
Figure 1. Skin cancer development is associated with areas of active skin inflammation in DLE.
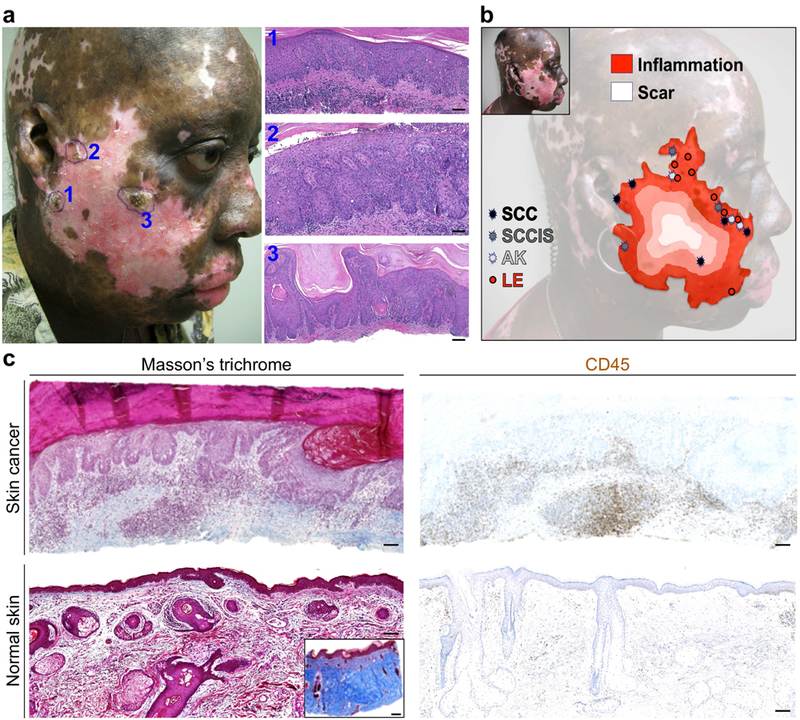
(a) Clinical and pathological images of three independent skin cancers, [1] SCC in situ (SCCIS), [2] SCC and [3] SCCIS, that were diagnosed concurrently at the margins of a depigmented DLE plaque on a patient’s sun-exposed skin are shown. (b) The review of clinical images and pathology reports reveals the locations of neoplastic skin lesions (SCC, SCCIS and AK: actinic keratosis) and active lupus inflammation (LE) that were biopsied to rule out skin cancer during the eight-year follow-up period on the stable DLE plaque. Each lesion is mapped onto a topographic outline of the DLE plaque with the opposite gradients of scarring and inflammation in DLE highlighted in the background. (c) The extent of dermal scarring (Masson’s trichrome stain) and inflammation (CD45 stain) are shown in patient’s skin cancer compared to aged-matched normal facial skin. Note the insert shows positive control for Masson’s trichrome staining in a skin sample with scarring. Cytoplasm and muscle fibers stain red, whereas collagen displays blue coloration; scale bars: 100 µm.