
Figure 1:
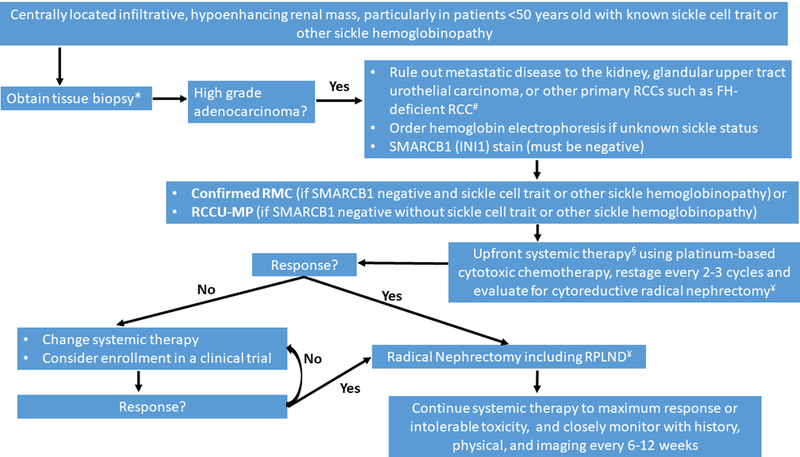
Diagnosis and management recommendations for renal medullary carcinoma (RMC) and renal cell carcinoma, unclassified with medullary phenotype (RCCU-MP). FH-deficient RCC: fumarate hydratase-deficient renal cell carcinoma; RCC: renal cell carcinoma; RPLND: retroperitoneal lymph node dissection
*Whenever possible, fresh frozen tissue should be saved for research use.
#RMC tumor tissues always contain sickled erythrocytes, often demonstrate reticular/yolk sac tumor-like patterns, and lack the tubulocystic patterns seen in FH-deficient RCCs. Secondary review of the pathology at specialized centers is strongly encouraged.
§Upfront surgery can be considered for isolated tumors ≤4 cm in greatest dimension, confined to the kidney. These patients should be followed closely post-operatively with history, physical, and imaging.
¥Cytoreductive radical nephrectomy should be considered if feasible based on response to systemic therapy, performance status, and surgical evaluation.