

Abstract
Background:
Female sexual dysfunction (FSD) and the associated risk factors are less studied in the Middle East. This study is designed to determine the prevalence of FSD and its associated risk factors in Jordan.
Materials and Methods:
A group of women were interviewed using detailed questionnaire on several aspects of FSD including desire, arousal, lubrication, orgasm, satisfaction, and pain disorders. They underwent sociodemographic investigation. Prevalence and risk factors of FSD are calculated in different age groups.
Results:
A total of 470 women aged 32.6 ± 9.6 years are included in this study. Desire problems were detected in 49.4% (232/470) of the studied women, while an arousal problem in 31.9% (150/470) and lubrication problem in 39.2% (184/470). An orgasm problem was detected in 39.57% (186/470) of the studied women, while satisfaction problem was detected in 43.82% (206/470) and pain problem during sexual relation in 19.2% (90/470). There was positive significant correlation between each domain of the FSD and the studied women's age except pain. FSD was found to be significant in women with more than four children (83.3%, P < 0.02), those who had been married for more than 10 years (76.7%, P < 0.02), in women with chronic medical diseases (76.7%, P < 0.02), in unemployed women (76.7%, P < 0.02), and in women not using contraception (75.2%, P < 0.005). There was no significant correlation with the level of education (P < 0.34) and monthly income (P < 0.24).
Conclusion:
The prevalence of FSD in Jordan is about 64.7%, the desire disorders are the most prevalent domain of FSD, and age is the most significant risk factor for FSD. Further research is needed with larger and more comprehensive sample to estimate the magnitude of FSD and to confirm its relationship with different risk factors.
Keywords: Dysfunction, female, Jordan, risk, sexual
Introduction
Female sexual dysfunction (FSD) and the associated risk factors are less studied in the Middle East.[1,2,3,4,5,6]
FSD may be a lifelong problem or acquired later in life after a state of normal sexual functioning. It takes different forms, including lack of sexual desire, impaired arousal, inability to accomplish orgasm, and/or pain during sexual activity.[7]
The sexuality manifestations are complex interactions of behavioral, intrapsychical, social, and interpersonal factors intervening in its initiation and maintenance.[7]
A normal sexual response is usually followed by characteristics of psycho-physiological expressions, and many physical and mental changes.[8]
The sexual response involves the entire body organs, although the most characteristic physiological changes occur in the genitalia. Healthy body is required to have effective and pleasant sexual response. For this reason, different natures of many body disorders may adversely affect the satisfactory sexual response.[9]
The female sexual cycle is first described by Master and Johnson in 1966.[10] It is divided into four phases: desire (libido), arousal (excitement), orgasm, and resolution. Understanding the sexual response cycle will help in the evaluation and management of the related disorders.[9]
No previous studies were conducted in Jordon to estimate the prevalence of FSD and its related risk factors; therefore, this study is designed to determine the prevalence of FSD and its associated risk factors in Jordan.
Materials and Methods
Four hundred seventy Jordanian women who attended King Hussein Medical Center in Amman, Jordan, were recruited in this cross-sectional, descriptive study from September 2017 to January 2018. The study was approved by the ethical committee of the Royal Medical Services, and women were recruited in this study after informed written consent.
Women with severe medical or psychiatric illnesses, divorced, or widowed were excluded from this study. The required data were collected through face-to-face interview with each participant by female doctor or qualified nurse using Arabic translation of female sexual function index (FSFI).[11]
Subjects were divided into six age groups, including ages less than 18, 19–29, 30–39, 40–49, 50–59, and 60–69 years. Demographic characteristics were collected using questionnaire including the following: age of the husband, occupational status, average income, level of education, parity, use of any medications, duration of relationship, contraception use, and the past medical and/or surgical history.
