

Abstract
Noninvasive transcranial or minimally invasive transtympanic electric stimulation may offer a desirable treatment option for tinnitus because it can activate the deafferented auditory nerve fibers while posing little to no risk to hearing. Here, we built a flexible research interface to generate and control accurately charge-balanced current stimulation as well as a head-mounted instrument capable of holding a transtympanic electrode steady for hours. We then investigated the short-term effect of a limited set of electric stimulation parameters on tinnitus in 10 adults with chronic tinnitus. The preliminary results showed that 63% of conditions of electric stimulation produced some degree of tinnitus reduction, with total disappearance of tinnitus in six subjects in response to at least one condition. The present study also found significant side effects such as visual, tactile, and even pain sensations during electric stimulation. In addition to masking and residual inhibition, neuroplasticity is likely involved in the observed tinnitus reduction. To translate the present electric stimulation into a safe and effective tinnitus treatment option, we need to optimize stimulation parameters that activate the deafferented auditory nerve fibers and reliably suppress tinnitus, with minimal side effects and tolerable sensations. Noninvasive or minimally invasive electric stimulation can be integrated with sound therapy, invasive cochlear implants, or other forms of coordinated stimulation to provide a systematic strategy for tinnitus treatment or even a cure.
Keywords: transcranial alternating-current stimulation, deafferented auditory nerve fibers, scalp, ear canal, promontory, round window, loudness, residual inhibition
Introduction
Sound therapy is only partially effective in tinnitus treatment because acoustic stimulation cannot activate the deafferented auditory nerve fibers that may be the root cause of tinnitus generation. On the other extreme, cochlear implants directly stimulate the auditory nerve and have been shown to suppress tinnitus, but their invasiveness and risk of permanent damage to acoustic hearing make them unsuitable to most tinnitus sufferers who have significant residual or even normal hearing. Noninvasive transcranial or minimally invasive transtympanic electric stimulation may offer a desirable treatment option because it can activate the detached nerve while posing minimal risk of damaging hearing (Zeng, Djalilian, & Lin, 2015). Although this form of electric stimulation has been used to treat tinnitus for more than 200 years (e.g., Althaus, 1886), no protocols or devices have been widely accepted by the scientific community or clinically approved by the U.S. Food and Drug Administration at present. While other factors are likely involved, the following four factors have significantly contributed to the lack of progress in translating electric stimulation for tinnitus treatment.
First, there is no clear and unified scientific rationale to guide technological development. For example, decreasing spontaneous activity in the auditory nerve was the goal for tinnitus treatment based on a noise-induced tinnitus model (Di Nardo et al., 2009; Mielczarek, Norena, Schlee, & Olszewski, 2018; Norena, Mulders, & Robertson, 2015). In contrast, increasing spontaneous activity in the auditory nerve was the goal for tinnitus treatment in a deafferented cochlear model (Rubinstein, Tyler, Johnson, & Brown, 2003; Rubinstein, Wilson, Finley, & Abbas, 1999). Both theories may be right insofar as they represent different types of tinnitus or reflect different time courses during tinnitus development, but they require divergent technical specifications; for example, direct current (DC: 0 Hz) stimulation for decreasing spontaneous activity and high-frequency (5000 Hz) stimulation for increasing spontaneous activity.
Second, safety is an important concern in electric stimulation for tinnitus. Several human studies used either ear canal or transcranial DC electric stimulation for tinnitus treatment (Althaus, 1886; Joos, De Ridder, Van de Heyning, & Vanneste, 2014; Mielczarek et al., 2018; Shekhawat et al., 2016). Although these studies showed significant tinnitus reduction, concerns about the long-term safety of charge-imbalanced DC stimulation have prevented its clinical application, especially in patients with significant residual or normal hearing (Aran, Wu, Charlet de Sauvage, Cazals, & Portmann, 1983; Dauman, 2000; Huang, Shepherd, Carter, Seligman, & Tabor, 1999).
Third, electric stimulation is not optimized to achieve the greatest efficacy for tinnitus treatment. For example, charge-balanced alternating-current stimulation is safe and has been shown to suppress tinnitus in about 50% of patients (Hazell, Jastreboff, Meerton, & Conway, 1993; Kuk, Tyler, Rustad, Harker, & Tye-Murray, 1989; Perez et al., 2015; Rubinstein et al., 2003; Shulman, Tonndorf, & Goldstein, 1985; Vernon & Fenwick, 1985). However, these previous studies showed a wide range of stimulus parameters used for tinnitus suppression, with occasionally contradictory suggestions. Hazell et al. (1993) favored low frequencies (<100 Hz), Rubinstein et al. (2003) advocated for a high-frequency (4800 Hz) pulse train, while Shulman et al. (1985) used amplitude-modulated sinusoids. The level of stimulation ranged from below audibility threshold (Shulman et al., 1985) to a 2-mA hardware limit (Perez et al., 2015). The duration of stimulation ranged from minutes (Rubinstein et al., 2003) to days (Shulman et al., 1985). Although alternating-current stimulation is safe, its clinical application requires a narrowing of this parameter space toward optimized stimulation strategies.
Finally, practicality is a significant limiting factor. There is not a single electric stimulator that is specifically designed and commercially available to meet the need for tinnitus treatment. Previous studies either used stimulators for pain management (e.g., Vernon & Fenwick, 1985) or customized equipment for research purposes only (e.g., Hazell et al., 1993; Shulman et al., 1985). In addition, stable electrode contact is difficult with either tympanic or transtympanic stimulation (e.g., Kuk et al., 1989; Perez et al., 2015). Although commercially available cochlear implants have been modified for tinnitus treatment (Hazell et al., 1993; Rubinstein et al., 2003; Wenzel et al., 2015), the invasive nature and the likelihood of damaging hearing limit their clinical utility because, after all, most tinnitus sufferers have significant residual or even normal hearing.
The long-term goal of the present study is to identify safe and effective modes of electric stimulation and to develop a commercially viable medical device for tinnitus treatment. The short-term goal is to explore both noninvasive and minimally invasive electric stimulation for tinnitus treatment, with a focus on experimental design and feasibility. The scientific premise is based on the deafferentation tinnitus model (Roberts et al., 2010; Schaette & McAlpine, 2011; Weisz, Hartmann, Dohrmann, Schlee, & Norena, 2006), in which detached auditory nerve fibers cannot be activated by acoustic stimulation but only by electric stimulation. The practical consideration is that non- and minimally invasive electric stimulation provides a natural bridge between sound therapy and cochlear implants or other forms of invasive electric stimulation.
