

Abstract
We had designed an educational program for early reporting of suspected child abuse for healthcare providers in South Korea. The purpose of study was to evaluate the effectiveness of education program for health care providers as pilot study. The educational program consisted of two 2-hour-long didactic lectures and was held at 15 hospitals between July and December 2016. We conducted a survey study with physicians, nurses, emergency medical technicians, and other hospital staff. Participants completed survey questionnaires before and after the lecture and 3 months later. The questionnaire contained 3 sections: practical knowledge regarding child abuse, confidence in reporting, and willingness to report. A 10-point Likert scale was used to evaluate the responses. A total of 1103 participants working in 15 different hospitals attended the educational program. In all, 663 participants (75.5%) completed the survey with nurses at 61.7% and physicians at 22%. 26.4% had previously received education about child abuse and reporting methods, and 227 (34.2%) had experience with reporting (direct and indirect) child abuse. The score about knowledge improved from 5.28 points before to 8.03 after the educational program, and was 7.1 after 3 months (P < .001), using a 10-point Likert scale. The confidence increased from 4.76 before the program to 7.59 after it, and was 6.6 after 3 months (P < .001). The willingness to report increased from 7.46 before the program to 8.68 after it, and was 8.14 after 3 months (P < .001). Participants’ satisfaction with the education program was 8.3 points immediately after education and 7.6 points after 3 months. The recommendation index of curriculum was 8.4 points before program and 8.1 points after 3 months. The educational program on the assessment of child abuse and reporting methods increased healthcare professionals’ knowledge and confidence and improved their willingness to report suspected child abuse in a low-perception environment.
Keywords: child abuse, educational program, emergency department, healthcare providers
1. Introduction
Child abuse is a serious public health problem and has long-term consequences that affect the child's life into adulthood.[1] In South Korea, the number of reported cases of child abuse has significantly increased since the Special Act on the Punishment of Child Abuse Crimes was enacted in September of 2014. Nevertheless, the incidence of child abuse was 1.10 per 1000 children in South Korea, while it was 17.24 per 1000 children in the United States.[1–3] In a previous study in Taiwan, lack of education about the recognition and management of child abuse in professionals, including healthcare providers, was reported as the reason for a low incidence rate.[4] In addition, other reasons may be associated with the low reported rate such as some cultural factors, including the severity of punishments.[4] In South Korea, physicians, nurses, emergency medical technicians (EMTs), and social services personnel are among those designated as mandatory reporters, who are required to report suspected child abuse encountered on the job. According to a report by the Child Protection Agency in 2015, 76.1% were found to be actual child abuse cases of all reported cases of child abuse by mandatory reporters and 68.0% were found to be actual child abuse cases in all reported cases by non-mandatory reporters.[5] The accuracy of child abuse reporting by healthcare providers is high, and improved reporting by healthcare providers should also reduce unnecessary reports.[5,6] According to a report by the Child Protection Agency, a total of 19,214 child abuse cases were reported in 2015, of which, only 137 (0.7%) were reported by healthcare providers.[7] For the past 10 years, the reported rate of child abuse by healthcare providers (CAHCP) has been around 1%. This is significantly different from the reported rate of 10% in other major developed countries.[8,9] Although it is possible to prevent the after-effects of child abuse by finding and reporting abuse on the initial visit, education is required to appropriately evaluate child abuse. Unfortunately, this education is not being conducted in South Korea. In some other countries, education related to child abuse is provided to physicians, and several studies have evaluated the effectiveness of such education.[5,10–12] Therefore, the present authors created first an educational training program for child abuse assessment and reporting called the Program for the Early Reporting of CAHCP, or early CAHCP, in 2016. The purpose of study was to evaluate the effectiveness of education program for health care providers as pilot study in South Korea.
2. Methods
2.1. Study design and setting
This was a survey study for the evaluation of an educational program for healthcare providers. The program and surveys were conducted at 15 hospitals with pediatric emergency departments or with emergency department injury surveillance systems in 3 areas (Seoul, Gyeonggi Province, and Gangwon Province) of South Korea between July and December 2016.