The Arabic translation of FSFI questionnaire was used to evaluate FSD. The FSFI[12] is a brief, 19-item self-report measure of FSD that provides scores on six domains of sexual function as well as a total score. The domains assessed in the questionnaire include the following: desire (2 items), arousal (4 items), lubrication (4 items), orgasm (3 items), satisfaction (3 items), and pain (3 items). The questionnaire assessed sexual function or disorders which had occurred during the past 4 weeks. Sexual desire was assessed by asking two questions about frequency and desire level. Arousal was assessed by asking four questions about frequency, level, confidence, and satisfaction. Lubrication was assessed by asking four questions about frequency, difficulty, frequency of maintaining lubrication, and difficulty in maintaining lubrication. Orgasm was assessed by asking three questions about frequency, difficulty, and satisfaction. Satisfaction was assessed by asking three questions about the amount of closeness with partner, sexual relationship, and overall sex life. Pain was assessed by asking three questions about pain frequency during vaginal penetration and pain frequency following vaginal penetration. Calculation of the prevalence of sexual dysfunction for each domain and comparison among the groups was done. Therefore, sexual dysfunction for each domain was considered when the desire score is ≤3.3 (range 1–5), an arousal score is ≤3.4 (range 0–5), lubrication score is ≤3.4 (range 0–5), an orgasm score is ≤3.4 (range 0–5), satisfaction score is ≤3.8 (range 0–5), and pain score is ≤3.8 (range 0–5). The total score was obtained by adding the six domain scores; the range of the total score was from 2 to 36. Sexual dysfunction was considered when the total score was <28. Interviewers (doctors and qualified nurses) matched respondents on various social attributes in an interview averaging 35 minutes. The collected data were tabulated and statistically analyzed using the Statistical Package for Social Sciences version 20 (Chicago, IL), to determine the prevalence of FSD and to predict the associated risk factors in Jordan.
Mean and standard deviation were used to represent numerical variables, whereas number and percentage were used to represent categorical variables. Independent Student's t-test was used for numeric parametric variables, and Chi-square test used for categorical variables analysis. P < 0.05 was considered statistically significant.
Sample size
The required sample size was calculated using G Power software version 3.17 for sample size calculation (Heinrich-Heine-Universität, Düsseldorf, Germany), setting α-error probability at 0.05, power (1−β error probability) at 0.95%, and effective sample size (w) at 0.3. The effective sample includes more than 110 women needed to produce a statistically acceptable figure.
Results
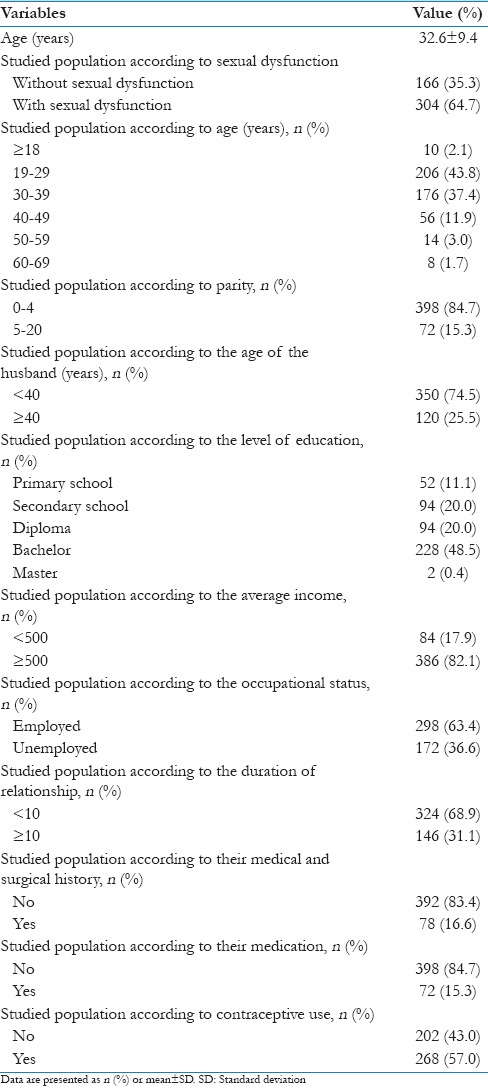
Four hundred seventy Jordanian women were recruited in this study and the sociodemographic data of the studied women were listed in Table 1. The sexual dysfunction was detected in 304 (64.7%) of the studied women [Table 1].
Table 1.
Sociodemographic and marital characteristics of the studied population, and the use of contraceptives
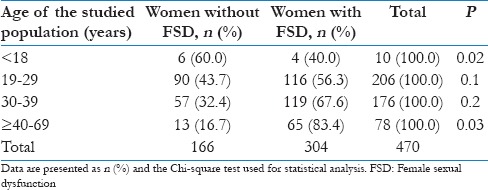
FSD was significantly low in women <18 years (4/304 women with FSD compared to 6/166 women without FSD, P = 0.02) and significantly high in women ≥40–69 years (65/304 with FSD compared to 13/166 women without FSD, P = 0.03; Table 2).
Table 2.