Methods
Subjects
A total of 10 adults who had chronic tinnitus (≥6 months) participated in the present study. All subjects provided informed consent for their participation, following a human subject protocol approved by the institutional review board of the University of California, Irvine. The study is currently registered as a human clinical trial with the U.S. Food and Drug Administration (NCT03511807). Table 1 displays demographic information for these tinnitus subjects.
Table 1.
Tinnitus Subject Information.
| Subject | Age (Years) | Gender | Audiogram | Tinnitus | Severity | Match |
|---|---|---|---|---|---|---|
| T1 | 48 | Female | Deaf in RE, residual hearing (<1000 Hz) in LE | Bilateral (RE > LE), multitonal | 44* | NA |
| T2 | 56 | Male | Normal hearing | Unilateral (RE), tonal | NA | 700-Hz tone |
| T3 | 67 | Male | Symmetrical, sloping hearing loss | Bilateral, tonal | 67* | 11,530-Hz tone |
| T4 | 67 | Female | Symmetrical, sloping hearing loss | Bilateral (RE > LE), tonal | 12 | 5686-Hz tone |
| T5 | 71 | Male | Symmetrical, sloping hearing loss | Bilateral (RE < LE), noisy | 44 | 9038–9845-Hz noise |
| T6 | 51 | Male | Symmetrical, mild sloping loss | Unilateral (LE), tonal | 12 | 6042-Hz tone |
| T7 | 58 | Male | Severe flat loss in RE, sloping loss in LE | Unilateral (RE), tonal | 74 | 12,000-Hz tone |
| T8 | 49 | Male | Sloping loss in RE (otosclerosis), normal in LE | Unilateral (RE), tonal | 86 | 2500-Hz tone |
| T9 | 55 | Female | Sloping loss in RE, deaf in LE | Unilateral (LE), Tonal + Musical | 84 | 1230-Hz tone |
| T10 | 70 | Female | Flat severe loss in RE, sloping loss in LE | Unilateral (RE), tonal | 56 | 1429-Hz tone |
Note. Severity was measured using either Tinnitus Functional Index (*) or Tinnitus Severity Index, with a scale from 0 indicating no tinnitus to 100 indicating the most severe tinnitus. T1 described three components in her tinnitus: (a) a high-pitched component that was always present, (b) a pulsing mid tone, and (c) a continuous low tone that was sometimes on and sometimes off. She could not perform tinnitus match because of hearing loss in both ears. T8 had previously unilateral mixed sloping hearing loss in the right ear and a history of right-sided tinnitus, which did not improve despite a successful right-sided stapedotomy with complete air-bone closure. T9 matched the dominant tonal component of her tinnitus in the deafened left ear to a 1230-Hz pure tone in the right ear. She also reported a second musical component in her tinnitus that sounded like a musical instrument without lyrics. Five subjects with the most severe degrees of tinnitus (T3, T7–T10) participated in the minimally invasive electric stimulation study.
RE = right ear; LE = left ear.
Stimuli
Noninvasive electric stimulation
Figure 1 shows a block diagram of the custom-made research interface for electric stimulus generation and control. A personal computer generated digital stimuli and controlled timing of stimulation. A sound card converted the digital signal into an analog signal. A current source converted the analog voltage stimulus into a constant current stimulus (Vurek, White, Fong, & Walsh, 1981). Either the experimenter or the subject could terminate electric stimulation by releasing a foot pedal connected to a safety switch. A transformer power supply (red circle and red lines) was used to isolate the subject from direct connection to the power line. An oscilloscope (green box and green line) was used to calibrate the equipment and monitor voltage delivered to the electrodes in real-time throughout the entire experiment. During calibration, before actual connection to the subject, a 1000-Ω resistor was connected to the output of the current source to ensure that the maximal output of the entire setup was exactly 2 mA and, under no circumstance, the current exceeded 2 mA. The 1000-Ω resistor was disconnected during the actual test session.
Figure 1.

The research interface for electric stimulation. The right panel shows a setup for noninvasive electric stimulation, in which a gold-plated tiptrode is inserted in the ear canal and a plate electrode is placed on the mastoid.
Electric stimulation was delivered to two electrodes, which could be a combination of the following three electrodes types, (a) silver chloride 2.3 × 3 cm plate (Natus Medical Inc., Pleasanton, CA), (b) gold cup (Natus Neurology-Grass, Warwick, RI), and (c) gold foil-wrapped-foam tiptrode (Etymotic ER3-26A, Elk Grove Village, IL). The example in the right panel of Figure 1 shows that electric stimulation was delivered to a gold-plated tiptrode inserted in the right ear canal and a plate electrode placed on the right mastoid. The stimulus was either a sinusoid or charge-balanced bi-phasic pulse train. The stimulus level varied from 0 to 2 mA or the maximal current that produced uncomfortable loudness or other sensations. The stimulus frequency varied from 10 to 10,000 Hz. The stimulus duration was 500 ms for initial psychophysical testing, namely finding threshold and uncomfortable loudness levels.
The psychophysical result was used to decide stimulus parameters for the tinnitus suppression experiment. If possible, the stimulus current was set individually to a level that was slightly softer than the tinnitus loudness; otherwise a 2-mA maximal level was used if the auditory percept was much softer than the tinnitus loudness or was even absent. Under no circumstance, did the stimulus current produce uncomfortable loudness or intolerable nonauditory side effects. The stimulus frequency included a 100-Hz low frequency, a mid frequency (300, 500, or 700 Hz), and a 5000-Hz high frequency. These frequencies were not matched to tinnitus pitch. Following previous tinnitus suppression protocols (Neff et al., 2017; Reavis et al., 2012; Tyler, Stocking, Secor, & Slattery, 2014), the present stimulus duration was 2 to 3 min in most test sessions, or up to 10 min if there was sufficient time in the test session. The intersession interval was 3 min or as long as needed until tinnitus returned to the baseline. In cases of extended residual inhibition longer than 30 min, the subject was released and instructed to report when tinnitus returned to the baseline. Stimulation was delivered to one of the following three sites, including (a) the tinnitus ear in unilateral cases, (b) the ear with more severe tinnitus in bilateral cases, or (c) both ears in bilateral cases by placing a tiptrode in each of the two ear canals (T1, T4, and T5).