We had predicted that about 20 to 50 healthcare providers would come together voluntarily for a one-time educational program. A total of 13 hospitals were expected and approximately 650 participants were expected to be educated. Finally, we educated 1103 participants in 15 hospitals. Among them, 846 participants completed 2 questionnaires before and immediately after the education and 633 participants completed the final questionnaire three months after the education.
2.2. Study participants
A recruitment announcement was made through the homepage and e-mail for regular members of 3 pediatric associations (The Korean Society of Pediatric Emergency Medicine, The Korean Society of Emergency Medicine, and The Korean Pediatric Society). The researchers developed the program through discussions in 4 or more meetings based on the assessment results of the previous year's curriculum, which was scheduled for 4 hours in the form of collective lectures and group discussions. The educational content consisted of an overview of the evaluation methods for child abuse, a description of the class notes being taught, group discussions on cases of child abuse, and a Q&A session. The Child Protection Agency was involved in a combination of case discussions and questions and answers. Instructors who completed a professional instructor course planned the schedule for the educational program for the healthcare providers at their respective hospitals and implemented a 1 to 1.5 h long educational program.
Healthcare providers working at pediatric-related departments, such as the emergency department, pediatric ward or outpatient clinic, and radiologic department, voluntarily applied for the educational program after the announcement of the lecture. The author explained the study's purpose and asked for volunteers. For evaluating the curriculum, a survey was conducted after the educational session by professional instructors. Participants who were late for lectures or did not complete the questionnaires were excluded from the study.
2.3. Ethics committee approval
The study was approved by the SMG-SNU Boramae Medical Center ethics committee (IRB-16-2016-90), and because of the study's retrospective nature, informed consent was not required.
2.4. Intervention
Instructors consisted of medical specialists in the emergency department and pediatrics. Early CAHCP consisted of 2 sections that were scheduled for a total of approximately 2 h. The purpose of the first section was to understand the definition of child abuse, types of child abuse, and child protection agency services. The second section focused on the symptoms of suspected child abuse and reporting methods. We showed x-rays and photographs of child abuses cases to show what injuries to be aware of. The participants were also trained on how to explain a suspected case of child abuse to law enforcement authorities while protecting the reporting person's identity. The total program was expected to last 2 h, with the first section lasting 45 min and the second lasting 60 min, with a 15 min break in between. Participants completed a pre- and post-lecture questionnaire.