Prevalence of female sexual dysfunction according to the age group of the study participants
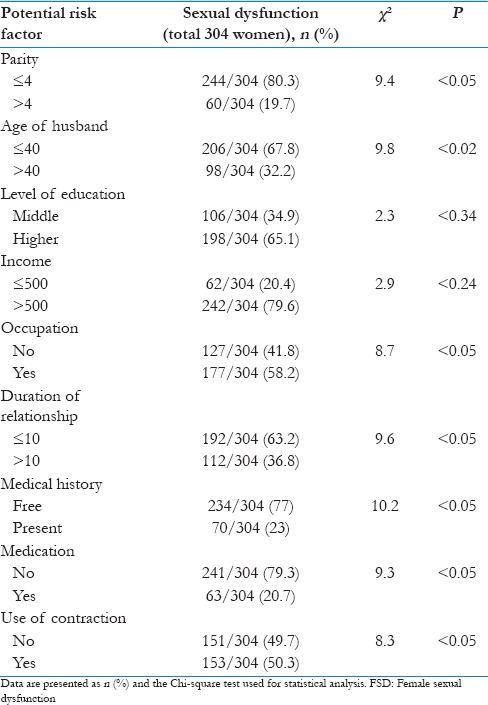
FSD was significantly high in women who had more than 4 children [30 (83.3%), P < 0.02]; their husbands were more than 40 years of age [98 (81.7%), P = 0.002]; had been married for more than 10 years [112 (76.7%), P < 0.02]; were unemployed [127 (76.7%), P < 0.02]; had medical problems such as hypertension, diabetes mellitus, and ischemic heart disease [70 (76.7%), P < 0.02]; used medication [62 (86.1%), P < 0.006]; and did not use contraceptives [151 (75.2%), P < 0.005]. There were no significant correlations between FSD and the level of education (P < 0.34) or monthly income (P < 0.24) [Table 3].
Table 3.
The potential risk factors for female sexual dysfunction
Desire problems were detected in 49.4% (232/470) of the studied women, while an arousal problem was detected in 31.9% (150/470) and lubrication problem in 39.2% (184/470). An orgasm problem was detected in 39.57% (186/470) of the studied women, while the satisfaction problem was detected in 43.82% (206/470) and pain problem during sexual relation in 19.2% (90/470). There was positive significant correlation between each domain of the FSD and the studied women's age except pain [Table 4].
Table 4.
The domain score of each sexual dimension of each studied group

Discussion
This study was conducted to determine the prevalence of FSD and its associated risk factors in Jordan. Sexuality is a crucial issue in enhancing marital relationships. In Jordanian society, like any other Arabic society, talking about sexual disorders is sensitive and may lead to improper assessment.[2]
All studies conducted in the Middle East to assess the sexual disorders are not comprehensive to discuss all the possible risk factors of FSD.[1,2,4]
In this study, we tried to assess the prevalence of FSD and some of its related risk factors using data collected from three different areas in Amman, the capital city of Jordan, where nearly half of the people in Jordan live and represent different socioeconomic levels.
In this study, FSD is recorded in 64.7% of the studied women (age range 18–69 years) which is higher than that reported by Laumann et al.,[3] who reported FSD in 43% of their studied women (1.749 women investigated, living throughout USA).[3]
The prevalence of FSD in a Turkish study conducted by Cayan et al.[4] ranged from 22% in women aged 18–27 years to 66% in those aged 48–57 years. Jaafarpour et al.[13] reported 46.2% prevalence of FSD in an Iranian study.
In this study, the desire problems were detected in 49.4% (232/470) of the studied women, while an arousal problem was detected in 31.9% (150/470) and the lubrication problem in 39.2% (184/470). An orgasm problem was detected in 39.57% (186/470) of the studied women, while the satisfaction problem was detected in 43.82% (206/470) and pain problem during sexual relation in 19.2% (90/470).
Cayan et al.[4] reported desire problems in 60% of their studied women, arousal problems in 43%, lubrication problems in 38%, and orgasmic problems in 46%, which indicate that the results of this study are consistent with what was reported by Cayan et al.[4]
In addition, Castelo-Branco et al.[14] conducted a study on 534 healthy women (52 ± 6 years) to assess FSD, and they reported desire disorders in 38%, arousal disorders in 32%, orgasmic disorders in 25%, and dyspareunia in 33% of the studied women.
Age is the most important factor for FSD[14,15,16,17]; in this study, participants with FSD were significantly older than 50 years of age (100%, P < 0.01), and they all have domains of FSD except dyspareunia which was less in their age group compared to others. This can be explained by the less frequent intercourse and/or sexual relation in their age group compared to other younger age groups.
In this study, there was positive significant correlation between each domain of the FSD and the studied women's age except pain (all domains of the FSD increased with the increased women's age). Levine et al.[16] previously confirmed this correlation in their study.
