

Abstract
Background
As the aging society progresses, the average age of mothers is also increasing. Advanced maternal age has been known to be associated with perinatal outcomes, as well as birth weight (BW). In this study, we aimed to investigate the perinatal factors associated with low birth weight infants (LBWIs) using birth statistics of the Korean population.
Methods
Birth statistics between 1993 and 2016 from the Korean Statistical Information Service were reviewed. We investigated 12,856,614 data points, which included the number of births, BWs, percentage of preterm births and LBWIs, multiple pregnancies, and maternal age.
Results
The proportion of LBWIs delivered by mothers of advanced maternal age has gradually increased since 1993. In addition, the proportion of older mothers (≥ 35 years old) giving birth to LBWIs has increased over the years. Average BW has a negative correlation with the ratio of preterm births, LBW, multiple births, and advanced maternal age. The mean BW also has a negative correlation with maternal age.
Conclusion
This study shows that the average BW continues to decline, and the incidence of LBWIs is increasing in Korea since 1993. This study also revealed that several perinatal factors, including percentage of preterm births, LBWIs, multiple births, and maternal age influence the mean BW. Although this study did not investigate the effects of decreasing mean BW on perinatal health, future research is worth discussing.
Keywords: Birth Weight; Premature Birth; Infant, Low Birth Weight; Maternal Age; Korea
Graphical Abstract
INTRODUCTION
Birth weight (BW) is significant because it is strongly associated with infant mortality, birth defects, developmental problems in childhood, and risk of various diseases in adulthood.1,2,3 Factors causing decreases in BW include preterm birth, multiple births, maternal age at delivery, underlying maternal diseases, gender of fetus, energy intake restrictions and dietary regulation during pregnancy, and pregnancy assisted by reproductive technology.4,6,7,8 Low BW, associated with inadequate fetal nutrition and growth restriction, increases the risk of serious neonatal morbidity or mortality.9
Although the social and medical environment in Korea has improved in recent years, fertility rates are still declining each year (1.17 births per 1,000 fertile women in 2016).10,11 Recent trends of delayed marriage and childbearing due to social and higher educational advancement of women are contributing to the increase in maternal ages in Korea.12 Advanced maternal age continues to be associated with a range of adverse pregnancy outcomes, including preterm birth, low birth weight infants (LBWIs), birth defects, and pregnancy complications, such as gestational diabetes, placenta previa, and early preeclampsia.5,13
This article presents population BW trends in Korea and their related perinatal factors, such as percentage of preterm births, LBWIs, multiple births, and maternal age from 1993 to 2016 using birth and nutritional statistics of the Korean population.
METHODS
Subjects and data sources
In this study, raw data for all live births from 1993 to 2016 were obtained from the Korean Statistical Information Service. A total of 12,856,614 birth data points were considered, including the number of total births, BW, preterm births, number of LBWIs, multiple births, and maternal age. Mean BW, mean maternal age, rates of preterm births, LBWIs, and multiple births, and advanced maternal age were calculated for each year. Preterm birth rates for 1993 and 1994 were not reported; therefore, they were not included in the analysis. Data from previous reports for the number of births, mean BW, and perinatal factors associated with BW from 1993 through 2016 were compared statistically. In addition, trend analysis was performed for each variable for each year.
Women were classified into nine categories according to maternal age: < 15, 15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, and ≥ 50 years. Advanced maternal age in this study was defined as ≥ 35 years.
Statistical analysis
Linear regression analysis was performed to confirm associations between dependent (BW) and independent (preterm birth, LBWIs, multiple births, mean maternal age, and advanced maternal age) variables. In order to minimize multicollinearity of independent variables, ridge regression analysis was performed to obtain the regression coefficient that minimizes the Mean Squared Error. We conclude that there was a trend if the regression coefficient was significant. A Mann-Kendall trend test was performed for data with variable frequency. All data were analyzed by the statistical program R version 3.3.1 (https://cran.r-project.org, R Foundation for statistical computing, Vienna, Austria). The code for the variance inflation factor (VIF), to verify multicollinearity, was “vif,” “lm” for linear regression analysis, “lmridge” for ridge regression analysis, and “mk.test” for Mann-Kendall trend test. The significance level of all statistical analysis was P < 0.05.
