

Abstract
Background
The genital infection caused by Chlamydia trachomatis (CT) is a common sexually transmitted infection (STI) globally. The infection is mainly asymptomatic in women, thus it can produce infertility and chronic pelvic pain. In men infection is mainly symptomatic, but can evolve to prostatitis. Clinical practice guidelines for CT urogenital infections do not give any specific recommendation about which antibiotic use as first option
Objectives
To assess the efficacy and safety of antibiotic treatment for CT genital infection in men and non‐pregnant women.
Search methods
The Cochrane Sexually Transmitted Infections' (STI) Information Specialist developed the electronic searches in electronic databases (CENTRAL, MEDLINE, Embase and LILACS), and trials registers. We searched studies published from inception to June 2018.
Selection criteria
We included parallel, randomised controlled trials (RCTs) of men, and sexually‐active, non‐pregnant women with CT infection (urethritis or uterine cervicitis or asymptomatic), diagnosed by cell culture for CT, nucleic acid amplification tests (NAAT) or antigen‐based detection methods, who had been treated with any of the antibiotic regimens recommended by any of the updated to 2013 CT Guidelines.
Data collection and analysis
Four review authors screened evidence according to selection criteria and independently extracted data and assessed risk of bias. Two authors developed the 'Summary of findings' tables. We used a fixed‐effect meta‐analysis model for combining data where it was reasonable to assume that studies were estimating the same underlying treatment effect. We estimated the pooled risk ratio in order to establish the effects of the comparisons. Our primary outcomes were microbiological failure and adverse events, and our secondary outcomes were clinical failure, antimicrobial resistance and reinfection.
Main results
We selected 14 studies ( 2715 participants: 2147 (79.08%) men and 568 (20.92%) women). The studies were conducted mainly at STD clinics. Sample sizes ranged from 71 to 606 participants; follow‐up was 29.7 days on average.
For the comparison: azithromycin single dose versus doxycycline once or twice daily for 7 days, in men treated for CT, the risk of microbiological failure was higher in the azithromycin group (RR 2.45, 95% CI 1.36 to 4.41; participants = 821; studies = 9; moderate‐quality evidence), but regarding clinical failure, the results showed that the effect is uncertain (RR 0.94, 95% CI 0.43 to 2,05; I² = 55%; participants = 525; studies = 3; low‐quality evidence). Regarding adverse events (AE) in men there could be little or no difference between the antibiotics (RR 0.83, 95% CI 0.67 to 1.02; participants = 1424; studies = 6; low‐quality evidence). About women treated for CT, the effect on microbiological failure was uncertain (RR = 1.71, 95% CI 0.48 to 6.16; participants = 338; studies = 5; very low‐quality evidence). There were no studies assessing clinical failure or adverse events in women, however, we found that azithromycin probably has fewer adverse events in both genders (RR 0.83, 95% CI 0.71 to 0.98; I² = 0%; participants = 2261; studies = 9; moderate‐quality evidence).
For the second comparison: doxycycline compared to ofloxacin, for men treated for CT the effect on microbiological failure was uncertain (RR 8.53, 95% CI 0.43 to 167.38, I² not applicable; participants = 80; studies = 2; very low‐quality evidence), as also it was on clinical failure (RR 0.85, 95% CI 0.28 to 2.62; participants = 36; studies = 1; very low‐quality evidence). The effect of in women on clinical failure was uncertain (RR 0.94, 95% CI 0.39 to 2.25; I² = 39%; participants = 127; studies = 2; very low‐quality evidence).Regarding adverse events, the effect in both men and women was uncertain (RR 1.02 95% CI 0.66 to 1.55; participants = 339 studies = 3; very low‐quality evidence). The effect on microbiological failure in women and in men and women together was not estimable. The most frequently AE reported were not serious and of gastrointestinal origin.No studies assessed antimicrobial resistance or reinfection in either comparison.
Authors' conclusions
In men, regimens with azithromycin are probably less effective than doxycycline for microbiological failure, however, there might be little or no difference for clinical failure. For women, we are uncertain whether azithromycin compared to doxycycline increases the risk of microbiological failure. Azithromycin probably slightly reduces adverse events compared to doxycycline in men and women together but may have little difference in men alone. We are uncertain whether doxycycline compared to ofloxacin reduces microbiological failure in men or women alone, or men and women together, nor if it reduces clinical failure or adverse events in men or women.
Based on the fact that women suffer mainly asymptomatic infections, and in order to test the effectiveness and safety of the current recommendations (azithromycin, doxycycline and ofloxacin), for CT infection, especially in low and middle income countries, future RCTs should be designed and conducted to include a large enough sample size of women, and with low risk of bias. It is also important that future RCTs include adherence, CT resistance to antibiotic regimens, and risk of reinfection as outcomes to be measured. In addition, it is important to conduct a network meta‐analysis in order to evaluate all those studies that included in one arm only the current antibiotic treatments for CT infection that are recommended by the updated clinical practice guidelines.
Plain language summary
Antibiotics for treating genital Chlamydia trachomatis infection in men and non‐pregnant women
Review question
This systematic review assessed the effectiveness and safety of antibiotic treatment for Chlamydia trachomatis (CT) genital infection in terms of microbiological or clinical failure in men and non‐pregnant women.
Background
CT is the most frequent cause of urinary tract and genital infections in women and men. However, women frequently show no symptoms when they are infected. CT infection can lead to complications or cause further problems in reproductive health in women (infertility, pelvic inflammatory disease, chronic pelvic pain), and men (prostatitis (swollen prostate gland), or chronic pelvic pain. Clinical guidelines for treating CT do not recommend a preferred antibiotic treatment. This Cochrane review evaluates all randomised controlled studies (where participants are assigned at random to one of the treatments), that included antibiotics for the treatment of genital CT infection that are recommended by the most up‐to‐date clinical guidelines.
Search date
We searched for studies published up to June 2018 that provided information about failure to eliminate the CT infection or improve the symptoms, presence of adverse events, antimicrobial resistance, and reinfection. as treatment outcomes
Study characteristics
We selected 14 studies with a total of 2715 men and non‐pregnant women with CT infection, who had been treated with any antibiotic recommended by clinical guidelines (2147 (79.08%) men and 568 (20.92%) women). Women showed no symptoms or had uterine cervicitis, and men had non‐gonococcal urethritis (an inflammation of the urethra not caused by gonorrhoeal infection). All of the participants had a positive test for CT. The studies lasted from 7 to 84 days after the end of treatment, with an average of 28 days. Most of the studies took place in sexually transmitted disease clinics in the USA. Studies compared the antibiotics doxycycline with azithromycin, and doxycycline with ofloxacin.
Study funding sources
One study reported funding from academic grants, another four studies declared having received sponsorship or grants from pharmaceutical companies. The other studies declared that they were self‐funded or did not mention funding at all.
Key results (statistics)
We developed meta‐analysis (a way of combining the results of studies), for two comparisons: azithromycin 1 g single dose versus doxycycline 100 mg twice a day for seven days, and doxycycline 100 mg twice a day for seven days versus ofloxacin 300 mg to 400 mg once daily or twice daily for seven days.
We found that microbiological failure was less likely in men treated with doxycycline than men given azithromycin, and there were fewer adverse events (side effects) in men and women with azithromycin. There were no differences in clinical failure for women or men in doxycycline versus azithromycin nor in doxycycline versus ofloxacin. This means that with current available evidence, doxycycline would be the first option for treatment in men with urethritis. For non‐pregnant women with CT infections there are no advantages with any of the included antibiotics. However, clinicians could consider single‐dose azithromycin as an option, because it caused fewer adverse events.
Quality of evidence
The included studies used poor methods that could mean that their results were biased (incorrectly favouring one drug instead of the other). This means we thought that the evidence they provided for microbiological failure in men, and for adverse events in men and women when azithromycin was compared with doxycycline was moderate quality, and for all the outcomes when doxycycline was compared with ofloxacin, we thought it was very low quality.
Summary of findings
Background
Description of the condition
The genital infection caused by Chlamydia trachomatis (CT) is one of the most common sexually transmitted diseases (STDs) globally (WHO 2016). CT is an obligated intracellular bacteria, which is surrounded by a rigid wall composed by lipopolysaccharides. This bacteria is not able to synthesise adenosine triphosphate (ATP), and this makes it dependent on ATP from the host. The literature describes 19 serovars of CT. This classification is based on membrane proteins that define the site of infection: serovars A, B and C cause trachoma (a chronic eye disease), serovars D to K cause urogenital infection, and L1 to L3 are associated with venereal lymphogranuloma (Schachter 2008). The CT infection cycle begins with unprotected sexual genital contact, and elementary bodies, infectious, metabolically inert particles from CT, link to the host cell, allowing its uptake. The elementary body becomes a vacuole that differentiates into another body that is larger and has metabolic action (reticulate body), that evolves into another elementary body with infectious activity (Hogan 2004). The CT infection is asymptomatic in two‐thirds of the women infected (Stamm 2008), and symptomatic in 50% of men (O'Connell 2016).
The incidence and prevalence of CT infection varies among countries, clinical presentation and risk behaviour. In the general population the prevalence varies from 2.2% to 15.9% in women aged 20 to 34 years under screening in Europe and Africa (Bakken 2007; Eksi 2011; Lan 1995; Oakeshot 2010). In Asia, in high‐risk populations such as sex workers, prevalence varies from 17.3% in China to 23%, while in India, the prevalence in women from India who attended a reproductive health clinic was lower, at 12.2% (Chen 2013; Vishwanath 2000). Prevalence among sex workers in South America was 24.9% in Perú, 25% in Nicaragua and 53.4% in Ecuador (Carcamo 2012; Pollet 2013). Some studies in Brazil found a prevalence of 12.2% and 20.6% in adolescent asymptomatic women (De Codes 2006; Miranda 2004;Santos 2003). Indigenous women from Oaxaca, México have a prevalence of CT infection of 7.3% (Acosta‐Cazares 1996). Results from Ecuador are an example of the high variability of CT prevalence depending on the type of population: prevalence in women with cervicitis or vaginal discharge in the general population was 22.8% and among sex workers was 34.5% (Narvaez 1986). In the USA, the prevalence of CT infection in national studies was 1.6% and it was found to be higher in some ethnic groups (African American and Hispanic), (Datta 2012). Thus, according to behavioural risk factors, the frequency of CT infection is higher in sexual workers (Soto 2007), teenagers and young people (De Codes 2006), and low socio‐economic status populations (Nahmias 2011).
CT is the most frequent aetiological agent associated with urogenital tract infections such as urethritis, uterine cervicitis, epididymitis and prostatitis. Also, it is related to 40% to 60% of pelvic inflammatory diseases (Cates 1991). This infection is sexually transmitted almost exclusively, although there are reported cases of vertical infection during labour that can lead to newborn conjunctivitis (Witkin 2002). CT is also the cause of trachoma, which is the main cause of blindness around the world (Satpathy 2017). Although CT infections are often asymptomatic, in non‐pregnant women the most common clinical manifestations are vaginal discharge, vaginal bleeding, dysuria, friable cervix, pelvic pain, difficult or painful sexual intercourse, and reactive arthritis (Angel‐Müller 2012; Rodriguez 2013). The signs and symptoms in men are mainly related to urethritis (urethral itch, painful urination), testicular pain and proctitis (Mylonas 2012).
The gold standard test for diagnosis of CT infection is the nucleic acid amplification test (NAAT), due to its high sensitivity and specificity (WHO 2016). Other diagnostic methods are culture, direct fluorescence of antibodies, enzyme immunoassay and rapid or point‐of‐care tests (sensitivity above 90% and specificity +/‐ 75%) (Herbst 2016).
According to current World Health Organization (WHO), clinical practice guidelines, the management of initial infection by Neisseria gonorrhoeae, requires treatment for CT, but in CT infections, co‐treatment for N gonorrhoeae is not considered necessary (WHO 2016). This recommendation is due to rare co‐infection when CT is the main cause of symptoms: prevalence of co‐infection that ranges from 0.61% in the general population (Ginocchio 2012), to 4.4% in high‐risk men attending STD clinics (Barbosa 2010). Another co‐infection, such as Mycoplasma genitalium, may be treated with the same antibiotics as CT infection with similar effectiveness (Blanchard 2011). Prevalence of M genitalium varies from 10% to 35% in men and is less frequent in the general population (1% to 3.3%), (Jensen 2016).
Studies with a long follow‐up have found that CT urogenital infection can develop spontaneous resolution in 50% of women in their first year after infection, especially those infected with B and C serovars (Molano 2005). Also, it has been described that clinical presentation of CT infection is linked to immune response in the host and virulence of CT, which implies a wide variation of symptoms and signs in people who are infected (Geisler 2003).
When the infection is not treated complications may develop, such as upper genital tract infection or pelvic inflammatory disease in women (17% to 34.8%), with the highest frequency in adolescents (Stamm 2008). Analyses of long‐term cohorts of women infected by CT have demonstrated that repeated and untreated infections are associated with higher risk of pelvic inflammatory disease (Ness 2006). In women these infections of the upper genital tract will end in sequelae such as infertility (16%), chronic pelvic pain (29%), and ectopic pregnancy (9.1%), (Haggerty 2010). In up to 25% of the cases, chlamydial isolation has been associated with infections to the prostate (Weidner 2002), and CT has been reported in up to 30% of men with epididymitis (Zdrodowska‐Stefanow 2000).
Description of the intervention
A wide variety of antibiotics, such as tetracyclines, macrolides and quinolones are used to treat CT infection. Evidence‐based clinical guidelines such as CDC 2015, Canada 2016, Colombia STD Guidelines 2013 and WHO 2016, recommend the following antibiotic regimens:
azithromycin, 1 g orally as a single dose;
doxycycline, a long‐acting tetracycline derived from oxytetracycline, 100 mg orally twice a day for seven days;
or one of these alternatives:
tetracycline, 500 mg orally four times a day for seven days;
erythromycin, 500 mg orally four times a day for seven days;
ofloxacin, 200 mg to 400 mg orally twice a day for seven days;
levofloxacin, a fluoroquinolone, is recommended at a dose of 500 mg orally once a day for seven days.
It has been demonstrated that azithromycin is one of the most efficacious antimicrobials against CT in vitro and has a prolonged intracellular half life (Patton 2005). Tests on azithromycin at 1 g orally, single‐dose, have shown that viable CT was not recoverable in vitro after eight days of exposure, although ribonucleic acid (RNA) could be detected for up to 14 days (Dreses‐Werringloer 2001). Some guidelines recommend azithromycin 1 g, given in one dose, as the first option of treatment for non‐complicated, genital CT infection in men and non‐pregnant women (CDC 2015; Colombia STD Guidelines 2013; WHO 2016). This recommendation is based on the convenience of a single dose. The second option is doxycycline 100 mg orally twice a day for seven days, which is less expensive in some settings.
Other recommended antibiotics include erythromycin base, erythromycin ethylsuccinate, levofloxacin or ofloxacin. These alternative regimens might be less effective than either azithromycin or doxycycline, mainly because of the frequent occurrence of gastrointestinal side effects that can lead to noncompliance (CDC 2015). On the other hand, some studies have found prevalence of around 1% of resistant CT (Somani 2000). Literature reports describe isolates of CT resistant to macrolides and quinolones, however, in vitro essays have been inconclusive (Wang 2005).