Parity and duration of marriage have negative correlation with FSD,[2] and this study and other previous studies showed that women with more children had higher sexual disorders.[18,19] Other studies failed to confirm this relationship.[20,21]
Makkii and Yazdi[22] recommended designing valid surveys on large samples to overcome the inconsistency in the results of the effect of parity on FSD.
Chronic diseases such as hypertension, diabetes mellitus, and ischemic heart diseases were generally not strongly correlated to FSD in some studies,[23] while in this research we found significant relationship between FSD and chronic diseases (89.7%, P < 0.001).
In addition, previous studies showed positive association among depression, anxiety, and FSD.[24]
Data regarding the effect of contraception on FSD are conflicting, as there are no randomized controlled trials to compare the effect of different methods of contraception (hormonal and non-hormonal methods) on FSD.
A decrease in sexual interest in women using some birth control methods was reported by a prospective cohort study,[25] which was the largest to address this issue. It compared women who used copper intrauterine device (IUD) with women using other hormonal methods; a decrease in interest was found in women using estrogen–progestin vaginal ring, depot medroxyprogesterone, and progestin implant. There was no effect on sexual interest in women using estrogen–progestin oral contraceptives, progestin IUD, or estrogen–progestin patch. In general, the data of this study showed more sexual dysfunction in those who did not use contraception (75.2%, P < 0.005).
The prevalence of FSD is high in this study and we have to acknowledge the fact that FSD is a problem in our society. We need to have clear pathways to refer these patients for further management. Unfortunately, we do not have sexual therapists in Jordan to treat these patients and some of them are managed by general gynecologists or psychiatrists who are not trained in this difficult area.
This study was conduction in Amman, which is the capital city of Jordan (urban area); no women from rural areas were included in this study, which is one of the limitations of this study. In addition, the questionnaire should be self-administered questionnaires to decrease the bias in the data collected for analysis.
Further research is needed with larger and more comprehensive sample to estimate the magnitude of FSD and to confirm the relationship of FSD with different risk factors.
Conclusion
The prevalence of FSD in Jordan is about 64.7%, the desire disorders are the most prevalent domain of FSD, and age is the most significant risk factor for FSD. Further research is needed with larger and more comprehensive sample to estimate the magnitude of FSD and to confirm its relationship with different risk factors.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors are grateful to all women who agreed to participate in this study.
References
- 1.Oksuz E, Malhan S. Prevalence and risk factors for female sexual dysfunction in Turkish women. J Urol. 2006;175:654–8. doi: 10.1016/S0022-5347(05)00149-7. [DOI] [PubMed] [Google Scholar]
- 2.Abu Ali RM, Al Hajeri RM, Khader YS, Ajlouni KM. Factors associated with sexual dysfunction in Jordanian women and their sexual attitudes. Ann Saudi Med. 2009;29:270–4. doi: 10.4103/0256-4947.55312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Laumann EO, Paik A, Rosen RC. Sexual dysfunction in the United States: Prevalence and predictors. JAMA. 1999;281:537–44. doi: 10.1001/jama.281.6.537. [DOI] [PubMed] [Google Scholar]
- 4.Cayan S, Akbay E, Bozlu M, Canpolat B, Acar D, Ulusoy E, et al. The prevalence of female sexual dysfunction and potential risk factors that may impair sexual function in Turkish women. Urol Int. 2004;72:52–7. doi: 10.1159/000075273. [DOI] [PubMed] [Google Scholar]
- 5.Mostafa AM, Khamis Y, Helmy HK, Arfa AE, Abbas AM. Prevalence and patterns of female sexual dysfunction among overweight and obese premenopausal women in Upper Egypt; a cross sectional study. Middle East Fertil Soc J. 2018;23:68–71. [Google Scholar]
- 6.El-Tahlawi S, Mohammad NE, Yousef NM, Abdelreheem T, Elsayed AY. Female sexual dysfunction in Elfayoum Governorate. Adv Sex Med. 2018;8:1–13. [Google Scholar]