RESULTS
Number of live births
The total number of live births from 1993 to 2016 was 12,856,614 in Korea. The number of births per year has gradually decreased, from 72,300 in 1993 to 40,600 in 2016. This is a decrease of 31,700 over the last 24 years (Table 1).
Table 1. Changes in the number of births, mean BW and related factors in Korean neonate (1993–2016).
| Year | No. of births | BW, g | Preterm births, % | LBWIs, % | Multiple births, % | Age of mother, yr | Advanced maternal age, % |
|---|---|---|---|---|---|---|---|
| 1993 | 723,900 | 3,360 | - | 2.6 | 1.1 | 27.6 | 3.8 |
| 1994 | 728,500 | 3,350 | - | 2.8 | 1.1 | 27.8 | 4.3 |
| 1995 | 721,100 | 3,390 | 2.5 | 3.0 | 1.3 | 27.9 | 4.7 |
| 1996 | 691,226 | 3,340 | 3.1 | 3.1 | 1.4 | 28.1 | 5.3 |
| 1997 | 668,344 | 3,330 | 3.2 | 3.3 | 1.4 | 28.3 | 5.7 |
| 1998 | 634,790 | 3,310 | 3.5 | 3.5 | 1.5 | 28.5 | 6.0 |
| 1999 | 614,233 | 3,300 | 3.8 | 3.6 | 1.6 | 28.7 | 6.2 |
| 2000 | 634,501 | 3,260 | 3.8 | 3.8 | 1.7 | 29.0 | 6.7 |
| 2001 | 554,895 | 3,260 | 4.3 | 4.0 | 1.8 | 29.3 | 7.4 |
| 2002 | 492,111 | 3,270 | 4.4 | 4.0 | 2.0 | 29.5 | 8.0 |
| 2003 | 490,543 | 3,260 | 4.5 | 4.1 | 2.0 | 29.7 | 8.4 |
| 2004 | 472,761 | 3,260 | 4.6 | 4.2 | 2.1 | 30.0 | 9.4 |
| 2005 | 435,031 | 3,250 | 4.8 | 4.3 | 2.2 | 30.2 | 10.6 |
| 2006 | 448,153 | 3,240 | 4.9 | 4.4 | 2.4 | 30.4 | 11.8 |
| 2007 | 493,189 | 3,240 | 5.2 | 4.7 | 2.7 | 30.6 | 13.0 |
| 2008 | 465,892 | 3,230 | 5.5 | 4.9 | 2.7 | 30.8 | 14.3 |
| 2009 | 444,849 | 3,220 | 5.7 | 4.9 | 2.7 | 31.0 | 15.4 |
| 2010 | 470,171 | 3,220 | 5.8 | 5.0 | 2.7 | 31.3 | 17.0 |
| 2011 | 471,265 | 3,210 | 6.0 | 5.2 | 2.9 | 31.4 | 18.0 |
| 2012 | 484,550 | 3,210 | 6.3 | 5.3 | 3.2 | 31.6 | 18.7 |
| 2013 | 436,455 | 3,200 | 6.5 | 5.5 | 3.3 | 31.8 | 20.2 |
| 2014 | 435,435 | 3,200 | 6.7 | 5.7 | 3.5 | 32.0 | 21.6 |
| 2015 | 438,420 | 3,200 | 6.9 | 5.7 | 3.7 | 32.2 | 23.9 |
| 2016 | 406,300 | 3,200 | 7.2 | 5.9 | 3.9 | 32.4 | 26.3 |
BW = birth weight, LBWIs = low birth weight infants.