How the intervention might work
Azithromycin is a semi‐synthetic antibiotic belonging to the macrolide subgroup of azalides, which binds to the 50S subunit of the 70S bacterial ribosomes and therefore inhibits RNA‐dependent protein synthesis in bacterial cells. Erythromycin acts by penetrating the bacterial cell membrane and reversibly binding to the 50S subunit of bacterial ribosomes or near the 'P' or donor site so that binding of tRNA (transfer RNA) to the donor site is blocked.
Tetracyclines act as a bacteriostatic by binding with ribosomes and thus inhibiting the bacterial protein synthesis (Lau 2002).
Quinolones are antibiotics that control CT infections by inhibiting bacterial type II topoisomerases and DNA gyrase. Ofloxacin, a quinolone/fluoroquinolone antibiotic, acts on DNA gyrase and topoisomerase IV: enzymes which, like human topoisomerase, prevent the excessive supercoiling of DNA during replication or transcription.
Why it is important to do this review
Currently, in the most up‐to‐date clinical practice guidelines, there is no clear recommendation about the preferred antibiotic regimen nor the options that should be based on efficacy/ effectiveness, safety, adherence to treatment, resistance and costs. This is evident in the current clinical practice guidelines, which recommend various regimens (Canada 2016; CDC 2015; UK Guidelines 2015). Two non‐Cochrane meta‐analyses published in 2002 and 2014, compared doxycycline with azithromycin for CT infection (Lau 2002; Kong 2014). However, it is important to determine the efficacy/effectiveness and safety of the other antibiotics recommended in the WHO CT Guideline (WHO 2016). On the other hand, no evaluation of the quality of all clinical studies related to treatment for genital CT infection has been conducted, and it is relevant to undertake a systematic review that summarises the evidence on this subject. Finally, this systematic review is relevant in order to provide evidence for policy makers, clinical guideline developers and users regarding the best option and alternative regimens for CT infection taking into account the available studies.
Objectives
To assess the efficacy and safety of antibiotic treatment for Chlamydia trachomatis (CT) genital infection in men and non‐pregnant women.
Methods
Criteria for considering studies for this review
Types of studies
We included parallel, randomised controlled trials (RCTs). Since we were looking for individual aetiological treatment for CT infection, we did not include cluster‐randomised trials. Also, since the disease is considered cured after the first treatment, we did not include cross‐over trials.
Types of participants
We selected studies that included sexually‐active men and non‐pregnant women with symptomatic (uterine cervicitis and urethritis) or asymptomatic genital CT infection diagnosed by any of the following diagnostic tests: cell culture for CT, antigen‐based detection methods, immunofluorescence test, enzyme immunoassay or nucleic acid amplification test (NAAT).
We excluded studies with the following characteristics.
Participants with co‐infection with Neisseria gonorrhoeae because of the high rate of documented resistance of this bacteria, which may had lead to changes in the response to CT treatment.
Women diagnosed with complicated infection (pelvic inflammatory disease), because treatment would have included other drugs, which may had modified the observed effectiveness.
Women and men diagnosed with any kind of immunodeficiency because their response to the treatment and comorbidity may have changed the prognosis.
Types of interventions
We considered studies with regimens of antibiotics according to the recommendations included in clinical practice guidelines from Canada 2016, CDC 2015, Colombia STD Guidelines 2013, Europe 2015, UK Guidelines 2015 and WHO 2016. The regimens found in the included studies are described below. For the meta‐analysis, we included only studies with head‐to‐head comparisons.
Azithromycin 1 g orally as a single dose (Canada 2016; CDC 2015; Colombia STD Guidelines 2013; Europe 2015; UK Guidelines 2015; WHO 2016)
Doxycycline 100 mg orally every 12 hours for seven days (Canada 2016; CDC 2015; Colombia STD Guidelines 2013; Europe 2015; UK Guidelines 2015; WHO 2016)
Ofloxacin 200 mg to 400 mg orally, daily for seven days (Canada 2016; CDC 2015; Europe 2015; UK Guidelines 2015; WHO 2016)
Tetracycline 500 mg orally, every six hours for seven days (WHO 2016)
Levofloxacin 500 mg orally, daily for seven days (CDC 2015; Europe 2015; WHO 2016)
Erithromycin 500 mg orally, every 12 hours for 10 to 14 days (CDC 2015; UK Guidelines 2015), or for seven days (Europe 2015), or 500 mg orally every six hours for seven days (Canada 2016)
We excluded Josamicin based on the fact it is only recommended by the European Guidelines as a third‐line treatment (Europe 2015).
We organised our results depending on the type of antibiotics that were compared in the included studies as follows.
Comparison 1: macrolides versus tetracyclines
Comparison 2: tetracyclines versus quinolones
Types of outcome measures
Primary outcomes
Microbiological failure: defined as a positive result for CT on any diagnostic tests after antibiotic treatment. The test was done within one to four weeks after the end of the antibiotic treatment. Diagnostic tests were cell culture for CT, antigen‐based detection methods, immunofluorescence tests, enzyme immunoassay or NAAT.
Any adverse event (AE). AEs included gastrointestinal symptoms (pyrosis or abdominal pain) or any serious or non serious systemic reactions (serious: Steven Johnson syndrome, cutaneous lupus erythematosus or erythema multiforme; non‐serious: headache, fatigue, myalgia, nausea, decrease of haemoglobin or white blood cells or platelets) during treatment.
Secondary outcomes
Clinical failure: participant reported presence of any or all the baseline symptoms after the treatment.
Antimicrobial resistance: low sensitivity to assessed antibiotics (according to measured minimal inhibitory concentration in antibiograms)
Reinfection: defined as a positive test after for weeks of treatment and evidence of microbiological cure during the first 4 weeks after treatment .
As mentioned earlier, we organised the effects of interventions according to the groups of antibiotics that were under comparison. Then, we described the outcomes of each comparison as subsections, and within those, we mentioned the particular comparisons that were addressed (e.g. comparison 1: macrolides versus tetracyclines; microbiological failure in participants treated with azithromycin 1 gram single oral dose versus doxycycline 100 mg orally twice a day for seven days).
Search methods for identification of studies
We selected studies that met the inclusion criteria irrespective of their language of publication, publication date or publication status (published, unpublished, in press and in progress).
Electronic searches
We contacted the Cochrane Sexually Transmitted Infections' Information Specialist (IS) in order to prepare a comprehensive search strategy. For this purpose, we used a combination of controlled vocabulary (MeSH, Emtree, DeCS, including exploded terms), and free‐text terms (considering spelling variants, synonyms, acronyms and truncation), for “genital Chlamydia trachomatis infection” and “antibiotics”, with field labels (title and abstract), proximity operators (adj), and boolean operators (OR, AND). The sensitivity of the search strategies was improved by including key words from relevant RCTs that had not been detected by earlier searches. The search strategies can be found in Appendix 1 and Appendix 2.
Specifically, we searched the following electronic databases:
Cochrane Sexually Transmitted Infections' Specialized Register, which includes RCTs and controlled clinical trials, from 1944 to June 2018, located through electronic searching (CENTRAL, MEDLINE and Embase ) and handsearching;
Cochrane Central Register of Controlled Trials (CENTRAL; 2017, Issue 9), Ovid platform;
MEDLINE, Ovid platform: inception to June 2018;
MEDLINE Daily Update, Ovid platform: inception to June 2018;
Embase, Ovid platform: inception to June 2018;
LILACS, IAHx interface: inception to June 2018.
For MEDLINE we used the Cochrane Highly Sensitive Search Strategy for identifying RCTs: sensitivity and precision maximizing version (2008 revision) (Lefebvre 2011). The LILACS search strategy was combined with the RCT filter of the IAHx interface.
We carried out the electronic searches initially in September 2017 and updated them in June 2018.
Searching other resources
We identified additional relevant studies by searching the following resources.
ClinicalTrials.gov
WHO International Clinical Trials Registry Platform (ICTRP) portal (apps.who.int/trialsearch/)
Web of Science: inception to June 2018.
We contacted authors of all RCTs identified by other methods.
We handsearched the following journals online: Anatolian Journal of Obstetrics & Gynecology, Current Medical Literature Gynecology & Obstetrics, Current Obstetrics and Gynecology Reports, ISRN Obstetrics and Gynecology, Journal of South Asian Federation of Obstetrics & Gynecology, Obstetrics and Gynecology International, Obstetrics Gynaecology and Reproductive Medicine, Sexual Science: the newsletter of the Society for the Scientific Study of Sexuality and Sexualities, Sexually Transmitted Infections, Sexually Transmitted Diseases
-
We handsearched conference proceedings and abstracts of the following events:
International Society for Sexually Transmitted Diseases Research (ISSTDR) (www.isstdr.org/): 2007 to June 2018;
British Association for Sexual Health and HIV (BASHH) (www.bashh.org/): 2004 to June 2018;
International Congress on Infectious Diseases (ICID) (www.isid.org/): 2010 to June 2018;
International Union against Sexually Transmitted Infections (IUSTI) (www.iusti.org/): 2011 to June 2018;
International Society for Infectious Diseases (ISID) (www.isid.org/): 2011 to June 2018;
International Meeting on Emerging Diseases and Surveillance (IMED) (imed.isid.org/): 2007 to June 2018;
Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC) (https://www.asm.org/index.php/asm‐events/post‐meeting‐materials): 2011 to June 2018;
International Federation of Gynecology and Obstetrics (FIGO) (www.figo.org/): 2012 to June 2018.
We handsearched previous systematic reviews and other relevant publications on the same topic.
We handsearched reference lists of all relevant RCTs identified by other methods.
Data collection and analysis
Selection of studies
CP, JPA and HGD independently reviewed the titles and abstracts and the full text of the selected studies. We excluded duplicate references, and documented and presented the selection process in a PRISMA flowchart (See Figure 1; Moher 2009). Reasons for exclusion are shown in Characteristics of excluded studies.
1.
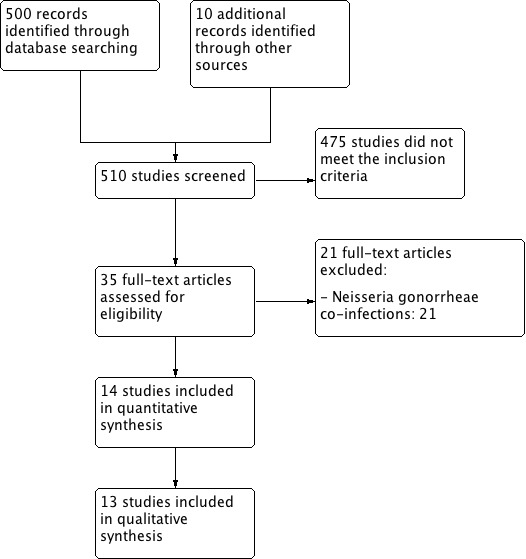
PRISMA study flow diagram
Data extraction and management
CP, JPA, JAR, HGD and LG independently collected in duplicate the most relevant study characteristics from the included studies and resolved any disagreements by discussion until we reached a consensus. We designed a data extraction form, tested it for usability, and five review authors extracted information on the following items of the data extraction form.
Methods: location of the study and setting, study design, power calculation performed
Population: inclusion and exclusion criteria, baseline information of the participants in order to have comparable intervention groups at entry (number of women, number of men, site, size, number of participants), total number of intervention groups
Interventions: types of interventions, types of comparison: number of participants enrolled and analysed, number of participants lost to follow‐up in each of the groups allocated
Outcomes: outcomes stated in methods versus outcomes reported in results, description of how secondary outcomes were measured, differences between groups for outcome assessment, time of follow‐up of participants until measured outcomes, how adverse event reports were validated, report of funding sources and ethical issues; use of signed informed consent and ethics approval
This information is presented in Appendix 3.
Assessment of risk of bias in included studies
Two review authors (CP, JPA), independently assessed the risk of bias for each included study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2017a). We solved disagreements by discussion. Those review authors who assessed risk of bias were content and methodology experts. We assessed risk of bias in the included studies and collected information in data extraction forms. We then added the information to Review Manager 5 (RevMan 5), (Review Manager 2014).
We evaluated the following topics proposed in the Cochrane Handbook for Systematic Reviews of Interventions to assess the risk of bias in the included studies.
Random sequence generation: it refers to the method of randomisation
Allocation concealment: to assess the risk of selection bias
Blinding of participants, personnel: to evaluate the possible performance bias
Blinding of outcome assessment: to evaluate the possible detection bias
Incomplete outcome data: possible attrition bias due to withdrawals, dropouts, protocol deviations
Selective outcome reporting: possible selective reporting of outcomes
Other sources of bias
Overall risk of bias
We also applied the criteria defined by Tramacere 2015 for assessing the risk of bias. To summarise the quality of the evidence we considered allocation concealment, blinding of outcome assessor and incomplete outcome data in order to classify each study as at: low risk of bias, when we judged all of the three criteria as at low risk of bias; high risk of bias, when we judged at least one criterion as at high risk of bias; unclear risk of bias, when we judged all three criteria as at unclear risk of bias; and moderate risk of bias in the remaining cases. We assessed the overall risk of bias by outcome, taking into account the number the included studies with the outcome of interest and the sample size of the study. In reference to the first seven domains above, we assessed the likely magnitude and direction of the bias and whether we considered it was likely to have an impact on the findings.
For detailed information on how we assessed the risk of bias in the included studies, please refer to Appendix 4.
Measures of treatment effect
We planned to combine results from the studies in meta‐analyses if possible; otherwise we would undertake a narrative synthesis. If meta‐analyses were feasible, we would present results for dichotomous data as summary risk ratios (RR), with 95% confidence intervals (CI), because these results are easier for clinicians to interpret. In case of continuous data, we would use the mean difference (MD), if studies measured outcomes in the same way. If studies measured the same outcomes but used different methods, we would use the standardised mean difference (SMD), to combine studies.
Unit of analysis issues
The unit of analysis was the individual with CT genital infection, confirmed by any diagnostic method, and who had been assigned to one of the treatment groups.
Analyses were conducted according to the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2017).
Dealing with missing data
Based on the fact that many of the included studies were carried out around 20 years ago, we were not able to get in touch with those investigators to request missing data. As we assessed microbiological failure as a primary outcome, we did not perform modified intention‐to‐treat analysis (analysis in symptomatic participants taking into account only positive culture or NAAT analysis).
Assessment of heterogeneity
We assessed statistical heterogeneity in each meta‐analysis using the Chi² (Deeks 2017), and I² (Higgins 2003), tests, with their correspondent P values. We considered heterogeneity to be important if the I² test was greater than 40% and either Tau² was greater than zero, or there was a low P value (less than 0.10) in the Chi² test for heterogeneity. We considered heterogeneity to be insignificant when the I² test was less than 40%. We assessed heterogeneity in prespecified subgroup analyses.
Assessment of reporting biases
In view of the difficulty of detecting and correcting for publication bias and other reporting biases, we aimed to minimise their potential impact by ensuring a comprehensive search for eligible studies and by being alert for duplication of data. If there were 10 or more studies in an outcome analysis, we used a funnel plot to explore the possibility of small study effects (a tendency for estimates of the intervention effect to be more beneficial in smaller studies), (Sterne 2017).
Data synthesis
We carried out statistical analysis using RevMan 5 software (Review Manager 2014). We used the Mantel Haenszel method and fixed‐effect model or, in case we found high heterogeneity, the random‐effects model.
