
FIGURE 1.
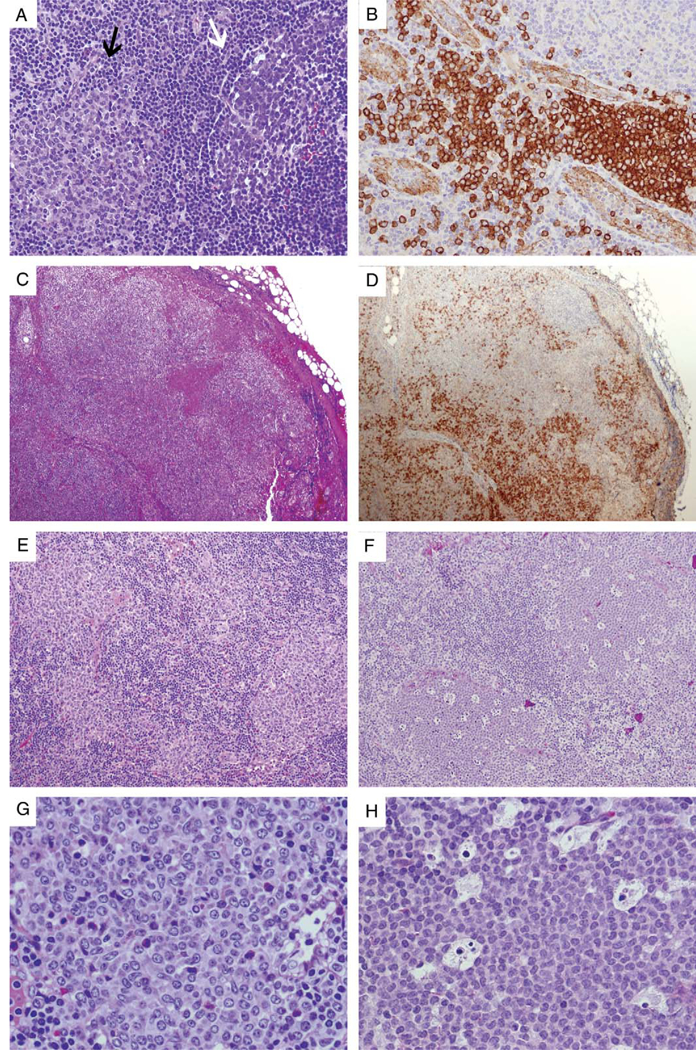
PDCs in reactive and neoplastic conditions. A, In this reactive lymph node, a PDC nodule (left, indicated by a black arrow) is compared with a neighboring germinal center (right, indicated by a white arrow), the latter having a heterogeneous cellular composition and surrounded by a discrete mantle zone. B, PDCs stain strongly positive for CD123 and are most prominent around high endothelial venules, which as a useful internal control are weakly positive for CD123. C (H&E) and D (CD123), Kikuchi-Fujimoto lymphadenopathy, which on H&E may mimic non-Hodgkin lymphoma, is often associated with loose sheets of PDCs (highlighted by CD123 staining), admixed with histiocytes and immunoblasts. E, Clusters of reactive PDCs in an exceptional case of classical Hodgkin lymphoma. F, PDC nodules in a child with juvenile myelomonocytic leukemia; the abundance of apoptotic bodies may result in a low power appearance resembling “naked” germinal centers. G, High-power view of (E) demonstrates intermediate-sized cells with distinct nuclear membranes and pinpoint nucleoli. H, High-power view of (F) demonstrates uniform intermediate-sized cells with finely dispersed chromatin and inconspicuous nucleoli, admixed with numerous apoptotic bodies. H&E indicates hematoxlin and eosin; PDC, Plasmacytoid dendritic cells.