2.5. Questionnaire of the survey
The study questionnaire contained 3 different sections with 12 questions in total. The first section included 4 questions regarding healthcare providers’ experience and awareness related to child abuse:
-
1.
Whether they have at work witnessed child abuse;
-
2.
whether they have reported any suspected child abuse at work;
-
3.
whether they have received any education associated with child abuse; and
-
4.
do they perceive themselves as a mandatory reporter for child abuse (Table 1).
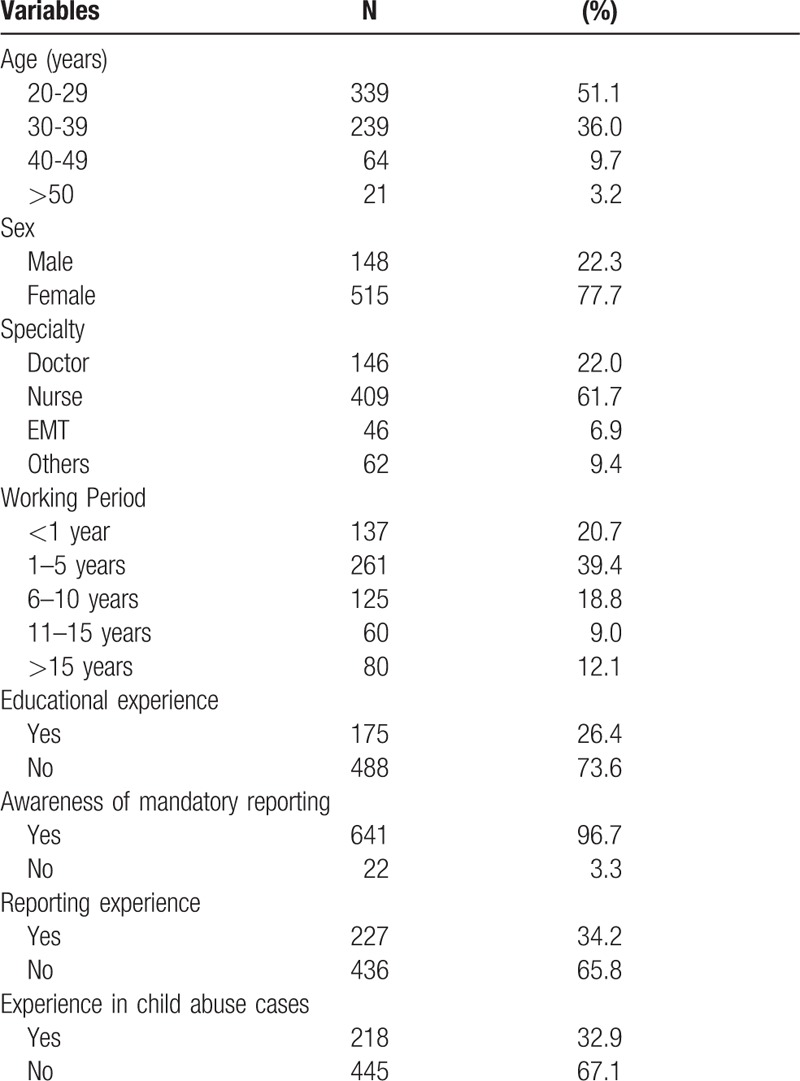
Table 1.
Characteristics, perceptions, knowledge and experience of survey respondents.
The second section pertained to respondents’ practical knowledge in relation to child abuse and their confidence and willingness to report child abuse. A 10-point Likert scale was used for the 8 questions in this section:
-
1.
How much do you know about suspected symptoms or signs of child abuse?
-
2.
How confident can you be when you meet a suspected victim of child abuse?
-
3.
How much do you know about reporting a suspected case of child abuse?
-
4.
How much do you know about the duties and penalties imposed upon mandatory reporters for violations of child abuse laws?
-
5.
If a child visiting the hospital is suspected of being abused, would you be willing to report this?
-
6.
Do you think it is necessary to provide educational programs related to child abuse for healthcare providers?
-
7.
How important do you think the role of healthcare providers is in the early detection of child abuse?
-
8.
Are you willing to participate regularly in the child abuse educational program for healthcare providers? (Table 2).
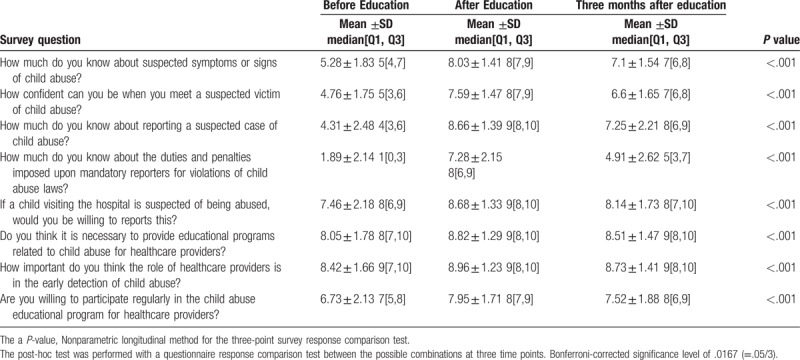
Table 2.
Questionnaires and answer score before, after and 3 months after the lecture.
The final section included demographic information, such as years of practice, field of practice, specific profession, sex, age, work experience, and hospital grade. After this section, respondents were then queried on their satisfaction and understanding of the material presented. Further, they were asked about the ideal amount of time between repetition of the class, ranging from every 6 months, or every year to every 5 years. After 3 months, the survey was administered to participants again to reevaluate the effects of their education.