We selected studies with the following comparisons taking into account macrolides as the first standard treatment and the other antibiotics as comparators. In the second comparison tetracyclines versus quinolones, tetracyclines was the standard treatment.
Macrolides (azithromycin) versus tetracyclines (doxycycline)
Tetraciclines (doxycycline) versus quinolones (ofloxacin)
Subgroup analysis and investigation of heterogeneity
Clinical presentation of CT and clinical responses to treatment differ according to sex, so we presented effects of interventions in women or men, or women and men when studies reported the outcome in both genders. We conducted one subgroup analysis by gender.
Sensitivity analysis
We carried out a sensitivity analysis restricted to studies without high risk of bias in microbiological failure and adverse events in order to establish the stability of findings. High risk of bias was defined according Tramacere 2015, described above in the risk of bias assessment section.
GRADE and 'Summary of findings' tables
We developed 'Summary of findings' tables for each comparator (Table 1; Table 2). These tables present key information for all outcomes and the rationale for our decisions on grading the quality of evidence.
Summary of findings for the main comparison. Azithromycin compared to doxycycline for treating genital Chlamydia trachomatis infection in men and non‐pregnant women.
| Comparison 1. Macrolides. Regimens with azithromycin. Azithromycin 1 g single dose versus doxycycline 100 mg twice a day for 7 days for treating genital C trachomatis infection in men and non‐pregnant women | ||||||
| Patient or population: men and non‐pregnant women with symptomatic (uterine cervicitis and urethritis), or asymptomatic genital CT infection, diagnosed by cell culture or NAAT Setting: outpatient clinic Intervention: macrolides, regimens with azithromycin 1 g single dose Comparison: doxycycline 100 mg twice a day for 7 days | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with doxycycline 100 mg twice a day for 7 days | Risk with azithromycin 1 g single dose | |||||
|
Microbiological failure Men |
33 per 1000 | 81 per 1000 (45 to 146) | RR 2.45 (1.36 to 4.41) | 821 (9 RCTs) | ⊕⊕⊕⊝ Moderatea | |
|
Microbiological failure Women |
12 per 1000 | 21 per 1000 (6 to 77) | RR 1.71 (0.48 to 6.16) | 338 (5 RCTs) | ⊕⊝⊝⊝ Very lowb,c | |
| Adverse events Men | 201 per 1000 | 167 per 1000 (135 to 205) | RR 0.83 (0.67 to 1.02) | 1424 (6 RCTs) | ⊕⊕⊝⊝ Lowd,e | |
| Adverse events Men and women | 183 per 1000 | 149 per 1000 (130 to 180) | RR 0.83 (0.71 to 0.98) | 2261 (9 RCTs) | ⊕⊕⊕⊝ Moderatea | |
|
Clinical failure Men |
123 per 1000 | 116 per 1000 (53 to 252) | RR 0.94 (0.43 to 2.05) | 525 (3 RCTs) | ⊕⊕⊝⊝ Lowd,f | |
|
Clinical failure Women |
No study in this comparison reported this outcome. | |||||
| Antimicrobial resistance | No study in this comparison reported this outcome. | |||||
| Reinfection | No study in this comparison reported this outcome. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; CT:Chlamydia trachomatis; NAAT: nucleic acid amplification tests; RCT: randomised controlled trial; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded one level for risk of bias: seven studies showed moderate risk of bias, concealment and detection were unclear; one study showed high risk of attrition bias; one study showed low risk of bias. bDowngraded one level for risk of bias: three studies showed moderate risk of bias, concealment and detection were unclear and attrition was low risk; one study showed high risk of attrition bias. cDowngraded two levels for imprecision: the 95% CI includes both effect and no effect. The sample size is lower than the optimal information size. dDowngraded one level for imprecision: the 95% CI includes both effect and no effect. eDowngraded one level for risk of bias: four of five studies were moderate risk of bias and one study was low risk of bias. fDowngraded one level for inconsistency: I² = 55%.
Summary of findings 2. Doxycycline compared to quinolones for treating genital Chlamydia trachomatis infection in men and non‐pregnant women.
| Comparison 2. Tetracyclynes. Regimens with doxycycline versus quinolones for treating genital C trachomatis infection in men and non‐pregnant women | ||||||
| Patient or population: men and non‐pregnant women with symptomatic (uterine cervicitis and urethritis), or asymptomatic genital CT infection, diagnosed by cell culture or NAAT for CT Setting: outpatient clinic Intervention: tetracyclines, regimens with doxycycline Comparison: quinolones (ofloxacin) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with quinolones | Risk with doxycycline | |||||
|
Microbiological failure Men Doxycycline 100 mg twice a day for 7 days vs ofloxacin 200 mg‐400 mg once a day for 7 days |
0 per 1000 | 0 per 1000 (0 to 0) | RR 8.53
(0.43 to 167.38) 2/27 in Doxycycline group 0/53 in Ofloxacin group |
80 (2 RCTs) |
⊕⊝⊝⊝ Very lowa,b | |
|
Microbiological failure Women Doxycycline 100 mg twice a day for 7 days vs ofloxacin 400 mg once a day for 7 days |
‐ | ‐ | Not estimable | 83 (1 RCT) |
⊕⊕⊝⊝ Lowa,c | No events in either group |
|
Microbiological failure Men and women Doxycycline 100 mg twice a day for 7 days vs ofloxacin 300 mg once a day for 7 days |
‐ | ‐ | Not estimable | 18 (1 RCT) |
⊕⊕⊝⊝ Lowa,c | 0 events in either group |
|
Adverse events
Men and women Assessed by participants' self‐report Follow‐up: range 1‐7 days |
181 per 1000 | 185 per 1000 (120 to 281) | RR 1.02 (0.66 to 1.55) | 339 (3 RCTs) | ⊕⊝⊝⊝ Very lowd,e | |
|
Clinical failure Men Doxycycline 100 mg twice a day for 7 days vs ofloxacin 400 mg once a day for 7 days Follow‐up: 8‐15 days |
320 per 1000 | 272 per 1000 (90 to 838) | RR 0.85 (0.28 to 2.62) | 36 (1 RCT) |
⊕⊝⊝⊝ Very lowb,d | |
|
Clinical failure Women Doxycycline 100 mg twice a day for 7 days vs ofloxacin 400 mg once a day for 7 days. Assessed with vaginal discharge or cervicitis Follow‐up: 8‐15 days |
141 per 1000 | 132 per 1000 (55 to 317) | RR 0.94 (0.39 to 2.25) | 127 (2 RCTs) | ⊕⊝⊝⊝ Very lowb,d | |
|
Clinical failure Men Doxycycline 100 mg twice a day for 7 days vs ofloxacin 300 mg once a day for 7 days Follow‐up: 8‐15 days |
‐ | ‐ | Not estimable | 18 (1 RCT) |
⊕⊕⊝⊝ Lowa,c | No events in either group |
| Antimicrobial resistance | No study in this comparison reported this outcome. | |||||
| Reinfection | No study in this comparison reported this outcome. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; CT:Chlamydia trachomatis; NAAT: nucleic acid amplification tests; RCT: randomised controlled trial; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded one level for risk of bias: unclear risk of bias in concealment and detection bias, high risk of attrition bias. bDowngraded two levels for imprecision: the confidence interval includes both effect and no effect. Lower sample size than optimal information size. cDowngraded one level for serious imprecision due to small sample size. dDowngraded two levels for risk of bias: two studies are high risk of bias (attrition bias), and one is unclear risk of bias (concealment and detection bias). eDowngraded one level for imprecision: the confidence interval includes both effect and no effect.
Grading the quality of evidence
We used the GRADE approach, based on the primary outcomes, microbiological failure and adverse events, and as secondary outcomes, clinical failure in all relevant comparisons. We specified four levels of quality (high, moderate, low and very low) starting from high for RCTs (Schünemann 2017a). When the included RCTs had quality flaws we downgraded the quality of evidence by one level depending on the presence of the following factors (Higgins 2017aSchünemann 2013; Schünemann 2017b).
Study limitations (risk of bias)
Inconsistency of results
Indirectness of evidence
Imprecision
Publication bias
Results
Description of studies
Results of the search
We retrieved a total of 510 references from electronic searches and other sources. After removal of duplicates and screening, 35 records were eligible for full‐text assessment. Of these, we excluded a total of 21 because they did not fulfil our inclusion criteria, all of them because participants had concurrent or previous Neisseria gonorrhoeae infection, (see Characteristics of excluded studies). Finally, we included 14 studies that met the inclusion criteria of comparisons between antibiotic regimens recommended by Clinical Guidelines (see Characteristics of included studies).
The PRISMA flow chart shows results of screening and selection of studies (see Figure 1 (Moher 2009)).
Included studies
We included 14 studies in the meta‐analysis, with a total population of 2715 (2147 men and 568 women; not all included participants presented with CT). Studies were conducted in different countries: seven of them were developed in the USA (Batteiger 1989; Geisler 2015; Hammerschlag 1993; Manhart 2013; Martin 1992; Schwebke 2011; Stamm 1995); followed by Turkey (Guven 2005; Sendag 2000), and the UK (Kitchen 1990; Lister 1993), with two studies each. The other studies took place in Brazil (Pereira 1994), Finland (Laurahanta 1993), and Iceland (Steingrímsson 1994).
Seven of the fourteen studies included only men, with a total of 564 participants (Laurahanta 1993; Lister 1993; Manhart 2013; Pereira 1994; Schwebke 2011; Stamm 1995; Steingrímsson 1994). Two studies included non‐pregnant women only (n = 96) (Guven 2005; Sendag 2000), and five studies included both men and women (n = 2217; Batteiger 1989; Geisler 2015; Hammerschlag 1993; Kitchen 1990; Martin 1992). In the last group of studies with both men and women, women represented 64% of the study population. Sample sizes ranged from 71 to 606 randomised participants.
For a detailed description of each study, see Characteristics of included studies.
Setting
All studies but one were developed by recruitment of participants in sexually transmitted disease (STD) clinics, hospitals or teaching centres for outpatient consultation, or university STD centres. One was developed in a youth correctional facility (Geisler 2015). Three studies were multicenter (Guven 2005; Hammerschlag 1993; Martin 1992).
Participants
Participants were men or women with Clamydia trachomatis (CT) genital infection. Participants' ages ranged from 17 to 60 years (27 years on average). CT infection was diagnosed in women from the urethra or uterine cervix and men from the urethra by cell culture in all studies; two studies also performed nucleic acid amplification tests (NAAT), (Geisler 2015; Manhart 2013). Since most of the participants were from STD clinics, men were mostly symptomatic for non‐gonococcal urethritis and women showed no symptoms or had uterine cervicitis. One study enrolled male and female participants aged 12 to 21 years, who were residing in four, long‐term, sex‐segregated youth correctional facilities in Los Angeles, CA, USA (Geisler 2015). One study stated that men were heterosexual (Schwebke 2011).
Interventions
Eligible interventions were based on recommendations for CT treatment in clinical guidelines updated within the last five years.
-
Macrolides (azithromycin: intervention), versus tetracyclines (doxycycline: comparator):
azithromycin 1 g, single oral dose versus doxycycline 100 mg orally twice a day for seven days (Geisler 2015; Guven 2005; Hammerschlag 1993; Laurahanta 1993; Lister 1993; Manhart 2013; Martin 1992; Schwebke 2011; Sendag 2000; Stamm 1995; Steingrímsson 1994).
-
Tetracyclines (doxycycline: intervention) versus quinolones (ofloxacin: comparator):
doxycycline 100 mg orally twice a day for seven days versus ofloxacin 300 mg twice a day for seven days (Batteiger 1989);
doxycycline 100 mg orally twice a day for seven days versus ofloxacin 400 mg once a day for seven days (Kitchen 1990);
One study included three arms (Pereira 1994). One arm received ofloxacin 200 mg twice a day for seven days, the second arm received ofloxacin 400 mg twice a day for seven days and the third arm received doxycycline 200 mg initial dose, then 100 mg twice a day for seven days. In this study, we analysed the two arms of ofloxacin together (28 participants), and we took the arm receiving doxycyline as the comparator.
It is important to mention that none of the studies compared azithromycin directly against ofloxacin.
Outcomes
Out of the five outcomes that we stated in the protocol (Types of outcome measures), we found results for three of them (microbiological failure, adverse events and clinical failure).
Most of the studies assessed the primary outcomes:
microbiological failure (Batteiger 1989; Geisler 2015; Guven 2005; Hammerschlag 1993; Kitchen 1990; Laurahanta 1993; Lister 1993; Manhart 2013; Martin 1992; Pereira 1994; Schwebke 2011; Sendag 2000; Stamm 1995; Steingrímsson 1994); or
clinical failure (Batteiger 1989; Kitchen 1990; Lister 1993; Manhart 2013; Pereira 1994; Stamm 1995).
All but one of the included studies defined microbiological failure by negative culture for CT. The remaining study used NAAT (Manhart 2013).
Studies defined clinical failure as self‐report of the presence of the same initial symptoms.
The most frequent adverse events evaluated among studies were those symptoms that developed during treatment related to the gastrointestinal system. Two studies reported participants with neurological symptoms (headache or dysaesthesia; Kitchen 1990; Laurahanta 1993).
The outcomes clinical failure and adverse events were not evaluated in women in the following comparison;
Azithromycin versus doxycycline
Doxycycline versus ofloxacin
We did not find any studies that assessed antimicrobial resistance or reinfection.
Length of follow‐up
Participants were followed up for 29.7 days on average, ranging from 10 to 42 days after the end of treatment.
Funding sources
Five studies declared having received sponsorship or grants from the pharmaceutical company that manufactured doxycycline (Hammerschlag 1993; Kitchen 1990; Martin 1992; Stamm 1995), another two declared that antibiotics were provided by Pfizer (Manhart 2013; Steingrímsson 1994). In one study, funding was given by the National Institute of Allergy and Infectious Diseases (Geisler 2015), and in another funding was from the National Institutes of Health in the USA (Schwebke 2011). The remaining studies did not declare their funding sources (Batteiger 1989; Guven 2005; Laurahanta 1993; Lister 1993; Sendag 2000).
Excluded studies
We excluded 21 studies because there was evidence of N gonorrhoeae co‐infection, diagnosed by Gram stain or subsequent culture evidence of gonococcal infection (see Characteristics of excluded studies).
Risk of bias in included studies
We have summarised our 'Risk of bias' assessment in Figure 2. We considered high risk of bias according to criteria defined by Tramacere 2015. We classified three studies as having high risk of bias (Batteiger 1989; Kitchen 1990; Martin 1992), one study as low risks of bias (Manhart 2013) and the other 10 as moderate risk of bias (see Figure 3).
2.
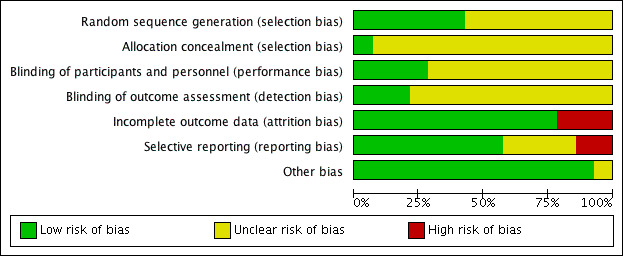
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
3.
