J Neurol Sci 1989; 16: 352–353. [DOI] [PubMed] [Google Scholar]
- 25. Logigian EL, Berger AR, Shahani BT. Injury to the tibial and peroneal nerves due to hemorrhage in the popliteal fossa. Two case reports. J Bone Joint Surg Am 1989; 71: 768–770. [PubMed] [Google Scholar]