Minimally invasive electric stimulation
Except for placing a ball electrode on the promontory or round window, the minimally invasive electric stimulation had an identical setup as the noninvasive stimulation. Due to time constraints, only 100- or 1000-Hz stimulation was used for tinnitus suppression. Stimulus duration varied from 3 to 10 min depending on time availability. Figure 2(a) shows the experimental setup, where a subject sat comfortably in a reclining patient exam chair. Note the pedal connected to the safety switch underneath the subject’s left foot. Figure 2(b) shows a 1.5-mm myringotomy made in the tympanic membrane over the round window niche. The myringotomy was performed under local anesthesia by applying a thin film of phenol (Apdyne Inc., Denver, CO) to the posterior-inferior quadrant of the tympanic membrane. A platinum-iridium ball electrode (diameter = 0.5 mm) was slightly bent to access the promontory or round window (Medtronic Yingling Flex Tip electrode REF8225251, Minneapolis, MN). The Medtronic electrode contained a flexible platinum-iridium wire that was fully insulated up to the ball tip to prevent current shunting. Figure 2(c) shows a customized head-mounted electrode holder that was modified from over-the-head or circumaural headphones and was used to keep the electrode steady and in close contact with the stimulation site during the experiment. The head-mounted electrode holder was placed on the subject, and the position, tension, and angle of the electrode holder was adjusted for comfort and access to the tympanic membrane, specifically the tympanostomy over the round window area. A 5-mm ear speculum (Welch Allyn Cat. No.52135, Skaneateles Falls, NY) was inserted into the ear canal and stabilized with hearing aid impression material (Audiologist’s Choice Cat. No.01602, Chesterfield, MO) being applied to the concha and the cartilaginous part of the external ear canal around the speculum. The bent ball electrode was carefully placed through the tympanostomy and onto the promontory or round window membrane. In the round window case, the surgeon first identified the round window niche in the posterior-inferior quadrant of the tympanic membrane, then the tectulum or the round window overhang, and finally placed the electrode on the round window membrane under the tectulum with the aid of a microscope. Contact with the round window membrane was further confirmed by decreased and stable electrode impedance on the monitoring oscilloscope. At the end of the experiment, all materials were carefully removed by first pulling the electrode out of the middle ear, then disengaging the clamp holding the electrode to remove the electrode from the ear canal, and taking off the headphones. The impression material and speculum were removed afterwards. The tympanic membrane was patched using a standard technique of paper patch myringoplasty. Placement of a myringotomy in the office is a routine part of neurotology practice and is considered minimally invasive compared with other invasive operative procedures such as full middle ear exploration or cochlear implantation. None of the five subjects who underwent this minimally invasive protocol reported any adverse events or complications during and after the experiment. The tympanic membranes healed in all five subjects who had myringotomy.
Figure 2.

(a) The minimally invasive electric stimulation setup, where a subject is positioned in a reclining patient exam chair with her right ear being stimulated and her left foot stepping on a safety switch. (b) A myringotomy (arrow) allowing an electrode to pass through the tympanic membrane; the umbo is labeled (asterisk). (c) A custom-made head-mounted electrode holder that holds the electrode and also shows the speculum and impression materials.
Procedures
Before each test session, the subject was reminded that he or she could terminate electric stimulation at any time during the experiment by releasing the foot pedal connected to the safety switch. The subject first reported the baseline tinnitus loudness on a 0 to 10 scale, with 0 representing no tinnitus and 10 representing uncomfortable loudness. To study tinnitus suppression, the electric stimulus level was set at a loudness level that was 0 to 2 units below the tinnitus loudness (Reavis et al., 2012), or the setup’s maximal level of 2 mA if the stimulus could not produce such a loudness level. The subject reported loudness estimates of both tinnitus and the stimulus at the onset of electric stimulation and every 30 s after that until the end of stimulation (Tang, Liu, & Zeng, 2006). The subject continued to report tinnitus loudness at the offset of stimulation and every 30 s after that until tinnitus returned the baseline level. In situations where residual inhibition lasted longer than minutes or even hours, the subject was instructed to report via phone or e-mail the time when his or her tinnitus returned to the baseline level.
Results
Noninvasive Electric Stimulation (100 Hz)
Figure 3 shows the effect of 100-Hz sinusoidal electric stimulation on both stimulus and tinnitus loudness over a 2- to 5-min duration in four subjects and six conditions. Except for one condition in T4 (bottom-left panel) where cup electrodes were placed between left and right temple, all other conditions used at least one tiptrode inserted in the ear canal. First, note loudness responses to electric stimulation (blue triangles). Except for T1 who experienced a slight increase in loudness from 3 to 4 during electric stimulation, all other subjects experienced loudness adaptation, or total adaptation without even noticing stimulus offset (T3 and T4). Second, note the effect of electric stimulation on tinnitus (red circles). Two subjects (T1 and T3) reported no effect of electric stimulation on tinnitus. T2 experienced slight tinnitus suppression during a short period of electric stimulation but total tinnitus disappearance after stimulation (i.e., residual inhibition). In two electrode configurations (bottom-left panel and T4 bottom-middle panel), T4 experienced slight reduction in tinnitus loudness (1–2 units) during and after electric stimulation. In the third condition applying tiptrodes to both ear canals (bottom-right panel), T4 experienced the most ideal result using electric stimulation to treat tinnitus: Both tinnitus and stimulus totally disappeared 1 to 3 min after the stimulation onset, with tinnitus being totally suppressed during the remaining period of stimulation and even after stimulation (i.e., residual inhibition).
Figure 3.

Effect of low-frequency electric stimulation on stimulus and tinnitus perception in six conditions (panels) from four subjects (T1–T4). Perceived loudness (y axis) is plotted as a function of time (x axis) for both tinnitus (red circles connected by the solid red line) and stimulus (blue triangles connected by the dotted blue line). Cz indicates the top of the head location.
RE = right ear; LE = left ear.
Noninvasive Electric Stimulation (300–700 Hz)
Figure 4 shows the effect of mid-frequency sinusoidal electric stimulation on both stimulus and tinnitus loudness over a time period of 2 to 5 min in four subjects. The subjects experienced either stimulus loudness adaptation (T1, T4, and T5) or no adaptation (T3), with nobody reporting loudness enhancement. Except for a slight rebound (T1) and inhibition (T5) at the stimulation offset, the mid-frequency electric stimulation had no effect on tinnitus.
Figure 4.