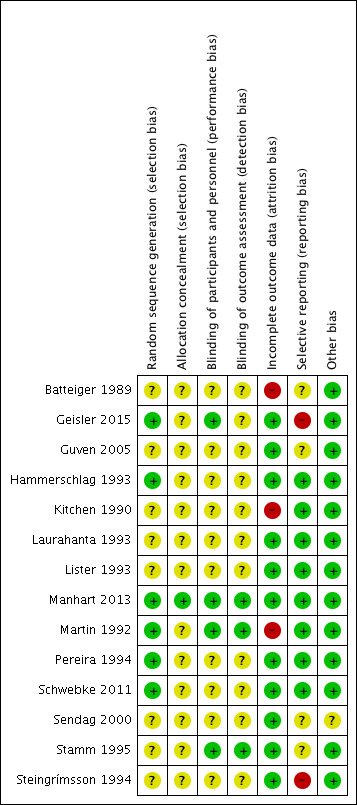
Risk of bias summary: review authors' judgements about each risk of bias item for each included study
Allocation
Random sequence generation
The studies that used adequate methods for randomisation (e.g. random number table; computer random number generation), were Geisler 2015; Hammerschlag 1993; Manhart 2013; Martin 1992; Pereira 1994 and Schwebke 2011, and we classified them as low risk of bias. Steingrímsson 1994 mentioned that they used a computer‐generated random list provided by Pfizer (unclear risk). Lister 1993 mentioned that eligible participants for the study were assigned to each therapy group according to a pre‐determined, randomised schedule; we considered the selection bias in this study to be unclear, as well as in other studies where there was insufficient information about the sequence generation process to permit judgement of high or low risk, since they only mentioned having applied randomised techniques with no further details (Batteiger 1989; Guven 2005; Kitchen 1990; Laurahanta 1993; Stamm 1995; Sendag 2000).
Allocation concealment
Two studies did not have an allocation method (Batteiger 1989; Stamm 1995) (High risk of bias). Another two reported some allocation method, or the lack of allocation did not represent a major risk of bias (Lister 1993; Manhart 2013) (Unclear and Low risk of bias respectively). The remaining studies did not report sufficient information to evaluate allocation concealment, so we judged them at unclear risk of selection bias (Geisler 2015; Guven 2005; Hammerschlag 1993; Kitchen 1990; Laurahanta 1993; Martin 1992; Pereira 1994; Schwebke 2011; Sendag 2000; Steingrímsson 1994).
Blinding
We did not find any of the studies to be high risk of bias. Three studies were blinded studies (Manhart 2013; Martin 1992; Stamm 1995), one of them mentioned placebo pills in order to complete treatment in a one‐dose regimen (azithromycin), (Stamm 1995) (low risk). The remaining 11 studies did not mention blinding of participants or personnel so we judged the risk of performance bias as unclear (Batteiger 1989; Geisler 2015; Guven 2005; Hammerschlag 1993; Kitchen 1990; Laurahanta 1993; Lister 1993; Pereira 1994; Schwebke 2011; Steingrímsson 1994; Sendag 2000).
Incomplete outcome data
We identified three studies with high risk of bias. One of them lost more than 68% of participants (Kitchen 1990), the other study reported loss of more than half of the initial population (Martin 1992), and the third one lost 26% of its participants during follow‐up (Batteiger 1989). Those studies were carried out between 1989 and 1992, thus we were not able to contact the researchers in order to ask for the missing data. The remaining studies did not report major losses in follow‐up, or the withdrawals were not significant when analysed (Geisler 2015; Guven 2005; Hammerschlag 1993; Laurahanta 1993; Lister 1993; Manhart 2013; Pereira 1994; Schwebke 2011; Sendag 2000; Stamm 1995; Steingrímsson 1994) (low risk of bias).
Selective reporting
We found two studies with high risk of reporting bias because the study authors did not include a table with the final results: in one study they did not state all results for genotyping, NAAT and outer membrane protein A stated in the methods section (Geisler 2015), and in the other study, the authors did not report all time points (1, 2 and 4 weeks after treatment) but reported solely a global estimate (Steingrímsson 1994). In two studies the bias was unclear: one of them because the study authors did not mention a previous protocol (Batteiger 1989) and the second because results were grouped and not clearly stated or presented in a table (Sendag 2000). The nine studies left were at low risk of reporting bias since all the outcomes considered in the methods section were presented in the results.
Other potential sources of bias
We did not identify any relevant sources of other bias. We looked for potential publication bias in microbiological failure in men, based on the fact that 10 studies included this outcome. We did not find risk of publication bias in the funnel plot (Figure 4).
4.
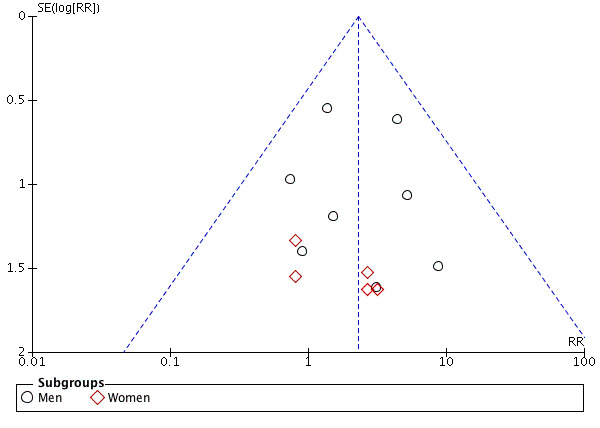
Funnel plot of comparison: 1 Macrolides. Regimens with azithromycin. Azithromycin 1 g single dose vs doxycycline 100 mg twice a day for 7 days, outcome: 1.1 Microbiological failure
Effects of interventions
Comparison 1. Macrolides versus tetracyclines
Eleven studies included the comparison 1 g single dose for azithromycin versus 100 mg doxycycline twice daily for seven days (Geisler 2015; Guven 2005; Hammerschlag 1993; Laurahanta 1993; Lister 1993; Manhart 2013; Martin 1992; Schwebke 2011; Sendag 2000; Stamm 1995; Steingrímsson 1994). We did not find studies comparing any other antibiotics than these two groups for this comparison.
1.1 Microbiological failure
Azithromycin 1 g single dose versus doxycycline 100 mg twice a day for seven days
Men
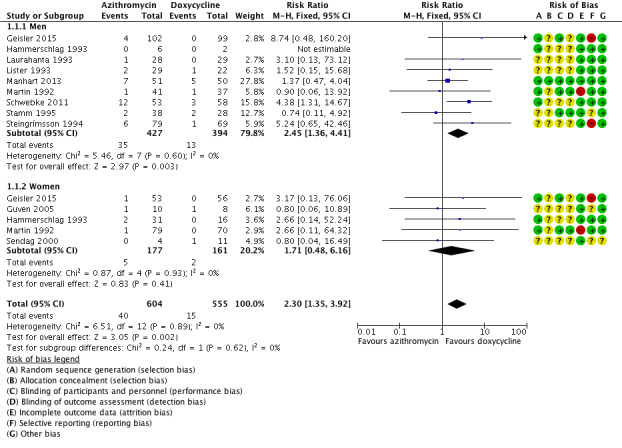
The results correspond to meta‐analysis of nine studies that included 821 participants (Geisler 2015; Hammerschlag 1993; Laurahanta 1993; Lister 1993; Manhart 2013; Martin 1992; Schwebke 2011; Stamm 1995; Steingrímsson 1994). According to the results, doxycycline probably prevents microbiological failure in men treated for CT infection (RR 2.45, 95% CI 1.36 to 4.41; participants = 821; studies = 9; I² = 0%). In other words the evidence suggests that in men with a 3% risk of failure with doxycycline, the risk of failure with azithromycin would be between 5% and 15% (Analysis 1.1; Figure 5). The quality of evidence is moderate, because one study had low risk of bias (Manhart 2013), seven studies showed moderate risk of bias and we considered one study as high risk of bias (Martin 1992). Although the 95% CI is wide, the Optimal Information Size (OIS) is enough to find 5% differences in microbiological failure.
1.1. Analysis.
Comparison 1 Macrolides. Regimens with azithromycin. Azithromycin 1 g single dose vs doxycycline 100 mg twice a day for 7 days, Outcome 1 Microbiological failure.
5.
Forest plot of comparison 1. Macrolides. Regimens with azithromycin: azithromycin 1 g single dose vs doxycycline 100 mg twice a day for 7 days, outcome: 1.1 microbiological failure
When we carried out sensitivity analysis by withdrawing the study at high risk of bias, Martin 1992, the overall effect did not change (RR 2.57, 95% CI 1.4 to 4.71).
Non‐pregnant women
The results correspond to meta‐analysis of five studies (Geisler 2015; Guven 2005; Hammerschlag 1993; Martin 1992; Sendag 2000), that included 338 participants. We found that in women treated for CT, the effect of azithromycin compared to doxycycline was uncertain in terms of microbiological failure (RR 1.71, 95% CI 0.48 to 6.16; participants = 338; studies = 5; I² = 0%).
The overall quality of evidence was low, as we classified four studies as moderate risk of bias (Geisler 2015; Guven 2005; Hammerschlag 1993; Sendag 2000), and one study had high risk of bias (attrition bias: loss to follow‐up greater than 50%; Martin 1992). There was insufficient evidence to determine whether there was a difference between the groups detected by the width of CIs, which included both no effect and appreciable benefit in both arms. On the other hand the interventions were different in relation to the appearance of the pills and the indications for taking them, with drugs in Hammerschlag 1993 and Sendag 2000 being taken on an empty stomach (Analysis 1.1; Figure 5).
When we carried out sensitivity analysis by withdrawing the study at high risk of bias, Martin 1992, the overall effect did not change (RR 1.55, 95% CI 0.38 to 6.33).
1.2 Adverse events
Azithromycin 1 g single dose versus doxycycline 100 mg twice a day for seven days
Men
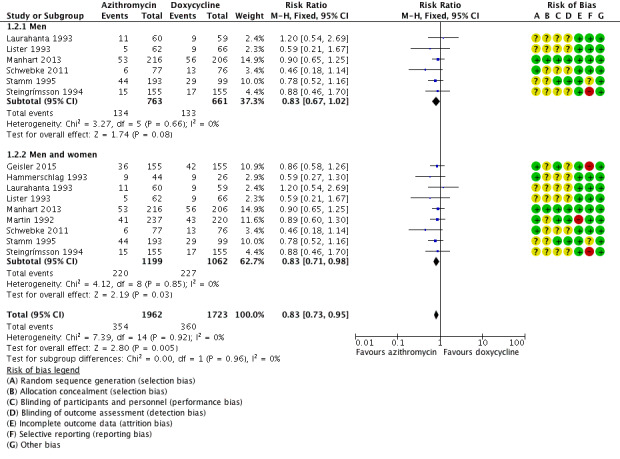
The results correspond to a meta‐analysis from six studies with 1424 men included (Laurahanta 1993; Lister 1993; Manhart 2013; Schwebke 2011; Stamm 1995; Steingrímsson 1994). The results indicate little or no difference in adverse events when men are treated with azithromycin or doxycycline (RR 0.83, 95% CI 0.67 to 1.02; participants = 1424; studies = 6; I² = 0%; Analysis 1.2; Figure 6). The overall quality of evidence is low because we considered five of the six studies as moderate risk of bias, and only one study as low risk of bias (Manhart 2013), and because of imprecision due to wide CIs that included both no effect and effect in both arms.
1.2. Analysis.
Comparison 1 Macrolides. Regimens with azithromycin. Azithromycin 1 g single dose vs doxycycline 100 mg twice a day for 7 days, Outcome 2 Adverse events.
6.
Forest plot of comparison 1. Macrolides. Regimens with azithromycin: azithromycin 1 g single dose vs doxycycline 100 mg twice a day for 7 days, outcome: 1.2 adverse events
Non‐pregnant women
None of the included studies reported results for adverse events in non‐pregnant women.
Men and women
Nine studies including 2261 participants of both sexes assessed this outcome (Geisler 2015; Hammerschlag 1993; Laurahanta 1993; Lister 1993; Manhart 2013; Martin 1992; Schwebke 2011; Stamm 1995; Steingrímsson 1994). We found that azithromycin probably has fewer adverse events compared to doxycycline, meaning that those men and women treated with azithromycin for CT had less risk of adverse events compared to those under doxycycline (RR 0.83, 95% CI 0.71 to 0.98; I² = 0%,). In other words, with doxycycline 23% of men and women would have adverse events while 19% of men and women receiving azithromycin would experience adverse events (Analysis 1.2; Figure 6). Quality of evidence was moderate because we classified one study as high risk of bias (Martin 1992).
When we carried out sensitivity analysis by withdrawing the study at high risk of bias, Martin 1992, there was no change in the effect (RR 0.82, 95% CI 0.68 to 0.98).
1.3 Clinical failure
Azithromycin 1 g single dose versus doxycycline 100 mg twice a day for seven days
Men
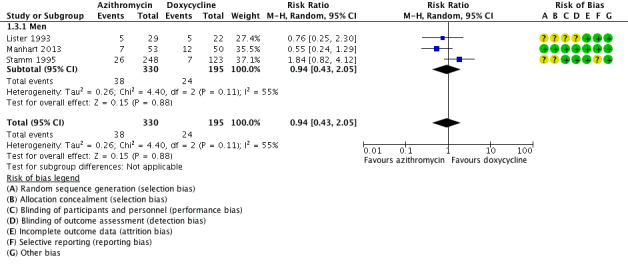
We included three studies in the meta‐analysis (Lister 1993; Manhart 2013; Stamm 1995), with 525 participants. The results indicate that there may be little or no difference in clinical failure when men are treated with azithromycin or doxycycline (RR 0.94, 95% CI 0.43 to 2.05; I² = 55% Analysis 1.3; Figure 7). We used random effects model because of the important heterogeneity. The overall quality of evidence is low because we classified one study as low risk of bias (Manhart 2013), and two studies as moderate risk of bias (Lister 1993; Stamm 1995). We also found high heterogeneity and serious imprecision related to wide CIs that include both no effect and appreciable benefit in both arms.
1.3. Analysis.
Comparison 1 Macrolides. Regimens with azithromycin. Azithromycin 1 g single dose vs doxycycline 100 mg twice a day for 7 days, Outcome 3 Clinical failure.
7.
Forest plot of comparison 1. Macrolides. Regimens with azithromycin: azithromycin 1 g single dose vs doxycycline 100 mg twice a day for 7 days, outcome: 1.3 clinical failure
Non‐pregnant women
None of the included studies reported results for clinical failure in non‐pregnant women.
1.4 Antimicrobial resistance
None of the included studies in this comparison reported this outcome.
1.5 Reinfection
None of the included studies in this comparison reported this outcome.