2.6. Data analysis
We compared the baseline, post-lecture, and 3-month-later results. We then evaluated the differences based on practical experience, knowledge, confidence, willingness to report child abuse, and satisfaction with the provided education. After the implementation of the educational program, suspicious cases of child abuse were confirmed by requesting data from the National Child Protection Agency regarding the number of reported cases. For the 15 hospitals that received education, we confirmed the actual number of child abuse cases by contacting the local child protection agency in each of the 4 districts. The number of reported cases in each district where the program was conducted was then compared with the number of reported cases in the previous year of 2015. In addition, the number of reported cases in the areas that received education was compared with the number of reported cases in the non-educated areas for 2015.
2.7. Statistical analysis
Statistical analysis was employed using SAS V.9.2 (SAS Institute, Cary, NC). Quantitative variables were expressed as the mean ± standard deviation and medians (interquartile ranges). We used nonparametric longitudinal methods to evaluate the education program effects.[13] Two-sided P values <.05 were considered statistically significant. The interactions between occupational group and education and between sex and education were tested. Post-hoc analyses for the questionnaire items showing significant differences between 3 time points (before education, after education, and after 3 months of education) were conducted using pairwise comparison between 2 time points and Bonferroni-corrected significance level of .0167 (= .05/3).
3. Results
3.1. Demographics of participants
A total of 1103 participants from 15 different hospitals attended the educational program. Out of these participants, 877 participated in the survey. Out of these 877, a total of 846 respondents submitted the questionnaire in the first and second round of surveys. At the 3-month mark, 633 participants responded to the survey request, for a response rate of 75.5%. Of those respondents, 515 (77.7%) were female. Stratified along age groups, the largest age group was between 20 and 29 with 339 people (51.1%). Regarding occupational groups, the largest was nurses at 409 (61.7%), 22% of them were physicians, 6.9% were EMTs, and 9.4% were classified as other. The other category included trainees, social workers, nursing assistants, departmental staff, and clinical psychologists. Most respondents had 1 to 5 years of work experience (Table 1). Among the questions related to experience with child abuse victims at work, 178 (26.4%) answered that they had experience with these patients, while 488 (73.6%) answered that they did not have any experience. For awareness of having cases initiated in their hospitals regarding child abuse, 227 (34.2%) reported having cases initiated, while 436 (65.8%) did not. Education regarding child abuse assessment and reporting methods within the past 3 years was only reported by 175 (26.4%) respondents (Table 1).
3.2. Change of knowledge, confidence, and willingness to report after educational program
The answers to the second section pertaining to knowledge, confidence, and willingness to report child abuse are as follows (Table 2). Respondents’ perception of the suspected symptoms of child abuse significantly improved from 5.28 pre-intervention to 8.03 post-intervention, and was 7.2 three months after the program. Confidence in reporting child abuse rose considerably from 4.76 pre-intervention to 7.59 post-intervention, and was 6.6 three months after the program. Knowledge about reporting methods significantly improved from 4.31 pre-intervention to 8.66 post-intervention, and was 7.25 three months after the program. Legal recognition of penalties for child abuse also showed a significant increase after the intervention, starting at 1.86 pre-intervention and increasing to 7.28 post-intervention, but it dropped to 4.91 three months after the program. Based on these data, we confirmed that respondents were unaware of the legal provisions regarding child abuse. After the lecture, the average score rose above the baseline from 5.86 to 8.24. Three months after the program, respondents showed a higher score than pre-intervention, but their scores were lower than the post-intervention results. The post-hoc test showed statistical significance for both before vs after education, before education vs 3 months after education, and after education vs 3 months after education.
Respondents attitudes toward the necessity of child abuse education, intention to participate in such education, and the role of healthcare providers in reporting child abuse all improved after the implementation of this program. Their attitude toward the necessity of such education remained relatively unchanged, starting at 8.05 pre-intervention and going to 8.82 immediately after, and 8.51 three months after the program. We confirmed that respondents felt that child abuse identification and reporting training was necessary even before the intervention. Respondents’ willingness to participate in this educational program was 7.46 pre-intervention, 8.68 post-intervention, and was 8.14 three months after the program (Table 2). The respondents’ satisfaction with this education on child abuse was highest after the program at 8.31 ± 1.54, and went down to 7.56 ± 1.64 after 3 months. Knowing how to report suspected cases of child abuse was also highest after the program, being 8.45 ± 1.36 post-intervention and 7.44 ± 1.67 after 3 months. Respondents’ intention to recommend this program to other healthcare professionals was also highest post-intervention 8.41 ± 1.49 immediately after and 7.97 ± 1.62 after 3 months (Fig. 1). There were significant interactions between occupational group and education and between sex and education in these items.