Effect of mid-frequency electric stimulation on stimulus and tinnitus perception in four subjects. T1 (top-left) and T4 (bottom-left) used 500-Hz sinusoidal stimulation, whereas T3 (top-right) used 700-Hz and T5 (bottom-right) used 300-Hz electric stimulation. Perceived loudness (y axis) is plotted as a function of time (x axis) for both tinnitus (red circles connected by the solid red line) and stimulus (blue triangles connected by the dotted blue line). Cz indicates the top of the head location.
RE = right ear; LE = left ear.
Noninvasive Electric Stimulation (5000 Hz)
Figure 5 shows the effect of 5000-Hz sinusoidal electric stimulation on both stimulus and tinnitus loudness over a 2 -or 3-min duration in four subjects. The subjects heard either a faint sound (T1) or nothing (T4–T6) during the 5000-Hz electric stimulation. In terms of its effect on tinnitus, two subjects (T1 and T5) reported no change in tinnitus, one subject (T4) reported slight decrease in tinnitus loudness (from 3 to 2.5), while the remaining subject (T6) experienced a significant decrease in tinnitus loudness (from 4.5 to 0.5) with residual inhibition lasting for another 3 min.
Figure 5.

Effect of high-frequency electric stimulation on stimulus and tinnitus perception in four subjects. Perceived loudness (y axis) is plotted as a function of time (x axis) for both tinnitus (red circles connected by the solid red line) and stimulus (blue triangles connected by the dotted blue line).
RE = right ear; LE = left ear.
Minimally Invasive Electric Stimulation
Figure 6 shows the effect of minimally invasive electric stimulation on both stimulus and tinnitus loudness in four subjects with unilateral hearing loss (T7–T10) and one subject with symmetrical sloping loss (T3). In T7, promontory electric stimulation did not produce any stimulus sensation or any change in tinnitus loudness, except for a slight decrease after the stimulus offset. However, T7 reported that electric stimulation made his tinnitus “less annoying and irritating.” In the remaining four subjects (T8–10 and T3), round window stimulation was applied. T8 experienced total stimulus loudness adaptation 1.5 min after stimulus onset, and, at the same time, reported a slight decrease in tinnitus loudness, which quickly recovered to its usual value during the adaptation period of the stimulus and after electric stimulation. T9 did not show any stimulus loudness adaptation but reported total suppression of his tonal tinnitus component during the entire period of electric stimulation. However, this total suppression was likely a result of simultaneous auditory masking for three reasons. First, T9 matched the pitch of her tonal tinnitus to a pure tone of 1230 Hz, which was close to 1000 Hz of the electric stimulus frequency. Second, tinnitus loudness not only dropped to zero immediately at the stimulation onset but also recovered to its usual value immediately at the stimulation offset. Third, T9 reported that the 1000-Hz electric stimulation had no effect on the musical tinnitus component, which had a loudness rating of 4. T10 experienced the most ideal outcome. The electric stimulus totally adapted 2 min after the stimulation onset. The tinnitus loudness was zero during the first 2 min of stimulation, rebounded to half of its usual value at the moment of total stimulus adaptation, and gradually reduced to zero at the end of stimulation and afterwards. In addition, T10 reported 5 h of residual inhibition in response to 10-min round window electric stimulation. T3, the symmetrically impaired subject who did not experience any tinnitus reduction with noninvasive electric stimulation (Figures 3 and 4), reported significant tinnitus reduction in response to round window stimulation. Different from T10, T3 did not adapt to electric stimulation. Similar to T10, T3 reported gradual suppression of tinnitus during electric stimulation and total residual inhibition of tinnitus after electric stimulation. Surprisingly, much longer than T10’s 5-h residual inhibition, T3’s total residual inhibition lasted 20 h in response to 3-min round window stimulation.
Figure 6.

Effect of promontory (T7) and round window (T8–T10) electric stimulation on stimulus and tinnitus perception. Perceived loudness (y axis) is plotted as a function of time (x axis) for both tinnitus (red circles connected by the solid red line) and stimulus (blue triangles connected by the dotted blue line).
Discussion
For a total of 19 conditions in 10 tinnitus subjects (Figures 3 to 6), 12 conditions or 63% produced some degree of tinnitus reduction, 6 or 32% had no effect on tinnitus, and 1 or 5% increased tinnitus (T4 in Figure 4). Here, we discuss the limitations of the present study, stimulation parameter and side-effect issues, potential mechanisms, and application of a systematic strategy for tinnitus treatment.
Limitations of the Present Study
The present study focused on the experimental design and feasibility of electric stimulation for tinnitus treatment but contained several significant limitations. The first limitation was the small sample size with 10 tinnitus subjects. The sample size limitation shall be overcome with increased subject enrollment as the present study continues. The second limitation was significant tinnitus heterogeneity, including subjects with unilateral or bilateral tinnitus, tonal or nontonal tinnitus, as well as normal hearing or hearing loss. The heterogeneity limitation may become a strength if we can relate tinnitus suppression efficacy to tinnitus type, hearing loss, and parameters of electric stimulation. Except for differential treatments applied to special tinnitus types such as pulsatile or somatic tinnitus (Henry, Zaugg, Myers, Kendall, & Michaelides, 2010; Landgrebe et al., 2010; Marks et al., 2018), there is little evidence for relating different treatments to different tinnitus laterality and tonality. The third limitation was nonsystematic testing of a large parametric space, depending on the subject’s interest and availability in the study as well as the study’s overall time and resource constraints. Although it is harder to overcome the third limitation than the first two, several strategies are laid out in the following section.
Large Parametric Space
The large parametric space includes electrode placement, electrode type, stimulus frequency, level, and duration. To systematically explore this large space, we needed to use five electrode placement sites (Mastoid, temple, ear canal, forehead, and top of the head), four electrode types (plate, cup, tiptrode, and ball), three frequencies (low, mid, and high), three levels (subthreshold, soft, and comfortable), and two durations (short and long). This combination would result in a total of 360 conditions (5 × 4 × 3 × 3 × 2) for a single subject. This large parametric space becomes even larger if additional electrode placement sites such as promontory and round window or additional stimuli such as amplitude-modulated waveforms are used to optimally suppress tinnitus. Although a literature search (PubMed with tinnitus and electric stimulation as key words on June 28, 2018) found 300 previous studies, none had systematically explored this large parametric space. Moving forward, we have to reduce the size of this parametric space with either empirical evidence or theoretical support. For example, the present preliminary data suggest the use of two frequencies at 100 and 5000 Hz (Figures 3 to 5). The present preliminary data are also in line with previous studies in favoring round window over promontory stimulation (e.g., Aran & Cazals, 1981). Theoretically, we need to identify electrical parameters that selectively activate the deafferented auditory nerve fibers.