Comparison 2. Tetracyclines versus quinolones
2.1 Microbiological failure
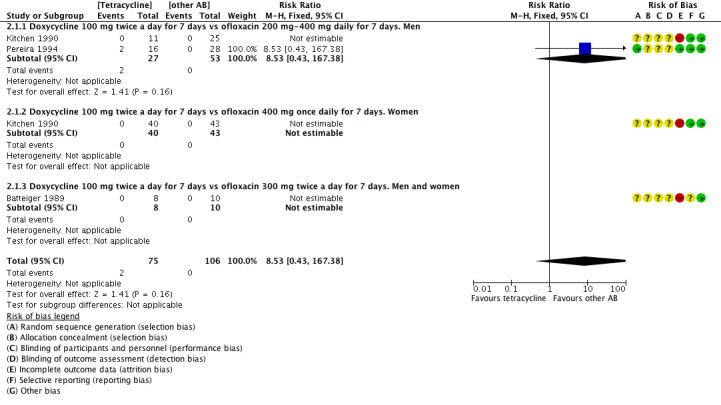
Three studies assessed this outcome (Batteiger 1989; Kitchen 1990; Pereira 1994; Analysis 2.1; Figure 8). Batteiger 1989 compared doxycycline 100 mg twice a day for seven days versus ofloxacin 300 mg twice a day for seven days, Kitchen 1990 compared doxycycline 100 mg twice a day for seven days versus ofloxacin 400 mg twice a day for seven days, and Pereira 1994 compared doxycycline 200 mg initial dose, then 100 mg twice a day for seven days against two arms that received ofloxacin 200 mg or 400 mg twice a day for seven days. We analysed those arms together.
2.1. Analysis.
Comparison 2 Tetracyclines. Regimens with doxycycline, Outcome 1 Microbiological failure.
8.
Forest plot of comparison 2. Tetracyclines. Regimens with doxycycline, outcome: 2.1 Microbiological failure
Doxycycline 100 mg twice a day for seven days versus ofloxacin 200 mg to 400 mg twice a day for seven days
Men
Two studies with 80 participants assessed this outcome in men (Kitchen 1990; Pereira 1994). We are uncertain whether doxycycline versus ofloxacin improves microbiological failure in men with CT infection (RR 8.53, 95% CI 0.43 to 167.38; participants = 80; studies = 2). In one study (Kitchen 1990), there were no failures in either of the two arms, thus the effect was not estimable (Analysis 2.1). Overall quality of evidence for this outcome is very low because of high risk of bias (attrition bias: loss to follow‐up 68%; Kitchen 1990), and very serious imprecision due to wide CIs that include both no effect and appreciable benefit in both arms.
Non‐pregnant women
We found one study that reported results for 83 women with CT urogenital infection (Kitchen 1990). In the doxycycline group there were no women reporting microbiological failure, in the same way in the ofloxacin group there were no microbiological failure, thus the overall effect is not estimable (Analysis 2.1). The quality of evidence is very low due to high risk of bias (unclear allocation concealment and detection bias, and high risk of attrition bias), and serious imprecision due to not estimable CIs.
Men and women
One study reported results for 18 participants (men and women), for doxycycline 100 mg twice a day for 7 days versus ofloxacin 300 mg once a day for seven days bus there were no events in either arm (Batteiger 1989).
2.2 Adverse events
Doxycycline 100 mg twice a day for seven days versus ofloxacin 200 mg‐400 mg twice a day for seven days
Men and women
Three studies assessed adverse events with the two mentioned antibiotic regimens (Batteiger 1989; Kitchen 1990; Pereira 1994). According to the evidence, we are uncertain whether doxycycline versus ofloxacin reduced adverse events in men and women (RR 1.02, 95% CI 0.66 to 1.55; participants = 339; studies = 3; I² = 0%; Analysis 2.2). The most common symptoms reported for each treatment were abdominal pain or nausea, or both, vomiting, tiredness and headache. The overall quality of evidence for this outcome is very low because we classified two studies high risk of bias (attrition bias: loss to follow‐up 68% (Kitchen 1990), and 26% (Batteiger 1989)), and serious imprecision due to wide CIs that include both no effect and appreciable benefit in both arms.
2.2. Analysis.
Comparison 2 Tetracyclines. Regimens with doxycycline, Outcome 2 Adverse events.
We did not perform sensitivity analysis because two studies were at high risk of bias and this would have left only Pereira 1994, that found 2/16 failures in doxycycline and 1/28 in ofloxacin
2.3 Clinical failure
This outcome was evaluated by three studies.
Doxycycline 100 mg twice a day for seven days versus ofloxacin 200 mg to 400 mg twice a day for seven days
Men
One study (Kitchen 1990), found no differences between clinical failure in men treated with these regimens (RR 0.85, 95% CI 0.28 to 2.62; participants = 36; studies = 1). Quality of evidence is very low due to high risk of bias for incomplete data in 68% of participants. There is also imprecision due to wide CIs that include both no effect and appreciable benefit in both arms and small sample size (Analysis 2.3).
2.3. Analysis.
Comparison 2 Tetracyclines. Regimens with doxycycline, Outcome 3 Clinical failure.
Non‐pregnant women
Two studies (Kitchen 1990; Pereira 1994), did not find significant differences between clinical failure in women treated with these regimens (RR 0.94, 95% CI 0.39 to 2.25; participants = 127; studies = 2). Quality of evidence is very low due to high risk of bias in one study, Kitchen 1990 (attrition bias, 32% of data only available), and also imprecision due to wide CIs that include both no effect and appreciable benefit in both arms and small sample size. We are uncertain whether doxycycline versus ofloxacin prevents clinical failure in women treated for CT infection (Analysis 2.3).
Doxycycline 100 mg twice a day for seven days versus ofloxacin 300 mg twice a day for seven days
Men
One study assessed clinical failure with this regimen (Batteiger 1989). The effect between the treatment groups was not estimable. The quality of evidence is low due to high risk of bias (attrition bias) and imprecision (wide CIs including no effect and small sample size).
2.4 Antimicrobial resistance
None of the included studies in this comparison reported this outcome.
2.5 Reinfection
None of the included studies in this comparison reported this outcome.
Discussion
Summary of main results
In the initial selection, we found a wide variety of antibiotic regimens for CT infection. As explained in Differences between protocol and review, we decided to modify the protocol in order to develop this meta‐analysis only for studies that included the antibiotic regimens recommended by the most up‐to‐date clinical practice guidelines: Canada guidelines (Canada 2016), CDC (CDC 2015), Colombian Guideline (Colombia STD Guidelines 2013), European (Europe 2015), UK (UK Guidelines 2015) and Word Health Organization (WHO 2016), because these are the main references for current CT treatment worldwide. We decided to present the results under two main comparisons according to antibiotic group: macrolides and tetracyclines, and tetracyclines versus quinolones. For macrolides, we found 11 studies that compared azithromycin 1 g single dose versus doxycycline 100 mg twice a day for seven days, and there were three studies that compared tetracyclines (doxycycline) against quinolones (ofloxacin).
We decided to organise results according to sex because CT urogenital infection presents major differences in men and women. For example, most of the infections in women are asymptomatic and this implies that records of clinical cure and relief of symptoms could differ between genders.
In terms of microbiological failure we found that in men doxycyline was more effective than azithromycin, with moderate‐quality evidence, and it had a similar effect in women but with low‐quality evidence (Analysis 1.1). Regarding the comparison between doxycyline and ofloxacin, none of the comparisons showed significant differences for these outcomes, with very low‐quality evidence for men and women alone, or for both genders together (Analysis 2.1).
When we compared azithromycin versus doxycycline the risk of adverse events was lower in men and women in the azithromycin group, with moderate‐quality evidence. However this effect disappeared when only men were considered. In general, these symptoms were gastrointestinal (nausea, vomiting and abdominal pain; Analysis 1.2). We did not find differences when we compared doxycycline versus ofloxacin in this outcome for men or women.
We did not find significant differences in clinical failure in men or women when treated with any of the regimens included in clinical practice guidelines published since 2013, with low‐quality evidence. It is important to highlight that microbiological failure was more frequently reported than clinical failure across all clinical studies (see Figure 5 and Figure 7).
Overall completeness and applicability of evidence
This review is limited, since we only included antibiotics recommended by the most up‐to‐date clinical practice guidelines, and as we only included head‐to‐head comparisons, excluding 36 studies that evaluated antibiotics not considered in those clinical practice guidelines. This reduces the body of evidence for a more precise estimation of the effect, however, a network meta‐analysis could include studies that evaluated the current clinical‐practice‐guideline‐recommended antibiotics in one arm only. It is worth remembering that many of those studies were carried out more than twenty years ago and some antibiotics may have been withdrawn due to antimicrobial resistance or high adverse effect rates and, in some cases, the antibiotics evaluated may no longer be widely available. We did not find any studies that evaluated clinical failure in women treated with azithromycin 1 g single dose or doxycycline 100 mg every 12 hours for seven days. We did not find data regarding resistance or adherence to antibiotic regimens.
Studies were conducted mostly in men (80% of participants). We found few studies that assessed all outcomes in both groups of participants (men and non‐pregnant women). We only found moderate‐quality evidence in the comparison azithromycin versus doxycycline for microbiological failure favouring doxycycline in men, and fewer adverse events in women and men favouring azithromycin. For the comparisons in women, the evidence was of low quality. Taking into account that clinical failure was not measured in women, that CT infection is mainly asymptomatic in women and results were obtained mainly in men (80%), generalisation of findings from men to women may not be appropriate.
The majority of studies were conducted with participants recruited in STD clinics or family planning clinics. It could be important to develop studies under different conditions, where asymptomatic women are more likely to attend, such as general practice, urology and gynaecology consultations.
We found that most of the studies assessed at least one of the primary outcomes (microbiological failure and adverse events). The most commonly reported adverse events were related to the gastrointestinal system.
Quality of the evidence
The quality of the evidence varies between the assessed outcomes and the comparisons: moderate‐quality evidence for microbiological failure and adverse events, when azithromycin versus doxycycline in men was compared; low‐quality evidence for microbiological failure when azithromycin versus doxycycline for women was compared; and for adverse events in men and women when doxycycline versus ofloxacin was evaluated, due to high risk of bias among studies (specially attrition bias) and imprecision (small sample sizes for most of the studies, with wide CIs that included both no effect and appreciable benefit and harm). See Table 1; Table 2. Hence, efficacy of the assessed antibiotic treatments for non‐pregnant women could be different if new analyses with high‐quality studies are performed.
We considered the criteria defined by Tramacere 2015 to assess risk of bias, as explained in Risk of bias in included studies.
Potential biases in the review process
We used systematic methods to develop this review.
As mentioned above, we did not include studies that evaluated antibiotics not considered currently for CT treatment in the up‐to‐date clinical practice guidelines, even if they were only included in one arm, and we only included head‐to‐head comparisons. Close to 80% af participants were men, thus a possible selection bias of asymptomatic women could affect the review and could affect extrapolation of the results.
Detection of microbiological failure could be affected by the use of various diagnostic tests, since the older studies used cell cultures and the most recent studies employed NAAT technologies.
We explored publication bias only for the outcome microbiological failure due to studies' characteristics.
Regarding this aspect, the funnel plot did not show publication bias for the comparison azithromycin versus doxycycline for microbiological failure in CT infection men (see Figure 4).
Agreements and disagreements with other studies or reviews
There are two non‐Cochrane reviews that assessed the effectiveness of azithromycin 1 g only dose versus doxycycline 100 mg twice daily for CT treatment (Kong 2014; Lau 2002). Our findings are consistent with Kong 2014, who showed that doxycycline was better that azithromycin for the treatment of symptomatic urethral infection in men. Lau 2002 concluded that both treatments were equally efficacious in achieving microbiological cure and the safety profile was similar; these conclusions differ from our findings.
Authors' conclusions
Implications for practice.
Regimens with azithromycin 1 g single oral dose are probably less effective than doxycycline 100 mg twice a day for seven days in men, in terms of microbiological failure. However, in men there might be little or no difference in terms of clinical failure. For women, we are uncertain whether azithromycin compared to doxycycline increases the risk of microbiological failure.
On the other hand, azithromycin probably slightly reduces adverse events compared to doxycycline, when men and women were considered together. However, when men were considered alone, there may be little or no difference between azithromycin and doxycycline in terms of adverse events. We did not find any studies that evaluated clinical failure in women, antimicrobial resistance or reinfection. We are uncertain whether doxycycline compared to ofloxacin reduces microbiological failure in men, women or women and men together nor if it reduces clinical failure or adverse events in men or women.
Implications for research.
Since we did not find any studies that assessed antimicrobial resistance, adherence to treatment or reinfection, we consider the development of studies including these outcomes to be necessary.
A network meta‐analysis could be done in order to include all those studies that have included in one of their arms only the antibiotic treatments for Clamydia trachomatis (CT) infection currently recommended by up‐to‐date clinical practice guidelines.
Since women are underrepresented in studies (20% of study population), their CT infection is mainly asymptomatic and the repercussions on sexual and reproductive health might be significant, it would be interesting to conduct studies including women in order to assess the safety and effectiveness profile of the current recommended antibiotic regimens. Also, due to new studies, it is important to assess effectiveness of treatment for anal infection. As most of the studies were conducted in the USA, response to antibiotic treatments might be different among different populations. Hence, this review has highlighted the importance of developing studies in other parts of the world.
Since azithromycin, doxycycline and ofloxacin are the recommended regimens, the assessment of antimicrobial resistance could be a high‐interest topic in CT research. Also recommended empirical CT treatment with azithromycin for women with vaginal discharge should be considered with caution, due to a possible increase of CT resistance to azithromycin or other macrolides.
Direct comparisons between azithromycin and ofloxacin are relevant for future studies. They should be conducted using high methodological standards and comparing the recommended antibiotic regimens proposed by the different guidelines for sexually transmitted diseases.
What's new
| Date | Event | Description |
|---|---|---|
| 28 February 2019 | Amended | Correction of grammatical error |
Acknowledgements
We thank the staff from the Clinical Research Institute of the School of Medicine of the National University of Colombia, and Marcela Torres and the Information Specialist from Cochrane Sexually Transmitted Infections for their support.
Also, We would like to thank Professor Nancy Santesso and Nicole Schwab for their help in full‐text acquisition and data extraction, also to Aleksandra Gara and Kerstin Mueller, for their invaluable help in translation and data extraction of non‐English articles. We would like to thank also Fernando Martínez for his contributions during the protocol stage and with selection of studies.