Figure 1.
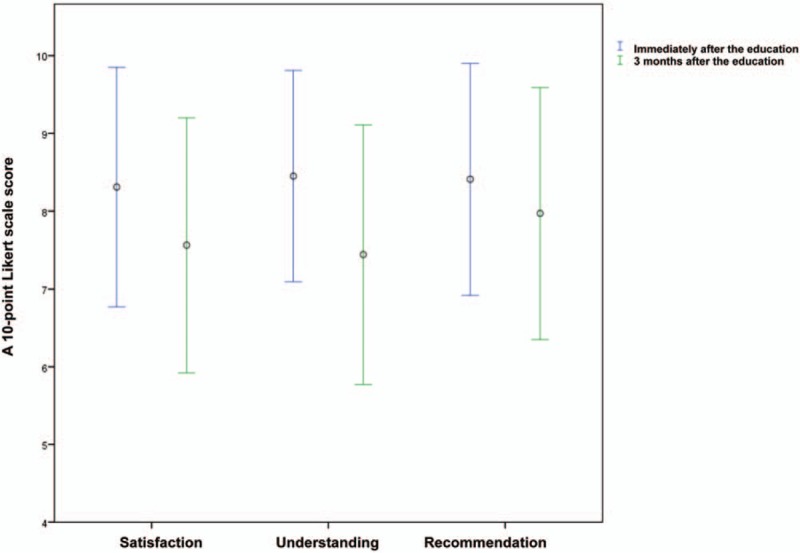
Comparison of respondents’ scores immediately post-intervention and 3 months after for satisfaction, understanding, and recommendation of the educational program. A 10-point Likert scale was used to evaluate the responses. N = 663, Wilcoxon signed rank sum test, P-value < .001.
For the questionnaire item ’How much do you know about reporting a suspected case of child abuse?’ EMTs were 3.74 ± 2.38 pre-intervention, 8.96 ± 1.11 post-intervention, and 7.61 ± 2.25 three months after the program. Nurses were 4.28 ± 2.42 pre-intervention, 8.67 ± 1.4 post-intervention, and 7.3 ± 2.11 three months after the program. Doctors were 4.42 ± 2.44 pre-intervention, 8.53 ± 1.38 post-intervention, and 6.77 ± 2.29 three months after the program. Etc. were 4.69 ± 2.95 pre-intervention, 8.65 ± 1.58 post-intervention, and 7.84 ± 2.42 three months after the program. The result of the interaction with time and occupation is P-value = .0025. The patterns of change before and after education were according to occupation. Therefore, we conducted a comparative analysis between the time points of each occupation. As a result, it was not statistically significant at only .09 in the Etc. occupation group only after the education vs 3 months after the education.
For the questionnaire item ‘Are you willing to participate regularly in the child abuse educational program for healthcare providers?’ for women, 6.69 ± 2.06 before education, 7.96 ± 1.66 immediately after education, and 7.58 ± 1.78 after 3 months. For men, 6.86 ± 2.38 before education, 7.89 ± 1.86 after education and 7.28 ± 2.17 after 3 months. The result of the interaction with time and sex is P-value = .026. According to the gender, the pattern of change before and after the training was different. In males, it was not statistically significant (P = .089) only after 3 months of education vs immediately after education.
3.3. Change in reported cases of suspected child abuse after the educational program
Compared to 2015, in the educated areas of Seoul, Incheon, and Gyeonggi Province, the number of child abuse cases reported in Seoul and Gyeonggi Province increased from 23 to 48 cases ((48–23)/23 × 100 = 109%) and 28 to 55 cases ((55–28)/28 × 100 = 96%), respectively, while Incheon showed no change. In the educated area of Gangwon Province, the number of cases reported also increased by 75% ((7–4)/4 × 100 = 75%) from 4 to 7 cases. Thus, the number of reported cases in all educated areas increased from 67 to 122 cases, for an increase of 82% ((122–67)/67 × 100 = 82%). For the areas where no education was provided, there was a 34% ((94–70)/70 × 100 = 34%) increase in the number of reported cases from 70 to 94, which shows that the rate of increase was much lower than that of educated areas (Fig. 2). Compared with the number of reports by the medical staff in areas not receiving the education, the number of reports by medical staff in educated districts increased significantly (Fig. 2).