Side Effects
There were significant and widespread side effects associated with electric stimulation. In the present study, electric stimulation evoked tactile sensation ranging from tingling and vibration to prick or even pain in all 10 subjects tested here. In some subjects, electric stimulation also evoked visual sensation, such as white flickers, and vestibular responses, and muscle activation (Zeng et al., 2018). In one particular case, T8 who had otosclerosis and received a stapes prosthesis, electric stimulation not only produced tingling and stinging sensations on the dermal electrode sites (i.e., ear canal and forehead), but also similar sensations on nonelectrode sites including the back of the head, back of the throat, and the ipsilateral side of the tongue, plus muscular contraction of the mid- and upper face. These sensations and movements are likely a result of activation of other cranial nerves such as the VII (facial), IX (glossopharyngeal), and XII (hypoglossal) nerves via low-impedance pathways associated with the more vascular bone and possibly large perforations in otosclerosis (Mens, Oostendorp, & van den Broek, 1994). All of the presently observed side effects were directly related to electric stimulation because they were not present before stimulation and immediately disappeared after stimulation. Surprisingly, most previous studies ignored these side effects. For example, a similar transcutaneous electric stimulation study showed tinnitus reduction in 53% of 500 tinnitus subjects but did not report any of the currently observed side effects except for allergic reaction to gold-plated electrodes in two subjects (Steenerson & Cronin, 2003). Another study using a slightly different protocol with a silver electrode immersed inside a saline filled ear canal and a return electrode on the forehead reported pain sensation in 51% of 49 tinnitus subjects and 41% of 34 normal controls (Mielczarek et al., 2018). In a more severe case, off-label use of transcutaneous vagus nerve stimulation even produced temporary hearing loss (Early & Stankovic, 2018). To provide safe and effective treatment, we need to study all side effects systematically and optimize electric stimulation that minimizes the side effects.
Potential Mechanisms
Six subjects experienced total tinnitus reduction (T2 and T4 using the tiptrode-tiptrode stimulation in Figure 3; T6 in Figure 5; T9, T10, and T3 in Figure 6). In T2’s case, the total reduction was due to residual inhibition likely as a result of forward suppression of spontaneous firing in auditory neurons (Galazyuk, Voytenko, & Longenecker, 2017). In T9’s case, the total reduction was likely a result of masking because tinnitus dropped to zero immediately after the stimulus onset and recovered to its normal level immediately after the stimulus offset. In the four other cases, the total reduction was likely due to a central neural mechanism because tinnitus suppression not only took time to occur but also took time to disappear (e.g., Hazell et al., 1993; Osaki et al., 2005). A neural mechanism underlying tinnitus suppression also received support from continuous monitoring of the stimulus waveform throughout the experiment. Figure 7 shows identical stimulus waveforms (low panels) between the onset and the offset of the 10-min electric stimulation, suggesting that perceptual changes in both loudness adaptation and tinnitus suppression (upper panel, the same data as T10 in Figure 6) are unrelated to any changes in physical stimulation but rather related to central changes in the nervous system. One possible mechanism is direct stimulus-induced neuroplasticity (e.g., Jackson, Mavoori, & Fetz, 2006; Weisz et al., 2007; Zeng et al., 2011) while another possible mechanism is indirect neuromodulation via vagus nerve stimulation (e.g., Engineer et al., 2011; Kreuzer et al., 2014; Suk, Kim, Chang, & Lee, 2018). At present we do not know the exact mechanisms, nor do we know whether the presently observed short-term tinnitus suppression can translate into a long-term tinnitus therapy. The present study is valuable in terms of its ability to provide immediate, albeit temporary, relief to those who suffer chronic and constant tinnitus.
Figure 7.
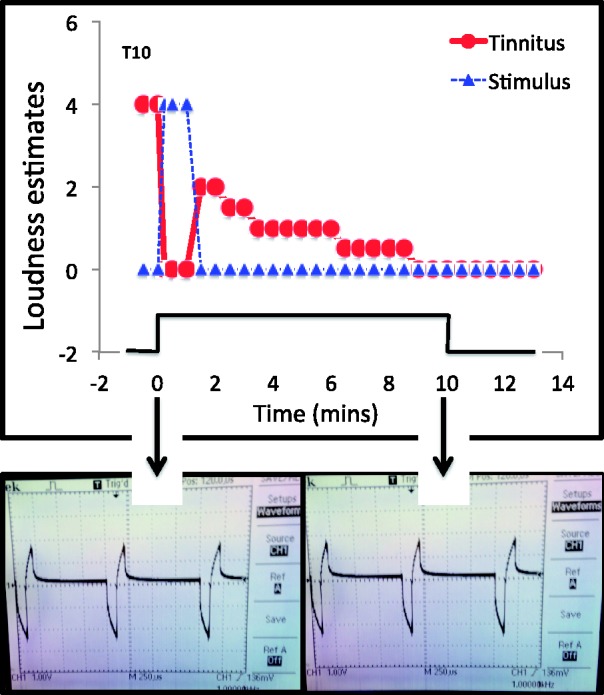
Loudness of tinnitus (red) and stimulus (blue) as a function of 10-min electric stimulation on round window (upper panel). Stimulus waveform at the onset (bottom-left panel) and the offset (bottom-right panel) of the electric stimulus.
A Systematic Treatment Strategy
Given the various degrees of hearing loss in tinnitus sufferers and the equally various degrees of effectiveness in tinnitus therapy, it is critical to develop a systematic approach to tinnitus treatment. To illustrate this point, we found that T5, who was not responsive to either mid- or high-frequency electric stimulation (Figures 4 and 5), actually responded effectively to pitch-matched sound stimulation (Reavis et al., 2012). T3 was another example of the need for a systematic treatment strategy, where the noninvasive electric stimulation was totally ineffective (Figures 3 and 6) but the minimally invasive stimulation produced not only immediate tinnitus suppression but also prolonged residual inhibition (Figure 6). Figure 8 shows a potential treatment strategy that takes both hearing loss and tinnitus therapy effectiveness into account.
Figure 8.