- 7.Dunn KM, Jordan K, Croft PR, Assendelft WJ. Systematic review of sexual problems: Epidemiology and methodology. J Sex Marital Ther. 2002;28:399–422. doi: 10.1080/00926230290001529. [DOI] [PubMed] [Google Scholar]
- 8.Hisasue S, Kumamoto Y, Sato Y, Masumori N, Horita H, Kato R, et al. Prevalence of female sexual dysfunction symptoms and its relationship to quality of life: A Japanese female cohort study. Urology. 2005;65:143–8. doi: 10.1016/j.urology.2004.08.003. [DOI] [PubMed] [Google Scholar]
- 9.Anastasiadis AG, Davis AR, Ghafar MA, Burchardt M, Shabsigh R. The epidemiology and definition of female sexual disorders. World J Urol. 2002;20:74–8. doi: 10.1007/s00345-002-0272-5. [DOI] [PubMed] [Google Scholar]
- 10.Masters WH, Johnson VE. Human Sexual Response. Boston: Ishi Press International; 1966. [Google Scholar]
- 11.Rosen RC, Taylor JF, Leiblum SR, Bachmann GA. Prevalence of sexual dysfunction in women: Results of a survey study of 329 women in an outpatient gynecological clinic. J Sex Marital Ther. 1993;19:171–88. doi: 10.1080/00926239308404902. [DOI] [PubMed] [Google Scholar]
- 12.Rosen R, Brown C, Heiman J, Leiblum S, Meston C, Shabsigh R, et al. The female sexual function index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26:191–208. doi: 10.1080/009262300278597. [DOI] [PubMed] [Google Scholar]
- 13.Jaafarpour M, Khani A, Khajavikhan J, Suhrabi Z. Female sexual dysfunction: Prevalence and risk factors. J Clin Diagn Res. 2013;7:2877–80. doi: 10.7860/JCDR/2013/6813.3822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Castelo-Branco C, Blumel JE, Araya H, Riquelme R, Castro G, Haya J, et al. Prevalence of sexual dysfunction in a cohort of middle-aged women: Influences of menopause and hormone replacement therapy. J Obstet Gynaecol. 2003;23:426–30. doi: 10.1080/0144361031000120978. [DOI] [PubMed] [Google Scholar]
- 15.Dennerstein L, Dudley E, Burger H. Are changes in sexual functioning during midlife due to aging or menopause? Fertil Steril. 2001;76:456–60. doi: 10.1016/s0015-0282(01)01978-1. [DOI] [PubMed] [Google Scholar]
- 16.Levine KB, Williams RE, Hartmann KE. Vulvovaginal atrophy is strongly associated with female sexual dysfunction among sexually active postmenopausal women. Menopause. 2008;15:661–6. doi: 10.1097/gme.0b013e31815a5168. [DOI] [PubMed] [Google Scholar]
- 17.Lou WJ, Chen B, Zhu L, Han SM, Xu T, Lang JH, et al. Prevalence and factors associated with female sexual dysfunction in Beijing, China. Chin Med J (Engl) 2017;130:1389–94. doi: 10.4103/0366-6999.207466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hayes RD, Dennerstein L, Bennett CM, Fairley CK. What is the “true” prevalence of female sexual dysfunctions and does the way we assess these conditions have an impact? J Sex Med. 2008;5:777–87. doi: 10.1111/j.1743-6109.2007.00768.x. [DOI] [PubMed] [Google Scholar]
- 19.Lin MC, Lu MC, Livneh H, Lai NS, Guo HR, Tsai TY, et al. Factors associated with sexual dysfunction in Taiwanese females with rheumatoid arthritis. BMC Womens Health. 2017;17:12. doi: 10.1186/s12905-017-0363-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Graziottin A. Prevalence and evaluation of sexual health problems – HSDD in Europe. J Sex Med. 2007;4(Suppl 3):211–9. doi: 10.1111/j.1743-6109.2007.00447.x. [DOI] [PubMed] [Google Scholar]
- 21.Abidin A, Draman N, Ismail SB, Mustaffa I, Ahmad I. Female sexual dysfunction among overweight and obese women in Kota Bharu, Malaysia. J Taibah Univ Med Sci. 2016;11:159–67. [Google Scholar]
- 22.Makkii M, Yazdi NA. Sexual dysfunction during primiparous and multiparous women following vaginal delivery. Tanzan J Health Res. 2012;14:263–8. [PubMed] [Google Scholar]
- 23.Kadri N, Mchichi Alami KH, Mchakra Tahiri S. Women sexual dysfunction: A population-based epidemiological study. Arch Women Ment Health. 2002;5:59–63. doi: 10.1007/s00737-002-0141-7. [DOI] [PubMed] [Google Scholar]
- 24.Sidi H, Puteh SE, Abdullah N, Midin M. The prevalence of sexual dysfunction and potential risk factors that may impair sexual function in Malaysian women. J Sex Med. 2007;4:311–21. doi: 10.1111/j.1743-6109.2006.00319.x. [DOI] [PubMed] [Google Scholar]
- 25.Boozalis A, Tutlam NT, Chrisman Robbins C, Peipert JF. Sexual desire and hormonal contraception. Obstet Gynecol. 2016;127:563–72. doi: 10.1097/AOG.0000000000001286. [DOI] [PMC free article] [PubMed] [Google Scholar]