Perinatal factors
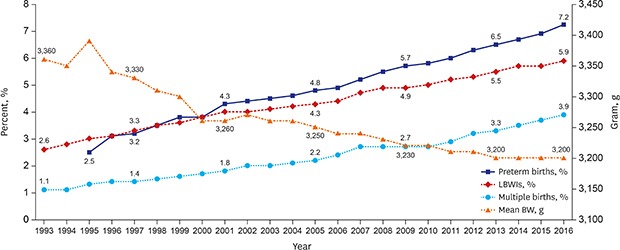
Mean BW was 3,360 g in 1993 and 3,200 g in 2016, a decrease of 160 g during the study period. Mean BW stayed the same or decreased every year except between 1994 and 1995, and between 2001 and 2002. The proportion of preterm births increased significantly by 2.9-fold (2.5%–7.2%) between 1995 and 2016, as well as an increase in the rate of LBWIs by 2.3-fold (2.6%–5.9%) between 1993 and 2016. The proportion of multiple births to total live births increased 3.5-fold (1.1%–3.9%) between 1993 and 2016. It has increased sharply since 2010 (Fig. 1). In 1993, the average maternal age was 27.55 years, and in 2016 was 32.40 years, which is an increase of 4.85 years. The rate of advanced maternal age was 3.8% in 1993 and 26.3% in 2016, which is a significant increase (Fig. 2).
Fig. 1. Changes of mean BW, percentage of preterm births, LBWIs, and multiple births in Korea (1993–2016).

BW = birth weight, LBWIs = low birth weight infants.
Fig. 2. Changes of mean maternal age and proportion of advanced maternal age in Korea (1993–2016).

Trends in BW, preterm births, LBWIs, multiple births, maternal age, and advanced maternal age
We analyzed changes between each year (1993–2016) in the number of births, mean BW, and maternal age, along with rates of preterm births, LBWIs, multiple births, and advanced maternal ages using linear regression for trend test (Fig. 3A). The results of the trend test are shown in the graph using the beta estimate of each variable, and the error bar of the graph indicates the confidence interval. In order to show the trend of each variable as a single graph, the units of variables are adjusted as shown in the figure. The results showed a significant decrease in the total number of births (estimate −1.40, P < 0.001) and mean BW (estimate −0.76, P < 0.001). There was also a significant increase in the number of preterm births (estimate 2.04, P < 0.001), LBWIs (estimate 1.38, P < 0.001), multiple births (estimate 1.18, P < 0.001), maternal age (estimate 2.61, P < 0.001), and advanced maternal age (estimate 0.93, P < 0.001).
Fig. 3. Linear regression for trend test by year (1993–2016). (A) Trends in the number of births, mean BW and related factors. (B) Trends in the percentages of LBWIs categorized by maternal age groups.

LBWIs = low birth weight infants.
‰ = 1/1,000.
Distribution of LBWIs by maternal age among total live births
We calculated the distribution of LBWIs at 5-year intervals according to maternal age for the total number of births (Table 2). All maternal age groups showed an increase in the proportion of LBWIs during the period of 1995 to 2015. In particular, the rate of LBWIs was found to be greatly increased in the group of maternal age ≥ 35 years old (4.8% in 1995 to 23.9% in 2015).
Table 2. The distribution of LBWIs by maternal age among total live births.
| Maternal age, yr | 1995, % | 2000, % | 2005, % | 2010, % | 2015, % |
|---|---|---|---|---|---|
| < 15 | 0 | 0 | 0 | 2.9 | 12.5 |
| 15–19 | 4.2 | 5.3 | 3.9 | 6.2 | 7.8 |
| 20–24 | 2.9 | 3.5 | 3.9 | 4.8 | 5.1 |
| 25–29 | 2.7 | 3.4 | 3.8 | 4.3 | 4.6 |
| 30–34 | 3.3 | 4.1 | 4.3 | 4.9 | 5.6 |
| 35–39 | 4.9 | 5.7 | 6.0 | 6.4 | 7.0 |
| 40–44 | 6.6 | 7.3 | 7.0 | 7.3 | 7.7 |
| 45–49 | 3.7 | 6.9 | 8.8 | 9.8 | 13.4 |
| ≥ 50 | 0 | 13.0 | 11.5 | 9.7 | 7.1 |
| Unknown | 4.1 | 1.2 | 4.8 | 5.3 | 3.0 |
| ≥ 35 (advanced age) | 4.8 | 6.7 | 10.6 | 17.0 | 23.9 |
| Total | 3.0 | 3.9 | 4.1 | 5.0 | 5.7 |
LBWIs = low birth weight infants.