Appendices
Appendix 1. Electronic search strategies
CENTRAL and MEDLINE (Ovid platform)
1 exp Uterine Cervicitis/ 2 cerviciti$.tw. 3 exp Urethritis/ 4 urethritis$.tw. 5 scrotal edema.tw. 6 scrotal swelling.tw. 7 inguinal bubo$.tw. 8 exp Prostatitis/ 9 prostatiti$.tw. 10 exp Proctitis/ 11 proctiti$.tw. 12 or/1‐11 13 exp Chlamydia trachomatis/ 14 Chlam?dia trachomatis.tw. 15 or/13‐14 16 12 and 15 17 exp Lymphogranuloma Venereum/ 18 lymphogranuloma$.tw. 19 or/16‐18 20 exp Anti‐Bacterial Agents/ 21 anti bacterial$.tw. 22 antibacterial$.tw. 23 antibiotic$.tw. 24 bacteriocid$.tw. 25 bactericid$.tw. 26 exp Anti‐Infective Agents/ 27 anti infective$.tw. 28 antiinfective$.tw. 29 microbicid$.tw. 30 antimicrobial$.tw. 31 anti microbial$.tw. 32 exp Tetracyclines/ 33 exp Tetracycline/ 34 tetracyclin$.tw. 35 exp Doxycycline/ 36 doxycycline.tw. 37 exp Lymecycline/ 38 lymecycline.tw. 39 exp Minocycline/ 40 minocycline.tw. 41 exp Macrolides/ 42 macrolide$.tw. 43 exp Erythromycin/ 44 erythromycin.tw. 45 exp Clarithromycin/ 46 clarithromycin.tw. 47 exp Azithromycin/ 48 azithromycin.tw. 49 exp Quinolones/ 50 quinolone$.tw. 51 exp Ciprofloxacin/ 52 ciprofloxacin$.tw. 53 exp Ofloxacin/ 54 ofloxacin$.tw. 55 levofloxacin$.tw. 56 moxifloxacin.tw. 57 exp Fleroxacin/ 58 fleroxacin.tw. 59 exp Amoxicillin/ 60 amox?cillin$.tw. 61 exp Rifamycins/ 62 rif?mycin$.tw. 63 exp Clindamycin/ 64 clindamycin.tw. 65 exp Josamycin/ 66 josamycin.tw. 67 tosufloxacin.tw. 68 rokitamycin.tw. 69 exp Spiramycin/ 70 spiramycin.tw. 71 or/20‐70 72 randomised controlled trial.pt. 73 controlled clinical trial.pt. 74 randomized.ab. 75 placebo.ab. 76 clinical trials as topic.sh. 77 randomly.ab. 78 trial.ti. 79 or/72‐78 80 exp animals/ not humans.sh. 81 79 not 80 82 19 and 71 and 81
Note: the CENTRAL search strategy does not include the lines #72 ‐ #81.
Embase (Ovid platform)
1 exp uterine cervicitis/ 2 cerviciti$.tw. 3 cervix infection.tw. 4 cervix inflammation.tw. 5 exp urethritis/ 6 urethritis$.tw. 7 urethra$ infection.tw. 8 urethra$ inflammation.tw. 9 exp chlamydial urethritis/ 10 urogenital chlamydiasis.tw. 11 scrotal edema.tw. 12 exp scrotal swelling/ 13 scrot$ swelling.tw. 14 swollen scrotum.tw. 15 testi$ swelling.tw. 16 inguinal bubo$.tw. 17 exp prostatitis/ 18 prostatiti$.tw. 19 prostate infection.tw. 20 exp proctitis/ 21 proctiti$.tw. 22 procitis.tw. 23 rectitis.tw. 24 or/1‐23 25 exp Chlamydia trachomatis/ 26 Chlam?dia trachomatis.tw. 27 or/25‐26 28 24 and 27 29 exp lymphogranuloma venereum/ 30 lymphogranuloma$.tw. 31 lymphopathia venere$.tw. 32 frei disease.tw. 33 nicholas favre disease.tw. 34 nicolas favre disease.tw. 35 or/28‐34 36 exp antiinfective agent/ 37 antiinfective$.tw. 38 anti infective$.tw. 39 antibacterial$.tw. 40 anti bacterial$.tw. 41 antimicrobial$.tw. 42 anti microbial$.tw. 43 exp antimicrobial therapy/ 44 exp antibiotic agent/ 45 antibiotic$.tw. 46 exp bactericide/ 47 bactericid$.tw. 48 bacteriocid$.tw. 49 exp microbicide/ 50 microbicid$.tw. 51 exp tetracycline/ 52 tetracyclin$.tw. 53 exp doxycycline/ 54 doxycycline.tw. 55 exp lymecycline/ 56 lymecycline.tw. 57 exp minocycline/ 58 minocycline.tw. 59 exp macrolide/ 60 macrolide$.tw. 61 exp erythromycin/ 62 erythromycin.tw. 63 exp clarithromycin/ 64 clarithromycin.tw. 65 exp azithromycin/ 66 azithromycin.tw. 67 exp quinolone/ 68 quinolone$.tw. 69 exp ciprofloxacin/ 70 ciprofloxacin$.tw. 71 exp ofloxacin/ 72 ofloxacin$.tw. 73 exp levofloxacin/ 74 levofloxacin$.tw. 75 exp moxifloxacin/ 76 moxifloxacin.tw. 77 exp fleroxacin/ 78 fleroxacin.tw. 79 exp amoxicillin/ 80 amox?cillin$.tw. 81 exp rifamycin/ 82 rif?mycin$.tw. 83 exp clindamycin/ 84 clindamycin.tw. 85 exp josamycin/ 86 josamycin.tw. 87 exp tosufloxacin/ 88 tosufloxacin.tw. 89 exp rokitamycin/ 90 rokitamycin.tw. 91 exp spiramycin/ 92 spiramycin.tw. 93 or/36‐92 94 Clinical Trial/ 95 Randomized Controlled Trial/ 96 exp randomisation/ 97 Single Blind Procedure/ 98 Double Blind Procedure/ 99 Crossover Procedure/ 100 Placebo/ 101 Randomi?ed controlled trial$.tw. 102 Rct.tw. 103 random allocation.tw. 104 randomly allocated.tw. 105 allocated randomly.tw. 106 (allocated adj2 random).tw. 107 Single blind$.tw. 108 Double blind$.tw. 109 ((treble or triple) adj blind$).tw. 110 placebo$.tw. 111 prospective study/ 112 or/94‐111 113 case study/ 114 case report.tw. 115 abstract report/ or letter/ 116 or/113‐115 117 112 not 116 118 exp animals/ or exp invertebrate/ or animal experiment/ or animal model/ or animal tissue/ or animal cell/ or nonhuman/ 119 human/ or normal human/ or human cell/ 120 118 and 119 121 118 not 120 122 117 not 121 123 35 and 93 and 122
LILACS
(mh:("Chlamydia trachomatis")) OR (ti:("Chlamydia trachomatis")) OR (ab:("Chlamydia trachomatis")) AND db:("LILACS") AND type_of_study:("clinical_trials")
RCTs filter: ((PT:"ensayo clinico controlado aleatorio" OR PT:"ensayo clinico controlado" OR PT:"estudio multicéntrico" OR MH:"ensayos clinicos controlados aleatorios como asunto" OR MH:"ensayos clinicos controlados como asunto" OR MH:"estudios multicéntricos como asunto" OR MH:"distribución aleatoria" OR MH:"método doble ciego" OR MH:"metodo simple‐ciego") OR ((ensaio$ OR ensayo$ OR trial$) AND (azar OR acaso OR placebo OR control$ OR aleat$ OR random$ OR enmascarado$ OR simpleciego OR ((simple$ OR single OR duplo$ OR doble$ OR double$) AND (cego OR ciego OR blind OR mask))) AND clinic$)) AND NOT (MH:animales OR MH:conejos OR MH:ratones OR MH:ratas OR MH:primates OR MH:perros OR MH:gatos OR MH:porcinos OR PT:"in vitro")
Cochrane Sexually Transmitted Infection’s Specialized Register
Using the terms “Chlamydia trachomatis” and “antibiotics” in title, abstract and keywords.
WHO International Clinical Trials Registry Platform ICTRP portal
Chlamydia trachomatis OR lymphogranuloma.
ClinicalTrials.gov (CT)
"Chlamydia trachomatis" OR lymphogranuloma
Appendix 2. Electronic search strategies update
| Search electronic report 1 | |
| Search type | Update |
| Databases |
|
| Platform | Ovid |
| Search date | 19 June 2018 |
| Update date | Undefined |
| Range of search date | 2013‐Current |
| Language restrictions | None |
| Other limits | None |
| Search strategy (results) | 1 exp Uterine Cervicitis/ (2340) 2 cerviciti$.tw. (1883) 3 (cervix adj5 infection).tw. (627) 4 (cervix adj5 inflammation).tw. (68) 5 exp Urethritis/ (4527) 6 urethritis$.tw. (4470) 7 (urethra$ adj5 infection).tw. (642) 8 (urethra$ adj5 inflammation).tw. (126) 9 (scrotal adj5 edema).tw. (222) 10 (scrot$ adj5 swelling).tw. (1029) 11 (swollen adj5 scrotum).tw. (62) 12 (testi$ adj5 swelling).tw. (497) 13 (inguinal adj5 bubo$).tw. (39) 14 exp Prostatitis/ (5173) 15 prostatiti$.tw. (5347) 16 prostate ajd5 infection.tw. (0) 17 exp Proctitis/ (2922) 18 proctiti$.tw. (2300) 19 rectitis.tw. (114) 20 or/1‐19 (22233) 21 exp Chlamydia trachomatis/ (11345) 22 (chlam?dia adj5 trachomatis).tw. (12435) 23 or/21‐22 (14748) 24 20 and 23 (2282) 25 exp Lymphogranuloma Venereum/ (1534) 26 lymphogranuloma$.tw. (3660) 27 (lymphopathia adj5 venere$).tw. (27) 28 (frei adj5 disease).tw. (0) 29 (nic?olas adj5 favre adj5 disease).tw. (71) 30 (chlamydia$ adj5 urethritis).tw. (489) 31 (urogenital adj5 chlamydiasis).tw. (8) 32 or/24‐29 (6442) 33 exp Anti‐Bacterial Agents/ (652317) 34 exp Anti‐Infective Agents/ (1496828) 35 (anti adj5 infective$).tw. (3650) 36 antiinfective$.tw. (454) 37 (anti adj5 bacterial$).tw. (3591) 38 antibacterial$.tw. (61961) 39 antibiotic$.tw. (292281) 40 antimicrobial$.tw. (133640) 41 (anti adj5 microbial$).tw. (3575) 42 antibiotic$.tw. (292281) 43 bacteri?cid$.tw. (28575) 44 microbicid$.tw. (5782) 45 exp Tetracyclines/ (45625) 46 exp Tetracycline/ (19292) 47 tetracyclin$.tw. (33466) 48 exp Doxycycline/ (8874) 49 doxycycline.tw. (11929) 50 exp Lymecycline/ (118) 51 lymecycline.tw. (112) 52 exp Minocycline/ (5476) 53 minocycline.tw. (6030) 54 exp Macrolides/ (101735) 55 macrolide$.tw. (14376) 56 exp Erythromycin/ (23726) 57 erythromycin.tw. (19677) 58 exp Clarithromycin/ (5824) 59 clarithromycin.tw. (8287) 60 exp Azithromycin/ (4541) 61 azithromycin.tw. (7040) 62 exp Quinolones/ (43088) 63 exp Fluoroquinolones/ (29992) 64 quinolone$.tw. (12794) 65 fluoroquinolone$.tw. (14592) 66 exp Ciprofloxacin/ (12248) 67 ciprofloxacin$.tw. (23136) 68 exp Ofloxacin/ (6647) 69 ofloxacin$.tw. (6478) 70 exp Levofloxacin/ (2918) 71 levofloxacin$.tw. (6643) 72 moxifloxacin.tw. (4003) 73 exp Fleroxacin/ (403) 74 fleroxacin.tw. (570) 75 exp Amoxicillin/ (10497) 76 amox?cillin$.tw. (15990) 77 exp Rifamycins/ (20436) 78 rif?mycin$.tw. (1961) 79 exp Clindamycin/ (5417) 80 clindamycin.tw. (9556) 81 exp Josamycin/ (225) 82 josamycin.tw. (656) 83 tosufloxacin.tw. (268) 84 rokitamycin.tw. (185) 85 exp Spiramycin/ (685) 86 spiramycin.tw. (1223) 87 or/33‐86 (1722528) 88 randomised controlled trial.pt. (462998) 89 controlled clinical trial.pt. (92463) 90 randomized.ab. (414460) 91 placebo.ab. (189764) 92 clinical trials as topic.sh. (183960) 93 randomly.ab. (292600) 94 trial.ti. (183747) 95 or/88‐94 (1157249) 96 exp animals/ not humans.sh. (4468254) 97 95 not 96 (1065510) 98 32 and 87 and 97 (146) 99 limit 98 to yr="2013 ‐Current" (8) |
| Number of records identified | 8 |
| Search electronic report 2 | |
| Search type | Update |
| Database | Embase |
| Platform | Embase.com |
| Search date | 19 June 2018 |
| Update date | Undefined |
| Range of search date | 2013‐Current |
| Language restrictions | None |
| Other limits | None |
| Search strategy (results) | 1. 'uterine cervicitis'/exp (4480) 2. cerviciti*:ab,ti (2394) 3. (cervix NEAR/5 infection):ab,ti (777) 4. (cervix NEAR/5 inflammation):ab,ti (88) 5. 'urethritis'/exp (7412) 6. urethritis*:ab,ti (5523) 7. (urethra* NEAR/5 infection):ab,ti (940) 8. (urethra* NEAR/5 inflammation):ab,ti (170) 9. 'scrotal swelling'/exp (2180) 10. (scrotal NEAR/5 edema):ab,ti (354) 11. (scrot* NEAR/5 swelling):ab,ti (1390) 12. (swollen NEAR/5 scrotum):ab,ti (88) 13. (testi* NEAR/5 swelling):ab,ti (666) 14. (inguinal NEAR/5 bubo*):ab,ti (53) 15. 'prostatitis'/exp (9911) 16. prostatiti*:ab,ti (7340) 17. (prostate NEAR/5 infection):ab,ti (627) 18. 'proctitis'/exp (5827) 19. proctiti*:ab,ti (3999) 20. rectitis:ab,ti (209) 21. #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 (35468) 22. 'chlamydia trachomatis'/exp (17510) 23. (chlam?dia NEAR/5 trachomatis):ab,ti (14895) 24. #22 OR #23 (19830) 25. #21 AND #24 (3326) 26. 'lymphogranuloma venereum'/exp (1959) 27. lymphogranuloma*:ab,ti (4066) 28. (lymphopathia NEAR/5 venere*):ab,ti (21) 29. (frei NEAR/5 disease):ab,ti (0) 30. (nic?olas NEAR/5 favre NEAR/5 disease):ab,ti (1) 31. 'chlamydial urethritis'/exp (201) 32. (chlamydia* NEAR/5 urethritis):ab,ti (636) 33. (urogenital NEAR/5 chlamydiasis):ab,ti (16) 34. #25 OR #26 OR #27 OR #28 OR #29 OR #30 OR #31 OR #32 OR #33 (8258) 35. 'antiinfective agent'/exp (2939258) 36. 'antimicrobial therapy'/exp (183809) 37. 'antibiotic agent'/exp (1282790) 38. 'bactericide'/exp (2428) 39. 'microbicide'/exp (1784) 40. (anti NEAR/5 infective*):ab,ti (5059) 41. antiinfective*:ab,ti (937) 42. (anti NEAR/5 bacterial*):ab,ti (5532) 43. antibacterial*:ab,ti (83144) 44. antibiotic*:ab,ti (386731) 45. antimicrobial*:ab,ti (175326) 46. (anti NEAR/5 microbial*):ab,ti (5822) 47. antibiotic*:ab,ti (386731) 48. bacteri?cid*:ab,ti (695) 49. microbicid*:ab,ti (6632) 50. 'tetracycline'/exp (79026) 51. tetracyclin*:ab,ti (38866) 52. 'doxycycline'/exp (46700) 53. doxycycline:ab,ti (16759) 54. 'lymecycline'/exp (698) 55. lymecycline:ab,ti (145) 56. 'minocycline'/exp (21827) 57. minocycline:ab,ti (8066) 58. 'macrolide'/exp (204032) 59. macrolide*:ab,ti (18797) 60. 'erythromycin'/exp (70949) 61. erythromycin:ab,ti (23487) 62. 'clarithromycin'/exp (33546) 63. clarithromycin:ab,ti (12078) 64. 'azithromycin'/exp (30239) 65. azithromycin:ab,ti (10508) 66. 'quinolone'/exp (4503) 67. 'quinolone derivative'/exp (149386) 68. quinolone*:ab,ti (17190) 69. fluoroquinolone*:ab,ti (18727) 70. 