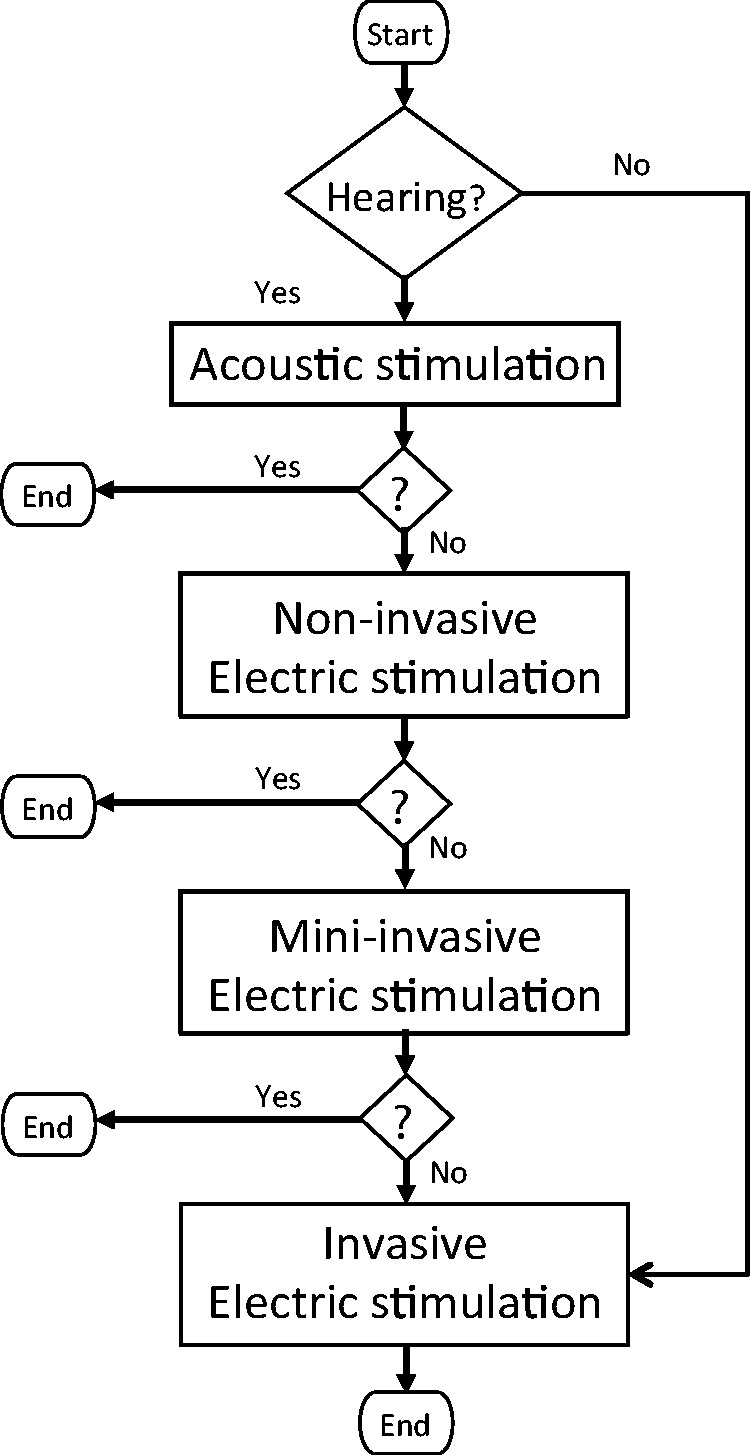
A future tinnitus treatment strategy that analyses a tinnitus sufferer’s hearing status and uses progressively more invasive stimulation dependent upon his or her response to the stimulation.
We envision that in the future, a tinnitus sufferer starts with hearing evaluation in this systematic protocol. If there is no functional hearing, then the person will go straight to the “invasive electric stimulation” intervention such as a cochlear implant to treat both deafness and tinnitus. If there is significant hearing, then the person will first try sound therapy or “acoustic stimulation” to evaluate its effectiveness. The person stays and ends with sound therapy if is effective, but if it is not, then he or she will try “noninvasive electric stimulation” by placing electrodes on the scalp or in the ear canal or the eardrum. Similarly, the person stays and ends with the noninvasive electric stimulation if it is effective, but if it is not, he or she will try “minimally invasive electric stimulation” by making a small myringotomy and placing an electrode on the promontory or round window. The person stays and ends with the minimally invasive electric stimulation if it is effective, but if it is still not, then he or she may consider invasive electric stimulation from cochlear implantation to vagus nerve or deep brain stimulation for the purpose of treating tinnitus. If a tinnitus sufferer indeed ends here, he or she needs to consider the balance between the benefit of tinnitus relief and the risk of surgery or losing hearing. At present, cochlear implantation is not applicable to tinnitus sufferers with normal hearing. The present strategy can be combined with other forms of treatment such as cognitive training and coordinated stimulation to produce a long-lasting effect and eventually find a cure for tinnitus (Cima et al., 2012; Engineer et al., 2011; Gloeckner, Smith, Markovitz, & Lim, 2013; Marks et al., 2018; Tass, Adamchic, Freund, von Stackelberg, & Hauptmann, 2012).
Conclusions
The present study investigated the short-term effect of a limited set of electric stimulation parameters on tinnitus in 10 adults with various types of chronic tinnitus. Six subjects showed nearly 100% tinnitus reduction in response to 2- to 10-min electric stimulation. However, the large electric stimulation parameter space was not systematically explored and significant side effects such as tactile or even pain sensations were encountered during electric stimulation. The present data were exploratory but suggested the need for customized stimulation for each individual tinnitus sufferer. The total and prolonged tinnitus suppression in two subjects (T3 and T10) further suggested that round window stimulation be further explored as a potential long-term solution. Stimulation optimization is required to translate electric stimulation into safe and effective treatment for tinnitus.
Acknowledgments
The authors thank S. George, T. Lu, S. Sun, K. Turner, and Y. Xu for assistance with data collection and all subjects for their spirited and cooperative participation in the present study. The authors also thank Dr. Marzena Mielczarek, Dr. Marlies Knipper, and an anonymous reviewer for their helpful comments on the manuscript. This work was reported at the Tinnitus Research Initiative Meeting, March 14 to 16, 2018 in Regensburg, Germany.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by National Institute on Deafness and Other Communication Disorders (NIH 5R01 DC015587).