Figure 2.
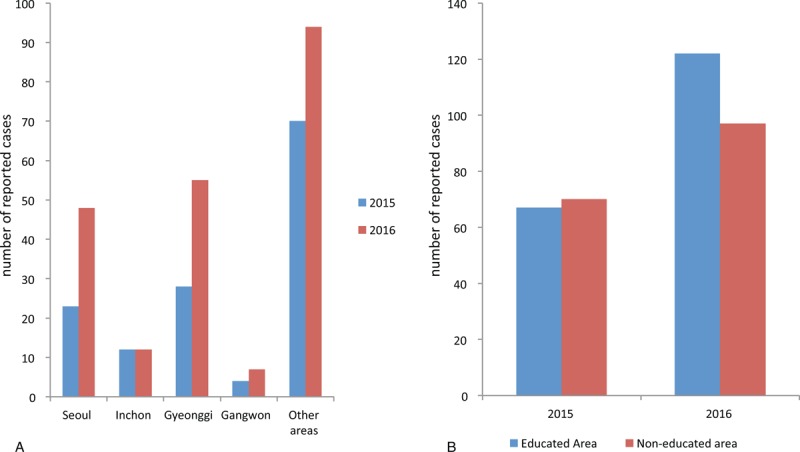
A. Comparison of the number of reported cases in 2015 and 2016 in the educated areas of Seoul, Incheon, and Gyeonggi Province and other areas. B. Comparison of the number of reported cases in educated and non-educated areas in 2015 and 2016.
3.4. Satisfaction with the educational program
In response to the question, "How often do you think education associated with child abuse needs to be provided?” 58 respondents (9%) answered every 6 months, 393 (60%) answered every year, 23% answered every 2 years, 34 (5%) responded every 3 years, and 22 (3%) responded every 5 years, as per the data collected immediately after the educational program. After 3 months, 146 (22%) responded every 6 months, 378 (57%) every year, 99 (15%) every 2 years, 24 (4%) every 3 years, and 11 (2%) answered every 5 years. A yearly reinforcement of this knowledge garnered the most responses.
4. Discussion
This study was the first to examine the effectiveness of an educational program on child abuse for healthcare providers in South Korea. Participants’ knowledge of child abuse increased, with a stronger willingness to report any suspected abuse after the program. Most items showed a significant increase immediately after the program and a slight decrease 3 months after, such as the willingness to report child abuse. This is most likely due to memory decline after 3 months, and this can be used as an argument for having yearly re-education.
Our simple educational program significantly increased healthcare providers’ confidence to evaluate cases of child abuse and willingness to report in a low recognition environment such as that in South Korea. Previous studies have assessed healthcare professionals’ knowledge, attitude, and beliefs regarding child abuse.[9,10] Their knowledge base was found to be significantly limited and in need of improvement; they would greatly benefit from increased educational opportunities.[5] Faculty and residents perceive a lack of adequate child abuse and neglect training in residency.[5,9–11] In one study, a 28-item survey was mailed to the chief residents of pediatric residency training programs in the United States from 2004 to 2005.[5] Ninety-three percent of respondents rated their teaching methods as useful or very useful. Further, 41% of programs required mandatory clinical rotations in child abuse and neglect, 57% offered elective rotations, and 25% offered no rotations at all. Respondents rated the levels of preparedness of graduating residents to address child abuse and neglect as follows: very well (12%), well (54%), somewhat well (28%), or not well (6%). Participants answered that they had confidence in being able to accurately diagnose child abuse after the lecture.[5]
The educational program used in this study was the first such child abuse educational program in South Korea, and it was special because the Child Protection Agency and the Korea Center for Disease Control (KCDC) also participated in it. Japan created a similar educational program for medical institution personnel to combat child maltreatment in 2014.[12] The questionnaire included 12 statements designed to ascertain respondents’ practical knowledge and attitudes relevant to addressing child maltreatment. They compared baseline scores determined before the lecture with those obtained after the lecture. The rate of correct answers for the 12 questionnaire items increased, and for 9 questions, it increased significantly (P < .05). Moreover, the scores for practical knowledge addressing child maltreatment improved significantly and became higher than the baseline scores scores (11.18 vs 10.57; t = −9.94, P < .01).[12] The United Kingdom (UK) has also developed a child abuse educational program for pediatric residents. The Level I program, "Safeguarding Children: Recognition and Response in Child Protection,” was launched nationally in the UK as an educational program for pediatricians in education.[12] This program used a standardized intensive day course taught by experienced trainers and was held in venues throughout the country. It aimed to raise awareness and better equip pediatricians with the knowledge and skills to assist them in recognizing and appropriately responding to child abuse competently. Early outcome measures might include improvements in attitudes, knowledge, and levels of confidence.[14,15] Through these studies, we know that many physicians have limited clinical education in child abuse that prompted the creation of this program. In addition to the lack of education among residents, there is also limited education for nurses and other healthcare providers. Increased knowledge and resident engagement with these programs as seen in these studies demonstrate the adequacy of initiating such a program for all healthcare providers.