'ciprofloxacin'/exp (87681) 71. ciprofloxacin*:ab,ti (31294) 72. 'ofloxacin'/exp (24537) 73. ofloxacin*:ab,ti (8565) 74. 'levofloxacin'/exp (30703) 75. levofloxacin*:ab,ti (10467) 76. 'moxifloxacin'/exp (15816) 77. moxifloxacin:ab,ti (5675) 78. 'fleroxacin'/exp (1749) 79. fleroxacin:ab,ti (786) 80. 'amoxicillin'/exp (56762) 81. amox?cillin*:ab,ti (23107) 82. 'rifamycin'/exp (3340) 83. rif?mycin*:ab,ti (2346) 84. 'clindamycin'/exp (46415) 85. clindamycin:ab,ti (12395) 86. 'josamycin'/exp (2245) 87. josamycin:ab,ti (852) 88. 'tosufloxacin'/exp (1223) 89. tosufloxacin:ab,ti (489) 90. 'rokitamycin'/exp (573) 91. rokitamycin:ab,ti (226) 92. 'spiramycin'/exp (4287) 93. spiramycin:ab,ti (1379) 94. #35 OR #36 OR #37 OR #38 OR #39 OR #40 OR #41 OR #42 OR #43 OR #44 OR #45 OR #46 OR #47 OR #48 OR #49 OR #50 OR #51 OR #52OR #53 OR #54 OR #55 OR #56 OR #57 OR #58 OR #59 OR #60 OR #61 OR #62 OR #63 OR #64 OR #65 OR #66 OR #67 OR #68 OR #69 OR #70 OR #71 OR #72 OR #73 OR #74 OR #75 OR #76 OR #77 OR #78 OR #79 OR #80 OR #81 OR #82 OR #83 OR #84 OR #85 OR #86 OR #87OR #88 OR #89 OR #90 OR #91 OR #92 OR #93 (3123002) 95. 'randomised controlled trial'/de (501265) 96. 'controlled clinical study'/de (426022) 97. random*:ti,ab (1296089) 98. 'randomisation'/de (77973) 99. 'intermethod comparison'/de (235344) 100. placebo:ti,ab (270442) 101. compare:ti AND or compared:ti AND or comparison:ti (0) 102. evaluated:ab AND or evaluate:ab AND or evaluating:ab AND or assessed:ab AND or assess:ab AND compare:ab AND or compared:ab AND or comparing:ab AND or comparison:ab (0) 103. (open NEAR/1 label):ti,ab (63938) 104. (double or single or doubly or singly NEAR/1 blind or blinded or blindly):ti,ab (0) 105. 'double blind procedure'/de (149601) 106. (parallel NEXT/1 group*):ti,ab (21512) 107. crossover:ti,ab OR 'cross over':ti,ab (92191) 108. (assign* or match or matched or allocation NEAR/5 alternate or group* or intervention* or patient* or subject* or participant*):ti,ab (0) 109. assigned or allocated:ti,ab (1) 110. (controlled NEAR/7 study or design or trial):ti,ab (0) 111. volunteer:ti,ab AND or volunteers:ti,ab (19) 112. trial:ti (250561) 113. 'human experiment'/de (406936) 114. #95 OR #96 OR #97 OR #98 OR #99 OR #100 OR #101 OR #102 OR #103 OR #104 OR #105 OR #106 OR #107 OR #108 OR #109 OR #110 OR #111 OR #112 OR #113 (2301703) 115. #34 AND #94 AND #114 (191) 116. #34 AND #94 AND #114 AND [embase]/lim AND [2013‐2018]/py (20) |
| Number of records identified | 20 |
| Search electronic report 3 | |
| Search type | Update |
| Database | The Cochrane Central Register of Controlled Trials (CENTRAL) |
| Platform | Ovid |
| Search date | 19 June 2018 |
| Update date | Undefined |
| Range of search date | 2013‐Current |
| Language restrictions | None |
| Other limits | None |
| Search strategy (results) | 1 exp Uterine Cervicitis/ (87) 2 cerviciti$.tw. (131) 3 (cervix adj5 infection).tw. (37) 4 (cervix adj5 inflammation).tw. (4) 5 exp Urethritis/ (197) 6 urethritis$.tw. (425) 7 (urethra$ adj5 infection).tw. (57) 8 (urethra$ adj5 inflammation).tw. (9) 9 (scrotal adj5 edema).tw. (18) 10 (scrot$ adj5 swelling).tw. (15) 11 (swollen adj5 scrotum).tw. (0) 12 (testi$ adj5 swelling).tw. (10) 13 (inguinal adj5 bubo$).tw. (1) 14 exp Prostatitis/ (297) 15 prostatiti$.tw. (564) 16 prostate ajd5 infection.tw. (0) 17 exp Proctitis/ (131) 18 proctiti$.tw. (296) 19 rectitis.tw. (15) 20 or/1‐19 (1643) 21 exp Chlamydia trachomatis/ (289) 22 (chlam?dia adj5 trachomatis).tw. (611) 23 or/21‐22 (670) 24 20 and 23 (151) 25 exp Lymphogranuloma Venereum/ (9) 26 lymphogranuloma$.tw. (28) 27 (lymphopathia adj5 venere$).tw. (0) 28 (frei adj5 disease).tw. (0) 29 (nic?olas adj5 favre adj5 disease).tw. (0) 30 (chlamydia$ adj5 urethritis).tw. (77) 31 (urogenital adj5 chlamydiasis).tw. (2) 32 or/24‐29 (184) 33 exp Anti‐Bacterial Agents/ (25660) 34 exp Anti‐Infective Agents/ (60436) 35 (anti adj5 infective$).tw. (196) 36 antiinfective$.tw. (28) 37 (anti adj5 bacterial$).tw. (138) 38 antibacterial$.tw. (1927) 39 antibiotic$.tw. (18212) 40 antimicrobial$.tw. (4855) 41 (anti adj5 microbial$).tw. (132) 42 antibiotic$.tw. (18212) 43 bacteri?cid$.tw. (1127) 44 microbicid$.tw. (330) 45 exp Tetracyclines/ (2249) 46 exp Tetracycline/ (757) 47 tetracyclin$.tw. (1509) 48 exp Doxycycline/ (947) 49 doxycycline.tw. (1412) 50 exp Lymecycline/ (30) 51 lymecycline.tw. (53) 52 exp Minocycline/ (437) 53 minocycline.tw. (691) 54 exp Macrolides/ (7556) 55 macrolide$.tw. (729) 56 exp Erythromycin/ (3006) 57 erythromycin.tw. (1505) 58 exp Clarithromycin/ (1313) 59 clarithromycin.tw. (2269) 60 exp Azithromycin/ (809) 61 azithromycin.tw. (1724) 62 exp Quinolones/ (4116) 63 exp Fluoroquinolones/ (3186) 64 quinolone$.tw. (496) 65 fluoroquinolone$.tw. (738) 66 exp Ciprofloxacin/ (1094) 67 ciprofloxacin$.tw. (1890) 68 exp Ofloxacin/ (939) 69 ofloxacin$.tw. (880) 70 exp Levofloxacin/ (518) 71 levofloxacin$.tw. (1020) 72 moxifloxacin.tw. (961) 73 exp Fleroxacin/ (60) 74 fleroxacin.tw. (106) 75 exp Amoxicillin/ (2527) 76 amox?cillin$.tw. (4014) 77 exp Rifamycins/ (1277) 78 rif?mycin$.tw. (100) 79 exp Clindamycin/ (812) 80 clindamycin.tw. (1254) 81 exp Josamycin/ (21) 82 josamycin.tw. (62) 83 tosufloxacin.tw. (19) 84 rokitamycin.tw. (11) 85 exp Spiramycin/ (28) 86 spiramycin.tw. (78) 87 or/33‐86 (80220) 88 32 and 87 (139) 1. 89 limit 88 to yr="2013 ‐Current" (6) |
| Number of records identified | 6 |
Appendix 3. Data extraction form ‐ information included
-
General information
Name of person extracting data
Reference citation
Study author contact details
Publication type
-
Study eligibility
Type of study
Participants
Exclusion criteria
Types of intervention
Types of comparison
Include/exclude? Reason
-
Characteristics of included studies
Methods
-
Country
Design
Was the study multicenter?
Funders of the trial
Duration of trial
Duration of participation
Ethical approval needed/obtained for study
-
Participants
Population description
Setting
Inclusion criteria
Exclusion criteria
Method of recruitment of participants
Total number randomised
Withdrawals and exclusions
Age
Sex
Race/ethnicity
Diagnostic method
-
Intervention groups
Antibiotic name
Number randomised to group
Details of the antibiotic
Dosing regimen
Mode of delivery
Co‐interventions
-
Outcomes
Outcome name
Time points measured
Time points reported
Person measuring/reporting
How was the outcome assessed?
Imputation of missing data
-
Data and analysis
Comparison
Outcome
Subgroup
Time point
Results (number of events and total in each group)
Any other results reported
Number missing participants and reason
Unit of analysis
Statistical methods used and appropriateness of these
Reanalysis required?
Reanalysis possible?
Reanalysed results
Appendix 4. Assessment of risk of bias
Random sequence generation
We qualified the method of randomisation as:
low risk of bias (the investigators describe a random component in the sequence generation process such as: random number table; computer random number generation; coin tossing, throwing dice, shuffling cards or envelopes);
high risk of bias (the investigators describe a non‐random component in the sequence generation process such as: odd or even date of birth; hospital or clinic record, number or date of admission); or
unclear risk of bias (insufficient information about the sequence generation process to permit judgement of high or low risk).
Allocation concealment (possible selection bias)
We looked for details of allocation sequence and qualified the method as:
low risk of bias (participants and investigators enrolling participants could not foresee assignment because one of the following, or an equivalent method, was used to conceal allocation: central allocation, sequentially‐numbered drug containers of identical appearance, or sequentially‐numbered, opaque, sealed envelopes);
high risk of bias (participants and investigators enrolling participants could possibly foresee assignment because one of the following methods was used: open random allocation schedule, unsealed or non‐opaque or not sequentially‐numbered envelopes, alternation or rotation, date of birth, case record number); or
unclear risk of bias (insufficient information about allocation concealment process to permit judgement of high or low risk).
Blinding of participants, personnel (possible performance bias)
We looked for blinding methods used for study participants and personnel. We considered low, high or unclear risk of performance bias for participants and for personnel involved in the trial according to the Cochrane 'Risk of bias' tool criteria.
Blinding of outcome assessment (possible detection bias)
We described the methods used, if any, to blind outcome assessors from knowledge of which intervention a participant received. We assessed blinding separately for different outcomes or classes of outcomes.
Incomplete outcome data (possible attrition bias through withdrawals, dropouts, protocol deviations)
We described the completeness of outcome data for each main outcome, including attrition and exclusion from the analysis; whether attrition and exclusion were reported; the numbers in each intervention group (compared with total of randomised participants); reasons for attrition/exclusions reported and any re‐inclusions in analyses performed by the review authors. We classified this domain according to the type of outcomes in terms of the length of follow‐up. In short‐term outcomes, such as bacteriological or clinical cure, it does not affect the assessment but in long‐term outcomes, such as complications, the potential for risk of bias will be increased. We qualify the method as:
low risk of bias (no missing outcome data; reasons for missing outcome data unlikely to be related to true outcome; missing outcome data balanced in numbers across intervention groups, with similar reasons for missing data across groups; for dichotomous data the proportion of missing outcomes compared with observed event risk not enough to have a clinically‐relevant impact on the intervention effect estimate; for continuous data, plausible effect size among missing outcomes not enough to have a clinically‐relevant impact on observed effect size; missing data have been imputed using appropriate methods);
high risk of bias (reason for missing outcome data likely to be related to true outcome; for dichotomous data the proportion of missing outcomes compared with observed event risk enough to induce clinically‐relevant bias in intervention effect estimate; for continuous data, plausible effect size among missing outcomes enough to induce clinically relevant bias in observed effect size; potentially inappropriate application of simple imputation; 'as‐treated' analysis done with substantial departure of the intervention received from that assigned at randomisation); or
unclear risk of bias (insufficient reporting of attrition/exclusion to permit judgement of high risk or low risk, or the study did not address this domain).
Selective outcome reporting: (possible selective reporting)
We qualified the method as:
low risk of bias (the study protocol was available and all of the study's pre‐specified outcomes that are of interest in the review were reported in the pre‐specified way; the study protocol was not available but it is clear that the published report includes all expected outcomes, including those that were pre‐specified).
high risk of bias (not all of the study's pre‐specified primary outcomes were reported; one or more primary outcomes were reported using measurements, analysis methods or subsets of data that were not pre‐specified. One or more reported primary outcomes were not pre‐specified, one or more outcomes of interest in the review were not completely reported so that they could not be entered in meta‐analysis; the study report failed to include results for a key outcome); or
unclear risk of bias (insufficient information to permit judgement of high risk or low risk).