References
- Althaus J. (1886) On tinnitus aurium and its treatment by electricity. Lancet 128(3283): 205–206. 10.1016/S0140-6736(00)49789-8. [DOI] [Google Scholar]
- Aran J. M., Cazals Y. (1981) Electrical suppression of tinnitus. Ciba Foundation Symposium 85: 217–231. [DOI] [PubMed] [Google Scholar]
- Aran J. M., Wu Z. Y., Charlet de Sauvage R., Cazals Y., Portmann M. (1983) Electrical stimulation of the ear: Experimental studies. Annals of Otology, Rhinology, and Laryngology 92(6 Pt 1): 614–620. doi: 10.1177/000348948309200616. [DOI] [PubMed] [Google Scholar]
- Cima R. F., Maes I. H., Joore M. A., Scheyen D. J., El Refaie A., Baguley D. M., Vlaeyen J. W. (2012) Specialised treatment based on cognitive behaviour therapy versus usual care for tinnitus: A randomised controlled trial. Lancet 379(9830): 1951–1959. doi:10.1016/S0140-6736(12)60469-3. [DOI] [PubMed] [Google Scholar]
- Dauman N. (2000) Electrical stimulation for tinnitus suppression. In: Tyler R. S. (ed) Tinnitus handbook, San Diego, CA: Singular, pp. 377–398. [Google Scholar]
- Di Nardo W., Cianfrone F., Scorpecci A., Cantore I., Giannantonio S., Paludetti G. (2009) Transtympanic electrical stimulation for immediate and long-term tinnitus suppression. International Tinnitus Journal 15(1): 100–106. [PubMed] [Google Scholar]
- Early S., Stankovic K. M. (2018) Reversible sensorineural hearing loss associated with off-label use of transcutaneous vagal nerve stimulator. Otolaryngology—Head and Neck Surgery 159(4): 802–804. doi:10.1177/0194599818788544. [DOI] [PubMed] [Google Scholar]
- Engineer N. D., Riley J. R., Seale J. D., Vrana W. A., Shetake J. A., Sudanagunta S. P., Kilgard M. P. (2011) Reversing pathological neural activity using targeted plasticity. Nature 470(7332): 101–104. doi:10.1038/nature09656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galazyuk A. V., Voytenko S. V., Longenecker R. J. (2017) Long-Lasting forward suppression of spontaneous firing in auditory neurons: Implication to the residual inhibition of tinnitus. Journal of the Association for Research in Otolaryngology 18(2): 343–353. doi:10.1007/s10162-016-0601-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gloeckner C. D., Smith B. T., Markovitz C. D., Lim H. H. (2013) A new concept for noninvasive tinnitus treatment utilizing multimodal pathways. Conference Proceedings of IEEE Engineering in Medicine and Biology Society 2013: 3122–3125. doi:10.1109/EMBC.2013.6610202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hazell J. W., Jastreboff P. J., Meerton L. E., Conway M. J. (1993) Electrical tinnitus suppression: Frequency dependence of effects. Audiology 32(1): 68–77. [DOI] [PubMed] [Google Scholar]
- Henry J. A., Zaugg T. L., Myers P. J., Kendall C. J., Michaelides E. M. (2010) A triage guide for tinnitus. Journal of Family Practice 59(7): 389–393. [PubMed] [Google Scholar]
- Huang C. Q., Shepherd R. K., Carter P. M., Seligman P. M., Tabor B. (1999) Electrical stimulation of the auditory nerve: Direct current measurement in vivo. IEEE Transactions on Biomedical Engineering 46(4): 461–470. [DOI] [PubMed] [Google Scholar]
- Jackson A., Mavoori J., Fetz E. E. (2006) Long-term motor cortex plasticity induced by an electronic neural implant. Nature 444(7115): 56–60. doi:10.1038/nature05226. [DOI] [PubMed] [Google Scholar]
- Joos K., De Ridder D., Van de Heyning P., Vanneste S. (2014) Polarity specific suppression effects of transcranial direct current stimulation for tinnitus. Neural Plasticity 2014: 930860, doi:10.1155/2014/930860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kreuzer P. M., Landgrebe M., Resch M., Husser O., Schecklmann M., Geisreiter F., Langguth B. (2014) Feasibility, safety and efficacy of transcutaneous vagus nerve stimulation in chronic tinnitus: An open pilot study. Brain Stimulation 7(5): 740–747. doi:10.1016/j.brs.2014.05.003. [DOI] [PubMed] [Google Scholar]
- Kuk F. K., Tyler R. S., Rustad N., Harker L. A., Tye-Murray N. (1989) Alternating current at the eardrum for tinnitus reduction. Journal of Speech and Hearing Research 32(2): 393–400. [DOI] [PubMed] [Google Scholar]
- Landgrebe M., Zeman F., Koller M., Eberl Y., Mohr M., Reiter J., Langguth B. (2010) The Tinnitus Research Initiative (TRI) database: A new approach for delineation of tinnitus subtypes and generation of predictors for treatment outcome. BioMed Central Medical Informatics and Decision Making 10: 42, doi:10.1186/1472-6947-10-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marks K. L., Martel D. T., Wu C., Basura G. J., Roberts L. E., Schvartz-Leyzac K. C., Shore S. E. (2018) Auditory-somatosensory bimodal stimulation desynchronizes brain circuitry to reduce tinnitus in guinea pigs and humans. Science Translational Medicine 10(422): eaal3175, doi:10.1126/scitranslmed.aal3175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mens L. H., Oostendorp T., van den Broek P. (1994) Cochlear implant generated surface potentials: Current spread and side effects. Ear and Hearing 15(4): 339–345. [DOI] [PubMed] [Google Scholar]
- Mielczarek M., Norena A., Schlee W., Olszewski J. (2018) Excitation of the Auditory system as a result of non-invasive extra-cochlear stimulation in normal subjects and tinnitus patients. Fronters in Neuroscience 12: 146, doi:10.3389/fnins.2018.00146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neff P., Michels J., Meyer M., Schecklmann M., Langguth B., Schlee W. (2017) 10 Hz amplitude modulated sounds induce short-term tinnitus suppression. Frontiers in Aging Neuroscience 9: 130, doi:10.3389/fnagi.2017.00130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Norena A. J., Mulders W. H., Robertson D. (2015) Suppression of putative tinnitus-related activity by extra-cochlear electrical stimulation. Journal of Neurophysiology 113(1): 132–143. doi:10.1152/jn.00580.2014. [DOI] [PubMed] [Google Scholar]