Percentages of LBWIs from 1993 to 2016, categorized by maternal age groups, were analyzed by linear regression for trend test (Fig. 3B). There was no significant difference between age groups < 15 and ≥ 50 years. A significant declining trend was observed in age groups 15 to 29 years (P < 0.001), but significant increase was observed in age groups 30 to 49 years (P < 0.001).
Factors associated with mean BW
Univariate linear regression analysis, exploring variables related to average BW, showed negative correlations with BW and preterm births, LBWIs, multiple births, average maternal age, and advanced maternal age (estimates −0.04, −0.05, −0.06, −0.04, and −0.01, respectively) and each variable showed statistical significance (P < 0.001) (Table 3).
Table 3. Univariate linear regression analysis on the relationship of variables related to mean BW.
| Variables | Estimate | SE | t value | Pr (> |t|) | Adjusted R2 |
|---|---|---|---|---|---|
| Preterm births, % | −0.04 | 0.00 | −12.21 | < 0.001 | 0.88 |
| LBWIs, % | −0.05 | 0.00 | −14.51 | < 0.001 | 0.90 |
| Multiple births, % | −0.06 | 0.01 | −10.36 | < 0.001 | 0.82 |
| Average maternal age, yr | −0.04 | 0.00 | −14.68 | < 0.001 | 0.90 |
| Advanced maternal age, % | −0.01 | 0.00 | −8.20 | < 0.001 | 0.74 |
BW = birth weight, SE = standard error, LBWIs = low birth weight infants.
Multivariate regression showed multicollinearity occurred among the variables. To solve this problem, we used Ridge regression analysis to minimize multicollinearity (Table 4). Following multivariate ridge regression analysis, preterm births, LBWIs, and average maternal age still showed negative correlation with mean BW (estimates −0.08, −0.07, and −0.08 respectively), which was significant (P < 0.001). On the other hand, the relationship between mean BW and multiple births was not statistically significant in ridge analysis (P = 0.498).
Table 4. Multivariate ridge regression analysis on the relationship of variables related to mean BW.
| Variables | Estimate | SE | t value | Pr (> |t|) | VIF | Adjusted R2 |
|---|---|---|---|---|---|---|
| Intercept | 6.32 | 30.76 | 0.21 | < 0.001 | - | 0.794 |
| Preterm births, % | −0.08 | 0.01 | −5.91 | < 0.001 | 0.57 | |
| LBWIs, % | −0.07 | 0.01 | −6.43 | < 0.001 | 0.37 | |
| Multiple births, % | 0.01 | 0.02 | 0.68 | 0.498 | 0.98 | |
| Average maternal age, yr | −0.08 | 0.01 | −5.59 | < 0.001 | 0.64 |
BW = birth weight, SE = standard error, LBWIs = low birth weight infants, VIF = variance inflation factors.
DISCUSSION
Korea is currently experiencing a decline in birth rates, which is believed to be due to reduced marriage rates and delays in marriage. Maternal age is increasing and there are concerns about perinatal complications and newborn health issues due to older mothers. The purpose of this study was to analyze trends of BW and associated factors, such as percentage of preterm births, LBWIs, multiple births, and maternal age in Korean populations. We investigated whether there was an increase in maternal age from 1993 to 2016 and whether the birth rate in this older group is increasing. Furthermore, we also studied changes in BW and incidences of LBWIs, preterm births, multiple births, and rate of LBWIs in older women. Our results show that between 1993 and 2016, there was a significant decline in the number of total births and average BW. In contrast, there was a significant increase in the proportion of preterm births, LBWIs, multiple births, and advanced maternal age. We also found that the rate of LBWIs in women over 35 years old has been rising greatly during the same period. Mean BW showed a statistically significant negative correlation with preterm births, LBWIs, and average maternal age.