An increase in the number of reported cases in the educated areas was a meaningful result, but it was only for a year. If a higher number of reported cases in the region can be observed after many years of education regarding child abuse, then it can be considered as a clear positive effect of such education. In our study, the post-intervention score was higher than the pre-intervention score for all questions. Three months later, the score was lower than that obtained immediately after the program, but not lower than the pre-intervention score. Our study included a relatively high percentage of non-physician participants, especially nurses. However, there was no statistical difference between occupational groups.
This study, however, has several limitations. First, it has a small sample size, and the study period is short. This was a pilot study designed to examine the effectiveness of the educational program we have developed. The increase in the number of reported cases in 6 months can be considered a positive sign; however, a longer study with a larger sample should be conducted to obtain clearer results. Second, we were unable to obtain any data from those who declined to submit the questionnaires. This could have skewed the results toward those who were engaged with the material and could represent some inadequacies in our design. Third, in terms of occupational categories, the adherence rate in the target population was 61.7% among nurses, 22% among physicians, and 6.9% among EMTs. Factors such as work overload, complexity of the object of research, lack of interest and education, and lack of compensation for participation in the study may be related to these rates. Medical professionals’ education and knowledge are also limitations inherent to the cross-sectional design of the study that measures a particular phenomenon in a single moment. This makes it difficult to deepen it and might be possible through qualitative research.
Fourth, our study has a population bias since it is limited to most healthcare providers working in the emergency room. The increase in the number of reported cases in the educated areas was a meaningful result, but it may be because voluntary practitioners were more interested in the subject of child abuse. The pre-intervention survey results may be higher for those participants that are interested in the subject. Finally, our study only educated healthcare providers at secondary or tertiary hospitals; thus, in order to expand more medical professionals, we need to develop additional programs for clinical physicians, including primary care practitioners. This educational program must be offered to all doctors who have contact with children and their families. There is a limited amount of research that shows the effectiveness of child protection education in this regard, at least in the short term. Moreover, effective education should not only provide the knowledge and skills required to address these challenges but also promote the development of appropriate attitudes and perceptions regarding the doctor's role in the protection of children from abuse or neglect. Long-term efficacy studies should be conducted through education of healthcare providers from all areas. The study's design and education program should be modified and developed in a more efficient way that enhances the overall effectiveness of the study in the future study.
5. Conclusions
The educational program that we developed regarding the assessment and reporting of child abuse cases increased healthcare providers’ knowledge and effectively strengthened their willingness to report such cases. Further, such education should be provided regularly in order to maximize and maintain its effectiveness for extended periods.