- Osaki Y., Nishimura H., Takasawa M., Imaizumi M., Kawashima T., Iwaki T., Kubo T. (2005) Neural mechanism of residual inhibition of tinnitus in cochlear implant users. Neuroreport 16(15): 1625–1628. doi:00001756-200510170-00004 [pii]. [DOI] [PubMed] [Google Scholar]
- Perez R., Shaul C., Vardi M., Muhanna N., Kileny P. R., Sichel J. Y. (2015) Multiple electrostimulation treatments to the promontory for tinnitus. Otology and Neurotology 36(2): 366–372. doi:10.1097/MAO.0000000000000309. [DOI] [PubMed] [Google Scholar]
- Reavis K. M., Rothholtz V. S., Tang Q., Carroll J. A., Djalilian H., Zeng F. G. (2012) Temporary suppression of tinnitus by modulated sounds. Journal of the Association for Research in Otolaryngology 13(4): 561–571. doi:10.1007/s10162-012-0331-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roberts L. E., Eggermont J. J., Caspary D. M., Shore S. E., Melcher J. R., Kaltenbach J. A. (2010) Ringing ears: The neuroscience of tinnitus. Journal of Neuroscience 30(45): 14972–14979. doi:10.1523/JNEUROSCI.4028-10.2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubinstein J. T., Tyler R. S., Johnson A., Brown C. J. (2003) Electrical suppression of tinnitus with high-rate pulse trains. Otology and Neurotology 24(3): 478–485. [DOI] [PubMed] [Google Scholar]
- Rubinstein J. T., Wilson B. S., Finley C. C., Abbas P. J. (1999) Pseudospontaneous activity: Stochastic independence of auditory nerve fibers with electrical stimulation. Hearing Research 127(1–2): 108–118. doi: 10.1016/S0378-5955(98)00185-3. [DOI] [PubMed] [Google Scholar]
- Schaette R., McAlpine D. (2011) Tinnitus with a normal audiogram: Physiological evidence for hidden hearing loss and computational model. Journal of Neuroscience 31(38): 13452–13457. doi:10.1523/JNEUROSCI.2156-11.2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shekhawat G. S., Sundram F., Bikson M., Truong D., De Ridder D., Stinear C. M., Searchfield G. D. (2016) Intensity, duration, and location of high-definition transcranial direct current stimulation for tinnitus relief. Neurorehabilitation and Neural Repair 30(4): 349–359. doi:10.1177/1545968315595286. [DOI] [PubMed] [Google Scholar]
- Shulman A., Tonndorf J., Goldstein B. (1985) Electrical tinnitus control. Acta Oto-Laryngologica 99(3–4): 318–325. 10.3109/00016488509108916. [DOI] [PubMed] [Google Scholar]
- Steenerson R. L., Cronin G. W. (2003) Tinnitus reduction using transcutaneous electrical stimulation. Otolaryngologic Clinics of North America 36(2): 337–344. doi: 10.1016/S0030-6665(02)00164-0. [DOI] [PubMed] [Google Scholar]
- Suk W. C., Kim S. J., Chang D. S., Lee H. Y. (2018) Characteristics of stimulus intensity in transcutaneous vagus nerve stimulation for chronic tinnitus. Journal of International Advanced Otology 14(2): 267–272. doi:10.5152/iao.2018.3977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tang Q., Liu S., Zeng F. G. (2006) Loudness adaptation in acoustic and electric hearing. Journal of the Association for Research in Otolaryngology 7(1): 59–70. doi: 10.1007/s10162-005-0023-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tass P. A., Adamchic I., Freund H. J., von Stackelberg T., Hauptmann C. (2012) Counteracting tinnitus by acoustic coordinated reset neuromodulation. Restorative Neurology and Neuroscience 30(2): 137–159. doi:10.3233/RNN-2012-110218. [DOI] [PubMed] [Google Scholar]
- Tyler R., Stocking C., Secor C., Slattery W. H., 3rd (2014) Amplitude modulated S-tones can be superior to noise for tinnitus reduction. American Journal of Audiology 23(3): 303–308. doi:10.1044/2014_AJA-14-0009. [DOI] [PubMed] [Google Scholar]
- Vernon J. A., Fenwick J. A. (1985) Attempts to suppress tinnitus with transcutaneous electrical stimulation. Otolaryngology—Head and Neck Surgery 93(3): 385–389. [DOI] [PubMed] [Google Scholar]
- Vurek L. S., White M., Fong M., Walsh S. M. (1981) Optoisolated stimulators used for electrically evoked BSER. Annals of Otology, Rhinology and Laryngology 90(82): 21–24. [DOI] [PubMed] [Google Scholar]
- Weisz N., Hartmann T., Dohrmann K., Schlee W., Norena A. (2006) High-frequency tinnitus without hearing loss does not mean absence of deafferentation. Hearing Research 222(1–2): 108–114. doi:10.1016/j.heares.2006.09.003. [DOI] [PubMed] [Google Scholar]
- Weisz N., Muller S., Schlee W., Dohrmann K., Hartmann T., Elbert T. (2007) The neural code of auditory phantom perception. Journal of Neuroscience 27(6): 1479–1484. doi:10.1523/JNEUROSCI.3711-06.2007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wenzel G. I., Sarnes P., Warnecke A., Stover T., Jager B., Lesinski-Schiedat A., Lenarz T. (2015) Non-penetrating round window electrode stimulation for tinnitus therapy followed by cochlear implantation. European Archives of Oto-Rhino-Laryngology 272(11): 3283–3293. doi:10.1007/s00405-014-3413-8. [DOI] [PubMed] [Google Scholar]
- Zeng F. G., Djalilian H., Lin H. (2015) Tinnitus treatment with precise and optimal electric stimulation: Opportunities and challenges. Current Opinion in Otolaryngology and Head and Neck Surgery 23(5): 382–387. doi:10.1097/MOO.0000000000000187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeng F. G., Tang Q., Dimitrijevic A., Starr A., Larky J., Blevins N. H. (2011) Tinnitus suppression by low-rate electric stimulation and its electrophysiological mechanisms. Hearing Research 277(1–2): 61–66. doi:S0378-5955(11)00089-X [pii] 10.1016/j.heares.2011.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeng, F.G., Tran, P., Richardson, M., Sun S. & Xu, Y. (2018). Human sensation of transcranial electric stimulation. Manuscript submitted for publication. [DOI] [PMC free article] [PubMed]