Although neonatal mortality of LBWIs has decreased dramatically due to the recent development of intensive care units in Korea, it is still the case that the lower the BW, the lower the survival rate of a newborn.9 According to a study reported in Korea, congenital defects were shown to be associated with LBWIs, preterm births, and multiple births.1 A systematic review also reported that neonatal factors, including low BW are associated with increased risk of intellectual disabilities.2
Results of this study, along with results of several studies previously reported, found factors associated with older maternal age and BW loss.5,14,15,16 Other factors known to affect BW loss in previous studies were primiparous,17 cesarean section,18 multiple birth,19,20 and maternal body mass index.17,21 Nutritional status,22,23 pre-pregnancy low BW and short stature,24,25 inappropriate antenatal care,25 teenage pregnancy,18,26,27 smoking,28 and female gender of infant18,20,28 also were factors.
We found that the maternal age is increasing in recent years in Korea, which is related to later marriage, development of assisted reproductive technology, and the increased education and economic activities of women. Many studies have investigated advanced maternal age and the unfavorable pregnancy outcomes in Korea. The risk of LBWIs and very LBWIs was high in mothers ≥ 35 years and the proportion of advanced maternal age and LBWIs in older mothers has increased.18,29 In a study analyzing birth statistics from 1960 to 2010, both hospital unit and Statistics Korea data showed that the higher the maternal age, the higher the risk of both high birth weight infant (HBWI) and LBWI.30 In a survey using hospital data, maternal age ≥ 35 years was associated with LBWIs, Apgar scores less than 7, and chromosomal abnormalities. Also maternal age ≥ 30 years had a risk of gestational diabetes mellitus, placenta previa, cesarean section, preterm births, and admission to the neonatal intensive care unit.5
There is still controversy regarding factors correlated with advanced maternal age. Contemporary older mothers tend to be well educated and have higher social status than older mothers from past decades.13 There have been some studies that have shown benefits of increased maternal age. A longitudinal survey, recently conducted in Japan, showed that children of older mothers had a lower risk of early health indicators, such as unintentional accidents, and lower hospitalization rates.14 In addition, prospective studies, conducted in five low and middle-income countries, showed mothers > 35 years had an advantage over younger mothers in nutritional status and education.5
The strength of this study is that it contains the most recent research on BW changes with maternal age and related perinatal factors in Korea. Our data suggests how to cope with advanced maternal age
and BW loss. Furthermore, the results show that it may be helpful to increase surveillance of older mothers to detect early signs of negative pregnancy outcomes. In contrast, a limitation of this study was the difficulty in collecting data from the Korean Statistical Information Service on other biological or socioeconomic factors that could affect BW. Therefore, additional analysis was not possible. Further large-scale research in the biological or socioeconomic factors in Korea is needed in the future.
Future research, including prospective and comparative studies, should consider how increase in maternal age is related to increase in premature infants or LBWIs after taking into account the increasing social advancement and trend toward higher education of women. Given the increasing rate of advanced maternal age and LBWIs, more attention and improvement should be given to their control. Advanced age of childbirth affects preterm births, multiple births, and LBWIs, so proper institutional arrangements should be made to reduce this risk. There is a need for aggressive antenatal screening and early detection of complications, along with an individualized protocol for older mothers.
Footnotes
Disclosure: The authors have no potential conflicts of interest to disclose.
- Conceptualization: Kim HE, Bae CW.
- Data curation: Song IG, Chung SH, Choi YS, Bae CW.
- Formal analysis: Song IG, Chung SH.
- Writing - original draft: Kim HE.
- Writing - review & editing: Chung SH.
