
Figure 7.
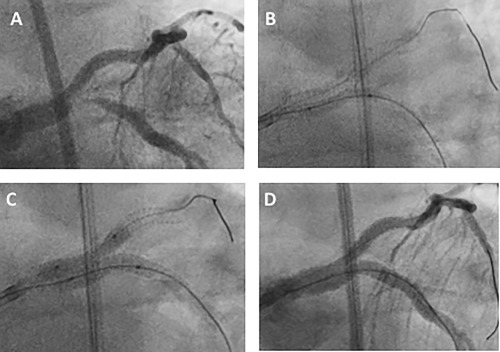
Second example of restenosis in SKS and its treatment with SKS/B (Case 18 in Table 3). A 54‐year‐old man presented in 2015 with crescendo angina and global ST segment depression on the ECG. He was found to have severe disease affecting the bifurcation of the LMS and proximal segments of his major coronary arteries. He underwent successful SKS (3.0 × 38 mm Promus Premier™ and 3.0 × 48 mm Xience™ stents). He represented 27 months later with a month's history of dyspnea on exertion. Repeat coronary angiography demonstrated restenosis at the bifurcation, predominantly affecting the LMS‐Cx limb of the SKS (A), whilst the original stents appeared well deployed. Two wires were passed and predilatation was performed to the lesion with a 2.5 mm balloon at high pressure (B). Simultaneous dilation was then performed with an 3.0 × 18 mm Onyx™ DES in the LMS‐Cx and 3.0 Sequent Please™ DEB to protect the LMS‐LAD. The SKS was then post‐dilated with simultaneous inflation of 3.5 mm noncompliant balloons (C). The final result was excellent (D). Recovery was uneventful and the symptoms were relieved