Acknowledgments
We would like to express our gratitude and appreciation to the physicians, nurses, and EMTs from the emergency departments of 15 hospitals who voluntarily attended this project. We would especially like to thank Chang-Pyo Hong, a specialist in the National Child Protection Agency, and Hwa Jeong Jang, the Director of the National Child Protection Agency, who participated in the development of educational program and provided the data of reporting cases. Finally, we would like to thank researchers Yul Bin Jang and Eun Sung Lee who collected the questionnaire for this study. This work was funded by the Ministry of Health and Welfare, Republic of Korea (grant number: 2016E1159A).
Author contribution
Approval of final manuscript: all authors.
Conceptualization: Paek SH, Jung JH, and Kwak YH.
Data curation: Paek SH and Noh H.
Formal analysis: Paek SH and Jung JH.
Writing – original draft: Paek SH and Jung JH.
Writing – review and editing: Jung JH and Kwak YH.
Footnotes
Abbreviations: CAHCP = child abuse by healthcare providers, EMT = emergency medical technician, KCDC = Korea Center for Disease Control, UK = United Kingdom.
The present study was funded by the Ministry of Health and Welfare in Korea (grant number: 2016E1159A).
The authors have no conflict of interest to disclose.
References
- [1].Lee HM, Kim JS. Predictors of intention of reporting child abuse among emergency nurses. J Pediatr Nurs 2018;38:e47–52. [DOI] [PubMed] [Google Scholar]
- [2].Korea Ministry of Health and Welfare, National Child Protection Agency. Child Abuse & Neglect Korea 2014. [online] Available at: http://www.korea1391.go.kr/new/bbs/download.php?bo_table=report&wr_id=9450&no=0 Accessed December 1, 2017. [Google Scholar]
- [3].U.S. Department of Health & Human Services Administration for Children and Families Administration on Children, Youth and Families Children's Bureau. Child maltreatment 2013. [online] Available at: https://www.acf.hhs.gov/cb/resource/child-maltreatment-2013 Accessed December 1, 2017. [Google Scholar]
- [4].Chang YC, Huang JL, Hsia SH, et al. Child protection medical service demonstration centers in approaching child abuse and neglect in Taiwan. Medicine (Baltimore) 2016;95:e5218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Narayan AP, Socolar RR, St Claire K. Pediatric residency training in child abuse and neglect in the United States. Pediatrics 2006;117:2215–21. [DOI] [PubMed] [Google Scholar]
- [6].Ainsworth F, Hansen P. Five tumultuous years in Australian child protection: Little progress. Child Fam Soc Work 2006;11:33–41. [Google Scholar]
- [7].Korea Ministry of Health and Welfare, National Child Protection Agency. Child Abuse & Neglect Korea 2014. [online] Available at: http://www.korea1391.go.kr/new/bbs/download.php?bo_table=report&wr_id=9866&no=0 Accessed December 1, 2017. [Google Scholar]
- [8].Jung JH, Kwak YH. Review of the screening tool for child abuse by health care provider. Pediatr Emerg Med J 2015;2:1–7. [Google Scholar]
- [9].Dubowitz H, Black M. Teaching pediatric residents about child maltreatment. J Dev Behav Pediatr 1991;12:305–7. [PubMed] [Google Scholar]
- [10].Woolf A, Taylor L, Melnicoe L, et al. What residents know about child abuse: Implications of a survey of knowledge and attitudes. Am J Dis Child 1988;142:668–72. [DOI] [PubMed] [Google Scholar]
- [11].Palusci VJ, McHugh MT. Interdisciplinary training in the evaluation of child sexual abuse. Child Abuse Negl 1995;19:1031–8. [DOI] [PubMed] [Google Scholar]
- [12].Tanoue K, Senda M, An B, et al. Training program for Japanese medical personnel to combat child maltreatment. Pediatr Int 2017;59:764–8. [DOI] [PubMed] [Google Scholar]
- [13].Brunner E, Puri ML. Nonparametric methods in factorial designs. Stat Pap (Berl) 2001;42:1–52. [Google Scholar]
- [14].Shabde N. Child protection training for paediatricians. Arch Dis Child 2006;91:639–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Bannon M, Carter YH. Paediatricians and child protection: the need for effective education and training. Arch Dis Child 2003;88:560–2. [DOI] [PMC free article] [PubMed] [Google Scholar]