References
- 1.Kim MA, Yee NH, Choi JS, Choi JY, Seo K. Prevalence of birth defects in Korean livebirths, 2005–2006. J Korean Med Sci. 2012;27(10):1233–1240. doi: 10.3346/jkms.2012.27.10.1233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Huang J, Zhu T, Qu Y, Mu D. Prenatal, perinatal and neonatal risk factors for intellectual disability: a systemic review and meta-analysis. PLoS One. 2016;11(4):e0153655. doi: 10.1371/journal.pone.0153655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.McNeill G, Tuya C, Smith WC. The role of genetic and environmental factors in the association between birthweight and blood pressure: evidence from meta-analysis of twin studies. Int J Epidemiol. 2004;33(5):995–1001. doi: 10.1093/ije/dyh260. [DOI] [PubMed] [Google Scholar]
- 4.Shin SM, Chang YP, Lee ES, Lee YA, Son DW, Kim MH, et al. Low birth weight, very low birth weight rates and gestational age-specific birth weight distribution of Korean newborn infants. J Korean Med Sci. 2005;20(2):182–187. doi: 10.3346/jkms.2005.20.2.182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Koo YJ, Ryu HM, Yang JH, Lim JH, Lee JE, Kim MY, et al. Pregnancy outcomes according to increasing maternal age. Taiwan J Obstet Gynecol. 2012;51(1):60–65. doi: 10.1016/j.tjog.2012.01.012. [DOI] [PubMed] [Google Scholar]
- 6.Zhang J, Bowes WA., Jr Birth-weight-for-gestational-age patterns by race, sex, and parity in the United States population. Obstet Gynecol. 1995;86(2):200–208. doi: 10.1016/0029-7844(95)00142-e. [DOI] [PubMed] [Google Scholar]
- 7.Dharmalingam A, Navaneetham K, Krishnakumar CS. Nutritional status of mothers and low birth weight in India. Matern Child Health J. 2010;14(2):290–298. doi: 10.1007/s10995-009-0451-8. [DOI] [PubMed] [Google Scholar]
- 8.Kondapalli LA, Perales-Puchalt A. Low birth weight: is it related to assisted reproductive technology or underlying infertility? Fertil Steril. 2013;99(2):303–310. doi: 10.1016/j.fertnstert.2012.12.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bae YM, Bae CW. The changes in the mortality rates of low birth weight infant and very low birth weight infant in Korea over the past 40 years. J Korean Med Sci. 2004;19(1):27–31. doi: 10.3346/jkms.2004.19.1.27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lim JW. The changing trends in live birth statistics in Korea, 1970 to 2010. Korean J Pediatr. 2011;54(11):429–435. doi: 10.3345/kjp.2011.54.11.429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fertility rate. [Updated 2017]. [Accessed July 10, 2018]. http://www.index.go.kr/potal/main/EachDtlPageDetail.do?idx_cd=1428.
- 12.Song JE, Ahn JA, Lee SK, Roh EH. Factors related to low birth rate among married women in Korea. PLoS One. 2018;13(3):e0194597. doi: 10.1371/journal.pone.0194597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kenny LC, Lavender T, McNamee R, O'Neill SM, Mills T, Khashan AS. Advanced maternal age and adverse pregnancy outcome: evidence from a large contemporary cohort. PLoS One. 2013;8(2):e56583. doi: 10.1371/journal.pone.0056583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kato T, Yorifuji T, Yamakawa M, Inoue S, Doi H, Eboshida A, et al. Association of maternal age with child health: A Japanese longitudinal study. PLoS One. 2017;12(2):e0172544. doi: 10.1371/journal.pone.0172544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Marozio L, Picardo E, Filippini C, Mainolfi E, Berchialla P, Cavallo F, et al. Maternal age over 40 years and pregnancy outcome: a hospital-based survey. J Matern Fetal Neonatal Med. 2017:1–7. doi: 10.1080/14767058.2017.1410793. [DOI] [PubMed] [Google Scholar]
- 16.Lee JJ. Effect of women's first childbearing age on the risk of low birth weight. Korean J Pediatr. 2007;50(12):1206–1211. [Google Scholar]
- 17.Shin YH, Choi SJ, Kim KW, Yu J, Ahn KM, Kim HY, et al. Association between maternal characteristics and neonatal birth weight in a Korean population living in the Seoul metropolitan area, Korea: a birth cohort study (COCOA) J Korean Med Sci. 2013;28(4):580–585. doi: 10.3346/jkms.2013.28.4.580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Shin SM, Chang YP, Lee ES, Lee YA, Son DW, Kim MH, et al. Low birth weight, very low birth weight rates and gestational age-specific birth weight distribution of Korean newborn infants. J Korean Med Sci. 2005;20(2):182–187. doi: 10.3346/jkms.2005.20.2.182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Choi SH, Park YS, Shim KS, Choi YS, Chang JY, Hahn WH, et al. Recent trends in the incidence of multiple births and its consequences on perinatal problems in Korea. J Korean Med Sci. 2010;25(8):1191–1196. doi: 10.3346/jkms.2010.25.8.1191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kim S, Lee JJ, Kim JH, Lee JH, Yun SW, Chae SA, et al. Changing patterns of low birth weight and associated risk factors in Korea, 1995–2007. Korean J Perinatol. 2010;21(3):282–287. [Google Scholar]
- 21.Cnattingius S, Villamor E, Johansson S, Edstedt Bonamy AK, Persson M, Wikström AK, et al. Maternal obesity and risk of preterm delivery. JAMA. 2013;309(22):2362–2370. doi: 10.1001/jama.2013.6295. [DOI] [PubMed] [Google Scholar]
- 22.Dharmalingam A, Navaneetham K, Krishnakumar CS. Nutritional status of mothers and low birth weight in India. Matern Child Health J. 2010;14(2):290–298. doi: 10.1007/s10995-009-0451-8. [DOI] [PubMed] [Google Scholar]
- 23.Watson PE, McDonald BW. The association of maternal diet and dietary supplement intake in pregnant New Zealand women with infant birthweight. Eur J Clin Nutr. 2010;64(2):184–193. doi: 10.1038/ejcn.2009.134. [DOI] [PubMed] [Google Scholar]
- 24.Han Z, Mulla S, Beyene J, Liao G, McDonald SD Knowledge Synthesis Group. Maternal underweight and the risk of preterm birth and low birth weight: a systematic review and meta-analyses. Int J Epidemiol. 2011;40(1):65–101. doi: 10.1093/ije/dyq195. [DOI] [PubMed] [Google Scholar]
- 25.Mumbare SS, Maindarkar G, Darade R, Yenge S, Tolani MK, Patole K. Maternal risk factors associated with term low birth weight neonates: a matched-pair case control study. Indian Pediatr. 2012;49(1):25–28. doi: 10.1007/s13312-012-0010-z. [DOI] [PubMed] [Google Scholar]
- 26.Schempf AH, Branum AM, Lukacs SL, Schoendorf KC. Maternal age and parity-associated risks of preterm birth: differences by race/ethnicity. Paediatr Perinat Epidemiol. 2007;21(1):34–43. doi: 10.1111/j.1365-3016.2007.00785.x. [DOI] [PubMed] [Google Scholar]
- 27.Fall CH, Sachdev HS, Osmond C, Restrepo-Mendez MC, Victora C, Martorell R, et al. Association between maternal age at childbirth and child and adult outcomes in the offspring: a prospective study in five low-income and middle-income countries (COHORTS collaboration) Lancet Glob Health. 2015;3(7):e366–77. doi: 10.1016/S2214-109X(15)00038-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Terada M, Matsuda Y, Ogawa M, Matsui H, Satoh S. Effects of maternal factors on birth weight in Japan. J Pregnancy. 2013;2013:172395. doi: 10.1155/2013/172395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Moon JY, Hahn WH, Shim KS, Chang JY, Bae CW. Changes of maternal age distribution in live births and incidence of low birth weight Infants in advanced maternal age group in Korea. Korean J Perinatol. 2011;22(1):30–36. [Google Scholar]
- 30.Kang BH, Moon JY, Chung SH, Choi YS, Lee KS, Chang JY, et al. Birth statistics of high birth weight infants (macrosomia) in Korea. Korean J Pediatr. 2012;55(8):280–285. doi: 10.3345/kjp.2012.55.8.280. [DOI] [PMC free article] [PubMed] [Google Scholar]