Other sources of bias
We will assess any important concerns about bias not addressed in the other domains of the tool. We will qualify the method as:
low risk of bias (the study appears to be free of other sources of bias);
high risk of bias (the study had a potential source of bias related to its specific design; stopped early due to some data‐dependent process, had extreme baseline imbalance; had been claimed to have been fraudulent or some other problem); or
unclear risk of bias (insufficient information to assess whether an important risk of bias exists for this domain
Data and analyses
Comparison 1. Macrolides. Regimens with azithromycin. Azithromycin 1 g single dose vs doxycycline 100 mg twice a day for 7 days.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Microbiological failure | 11 | 1159 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.30 [1.35, 3.92] |
| 1.1 Men | 9 | 821 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.45 [1.36, 4.41] |
| 1.2 Women | 5 | 338 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.71 [0.48, 6.16] |
| 2 Adverse events | 9 | 3685 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.73, 0.95] |
| 2.1 Men | 6 | 1424 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.67, 1.02] |
| 2.2 Men and women | 9 | 2261 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.71, 0.98] |
| 3 Clinical failure | 3 | 525 | Risk Ratio (M‐H, Random, 95% CI) | 0.94 [0.43, 2.05] |
| 3.1 Men | 3 | 525 | Risk Ratio (M‐H, Random, 95% CI) | 0.94 [0.43, 2.05] |
Comparison 2. Tetracyclines. Regimens with doxycycline.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Microbiological failure | 3 | 181 | Risk Ratio (M‐H, Fixed, 95% CI) | 8.53 [0.43, 167.38] |
| 1.1 Doxycycline 100 mg twice a day for 7 days vs ofloxacin 200 mg‐400 mg daily for 7 days. Men | 2 | 80 | Risk Ratio (M‐H, Fixed, 95% CI) | 8.53 [0.43, 167.38] |
| 1.2 Doxycycline 100 mg twice a day for 7 days vs ofloxacin 400 mg once daily for 7 days. Women | 1 | 83 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 1.3 Doxycycline 100 mg twice a day for 7 days vs ofloxacin 300 mg twice a day for 7 days. Men and women | 1 | 18 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 2 Adverse events | 3 | 339 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.66, 1.55] |
| 2.1 Doxycycline 100 mg twice a day for 7 days vs ofloxacin 200 mg‐400 mg once daily for 7 days. Men and women | 3 | 339 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.66, 1.55] |
| 3 Clinical failure | 3 | 181 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.91 [0.46, 1.81] |
| 3.1 Doxycycline 100 mg twice a day for 7 days vs ofloxacin 400 mg once daily for 7 days. Men | 1 | 36 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.85 [0.28, 2.62] |
| 3.2 Doxycycline 100 mg twice a day for 7 days vs ofloxacin 400 mg once daily for 7 days. Women | 2 | 127 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.39, 2.25] |
| 3.3 Doxycycline 100 mg twice a day for 7 days vs ofloxacin 300 mg twice a day for 7 days. Men | 1 | 18 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Batteiger 1989.
| Methods | RCT | |
| Participants | 30 men and 34 women. Recruitment was in the clinic. Inclusion criteria Men: with NGU or with positive chlamydial culture and had not received therapy Women: with mucopurulent cervicitis, or with positive untreated chlamydial culture or with sexual contact with men known to have chlamydial urethritis and had not received therapy. There was a follow‐up lost of 9%. |
|
| Interventions | Doxycycline 100 mg every 12 h for 7 days (n = 26) vs ofloxacin 300 mg every 12 h for 7 d (n = 32) | |
| Outcomes | Microbiological failure (culture) Adverse events Clinical failure |
|
| Notes | Developed in the Indiana University Medical Center, USA | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of random sequence generation unclear |
| Allocation concealment (selection bias) | Unclear risk | Method not described Study published in 1989. At that time importance of concealment was not known. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Study authors did not mention blinding, however is very unlikely that absence of blinding biased results because doses and tablets were similar. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Study authors did not mention blinding, however is very unlikely that absence of blinding biased results because doses and tablets were similar. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Lost of 26% of participants for all outcomes |
| Selective reporting (reporting bias) | Unclear risk | Sexual re‐infection risk after treatment in non‐cured participants, specially in 21‐28 d post treatment. No protocol available |
| Other bias | Low risk | Unclear risk. ITT analysis ‐ unclear; baseline characteristics ‐ not described |
Geisler 2015.
| Methods | RCT | |
| Participants | Male and female participants aged 12‐21 years who were residing in 4 long‐term, sex‐segregated youth correctional facilities in Los Angeles, CA, USA. Inclusion criteria: study staff recruited residents who had a positive screening NAAT result and, after obtaining written informed consent, reviewed the eligibility criteria and enrolled eligible residents. Exclusion criteria: pregnancy, breast‐feeding, gonorrhoea coinfection, allergy to tetracyclines or macrolides, previous photosensitivity from doxycycline, an inability to swallow pills, receipt of an antibiotic with anti‐chlamydial activity within 21 d before screening or between screening and enrolment, concomitant infection requiring treatment with an antibiotic agent that had anti‐chlamydial activity, and pelvic inflammatory disease or epididymitis. The population randomised was 567 patients. They were mainly African American (44%) compared to white (33%). |
|
| Interventions | Azithromycin 1 g single dose (n = 284) or doxycycline 100 mg twice daily for 7 d (n = 283). Both treatments were taken under supervision. |
|
| Outcomes | Failure to respond to treatment (microbiological failure) | |
| Notes | The study drugs were purchased from a pharmacy in Los Angeles with study funds from the National Institute of Allergy and Infectious Diseases. The study was approved by the institutional review board at the University of Alabama at Birmingham and at the County of Los Angeles Public Health Department, as well as by the Superior Court of California County of Los Angeles Juvenile Division, the County of Los Angeles Probation Department, and Office for Human Research Protections, Department of Health and Human Services. Diagnostic test was NAAT to screen for chlamydia (APTIMA Combo 2, Gen‐Probe), routinely performed on first‐catch urine specimens obtained from residents of Los Angeles County youth correctional facilities at intake. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants were randomly assigned, in a 1:1 ratio, with the use of a block randomisation scheme (with randomisation performed separately within each facility), to receive the CDC‐recommended azithromycin regimen or doxycycline regimen |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment method not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Although regimens were different, it was not a cause of different results because of the type of test used for assessment of failure (NAAT) |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Study authors did not mention if there was blinding for outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Per protocol analysis, similar losses in follow‐up in both groups |
| Selective reporting (reporting bias) | High risk | Study authors did not include a table with the final results, they did not state all results for genotyping, NAAT and outer membrane protein A |
| Other bias | Low risk | ‐ |
Guven 2005.
| Methods | RCT | |
| Participants | Participants were sexually active, non‐pregnant women of reproductive age or early menopause (range 18–52 years). Inclusion criteria: women who attended clinics due to various symptoms. Exclusion criteria: treatment with another antimicrobial agent within the previous 2 weeks; known hypersensitivity to macrolides or tetracyclines Total number randomised: 81 women. |
|
| Interventions | Azithromycin 1 g single dose (Zitrotek, Pfizer), taken in the clinic as 2 x 500 mg tablets on an empty stomach (n = 41) and Doxycycline 100 mg twice daily for 7 days (n = 40) | |
| Outcomes | Microbiological failure measured by culture | |
| Notes | The study developed took place from February 2002 to February 2003. This was a multicentre study, in gynaecology STD clinics: Kahramanmaras Sutcuimam University, Faculty of Medicine, Kahramanmaras and Ankara Zekai Tahir Burak Teaching Hospital, Obstetrics and Gynecology clinics, Turkey | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Processs not detailed |
| Allocation concealment (selection bias) | Unclear risk | Processs not detailed |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Regimens were different and that could lead to performance bias. Study authors did not mention blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Regimens were different. Study authors did not mention blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No significant losses between the groups. |
| Selective reporting (reporting bias) | Unclear risk | No previous protocol |
| Other bias | Low risk | No sources of other bias |
Hammerschlag 1993.
| Methods | RCT | |
| Participants | Adolescent men and women, 15‐20 years of age, seen in adolescent gynaecology clinics. Inclusion criteria: patients with chlamydial infection, provided they were not pregnant or nursing and had not taken antibiotics within the 72 h before entry into the study. Exclusion criteria: significant hepatic, renal, cardiac, or hematologic diseases, known allergy to the study drugs, and evidence of gonococcal pharyngitis, proctitis, or disseminated gonococcal infection Total number of randomised: 73 |
|
| Interventions | Azithromycin 1 g single dose (n = 46) vs doxycycline 100 mg twice/d for 7 d (n = 27) | |
| Outcomes | Microbiological failure measured by culture, adverse events | |
| Notes | The study was multicentre, included patients from Kings County Hospital Center, Brooklyn, N.Y. USA, the Brookdale Hospital Medical Center, Brooklyn, and the adolescent clinic at the University of Alabama at Birmingham. Study dates April 1990‐July 1992 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was clear, the study authors used a randomisation table |
| Allocation concealment (selection bias) | Unclear risk | Authors did not state if they used a method for allocation concealment |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No mention of blinding |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Study authors did not mention blinding of outcome assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low losses among the groups |
| Selective reporting (reporting bias) | Low risk | All initial outcomes were reported. |
| Other bias | Low risk | ‐ |
Kitchen 1990.
| Methods | Parallel RCT | |
| Participants | Men and women, recruited by invitation when attending the clinic, even thought this was not clearly stated in the document Inclusion criteria Men aged 18‐52 years, who presented with symptoms suggestive of a new episode of NGU. Women aged 18‐50 years with a positive test for chlamydial infection of the cervix in the absence of concurrent gonococcal or trichomonal infection. Exclusion criteria Men with a concurrent gonococcal or trichomonal infection, those who had received antibiotic therapy within the previous week, those who had concurrent systemic illness or past history of allergy to any antibacterial agent or patients with epilepsy Women who were pregnant or not using reliable contraceptive measures, women who were breast‐feeding and patients with clinical evidence of pelvic inflammatory disease All of them were seen in St. Mary's Hospital in the UK. Total number randomised: 282 (182 men and 100 women). This value includes all participants even though eventual diagnosis of Chlamydia was not confirmed in all of them (specially men). |
|
| Interventions | Doxicyclin 100 mg twice/d for 7 d (n = 140, 90 men and 50 women) vs ofloxacin 400 mg/d for 7 days (n = 142, 92 men and 50 women) | |
| Outcomes | Microbiological failure based on negative tests of chlamydial infection at both follow‐up visits. The laboratory test was a test detecting C. trachomatis in urethral or endocervical samples by means of a direct immunofluorescent monoclonal antibody technique (MicroTrak‐Syva). Clinical failure Adverse events: recorded after spontaneous reporting by the participant. Its relation to the study therapy was assessed by the attending clinician. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Methods for randomisation are not clearly stated: Quote: “Male and female patients were randomised separately for treatment over seven days….” |
| Allocation concealment (selection bias) | Unclear risk | Study authors mention randomisation but not a description of method |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Study authors mention “blinding in evaluation” and no further description |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Study authors mention “blinding in evaluation” and no further description |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Large follow‐up losses (more than 68%) In men they state that: “Results of efficacy were evaluable for 153 patients attending for follow up on completion of the treatment, that is 78 patients in the ofloxacin group and 75 in the doxycycline group. Default rates were similar for each group” In women they state that: “Forty three patients in the ofloxacin group and 40 patients in the doxycycline group were evaluable for efficacy of treatment…” Comment: reasons for not attending were not included in the female groups, loss to follow‐up was considerable. |
| Selective reporting (reporting bias) | Low risk | All the outcomes that were initially considered were reported, even though presentation was not very clear. |
| Other bias | Low risk | ‐ |
Laurahanta 1993.
| Methods | Parallel RCT | |
| Participants | Symptomatic male patients aged 18‐60 years with NGU with ≥ 4 white blood cells in urethral smear. Inclusion criteria: male patients (18‐60 years old) with signs and symptoms compatible with non‐gonococcal urethritis (dysuria, urethral irritation or discharge, or with at least four WBC (White Blood Cells)/high‐power field on microscopy of a methylene blue stained urethral smear) Exclusion criteria
Total number randomised was 120, but CT was isolated in only 63. |
|
| Interventions | Azithromycin 1 g single dose (n = 60) vs doxycycline 100 mg twice/d for 7 d (n = 60) | |
| Outcomes | Microbiological failure assessed by CT culture Adverse events |
|
| Notes | Seems that the study was carried out in the Helsinki University Central Hospital, Finland, only. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study authors did not mention randomisation method |
| Allocation concealment (selection bias) | Unclear risk | Study authors did not mention allocation method |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Only one participant was missing from the adverse events evaluation |
| Selective reporting (reporting bias) | Low risk | All the pre‐specified outcomes were presented in the results |
| Other bias | Low risk | ‐ |
Lister 1993.
| Methods | Parallel RCT | |
| Participants | Men aged ≥ 18 years attending at the Department of Genito‐Urinary medicine at the University College Hospital, London. Mean age was 29.5 years old, range 19‐57 Inclusion criteria: symptoms and/or signs of NGU (discharge, dysuria or urethral irritation) and with ≥ 5 polymorphonuclear leucocytes. Exclusion criteria: Gram‐negative intracellular diplococci in the urethral smear, or who had received treatment with another antimicrobial agent within 2 weeks of enrolment, or who had other associated infections requiring treatment with another antimicrobial agent in addition to the study drug, or who were allergic to macrolides or tetracyclines. Total number of men randomised was 143. |
|
| Interventions | Azithromycin 1 g single dose (n = 72) vs doxycycline 100 mg twice/d for 7 d (n = 71) | |
| Outcomes | Microbiological failure Clinical failure Adverse events |
|
| Notes | The study took place from June 1990‐October 1991. The setting was the department of Genito‐Urinary medicine at the University College Hospital, London. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients who were eligible for the study were assigned to each therapy group according to a pre‐determined randomised schedule” |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: ”This was an open comparative study…” Comment: Even thought it was open, the microbiological cure did not pose a threat to the evaluation of the outcome. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Study authors stated that the study was open. For microbiological cure, it is not a problem. Adverse events can be affected by the type of study, but there were no significant differences among groups. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No significant losses |
| Selective reporting (reporting bias) | Low risk | All the proposed objectives were presented in the article. |
| Other bias | Low risk | ‐ |
Manhart 2013.
| Methods | Parallel‐group, superiority study | |
| Participants | Men ≥ 16 years old with NGU Inclusion criteria: visible urethral discharge on examination or ≥ 5 polymorphonuclear leukocytes per high‐power field (PMNs/HPF) on a Gram‐stained slide of urethral exudates. English‐speaking, attending the Public Health Seattle & King County STD Clinic in Seattle, WA, USA. Exclusion criteria: men who had received antibiotics in the past month or had allergies to study drugs Total number randomised: 606 |
|
| Interventions | Azithromycin 1 g single dose (n = 304) vs doxycycline 100 mg twice/d for 7 d (n = 302) | |
| Outcomes | Microbiological failure assessed by culture and NAAT Clinical failure |
|
| Notes | Funders of the study: National Institute of Health: National Institute of Allergy and Infectious diseases and the National Cancer Institute. Pfizer, Inc, provided the study drugs. The study took place in the USA |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation and blinding were managed by the Harborview Medical Center Investigational Drug Service (HMC IDS), using Excel to generate the random sequence in blocks of 10 |
| Allocation concealment (selection bias) | Low risk | HMC IDS prepared sequentially numbered treatment packets in sealed, opaque envelopes; treatment arm was assigned when the clinician gave the participant the next numbered packet in the sequence. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | All participants, clinicians, and study staff were blinded to treatment assignment until the end of the study. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All participants, clinicians, and study staff were blinded to treatment assignment until the end of the study. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | They presented the analysis of modified ITT, and also presented the sensitivity analysis |
| Selective reporting (reporting bias) | Low risk | All the outcomes stated in the objectives were included in the report |
| Other bias | Low risk | ‐ |
Martin 1992.
| Methods | Parallel RCT | |
| Participants | Men and women with positive CT rapid test and cultures recruited from STD, college‐student health, adolescent health and family‐planning clinics in USA Inclusion criteria: presumptive chlamydial urethral and/or endocervical infection Exclusion criteria: evidence of gonococcal pharyngitis, proctitis, or disseminated gonococcal infection; treatment with a systemic antibiotic within 72 h before enrolment; evidence of salpingitis or epididymitis; history of allergy or hypersensitivity to erythromycin or doxycycline; history of a serious underlying chronic disease; a positive test for hepatitis B surface antigen; and known alcohol or drug abuse. Patients who were pregnant or lactating were also excluded. Total number randomised: 457 |
|
| Interventions | Azithromycin 1 g single dose (n = 237) vs doxycycline 100 mg twice/d for 7 d (n = 220) | |
| Outcomes | Microbiological failure assessed by culture for CT Adverse events |
|
| Notes | The study took place in USA. Funded by Pfizer Central Research | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The study authors used a randomisation table. |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Although the study was not blind for the participants, and no clear information was available for blinding of personnel in charge of evaluating this outcome, due to its nature it is unlikely that it influenced the measurement of outcomes. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: “Placebos were not used” Quote: “The drugs were distributed by a person who was not involved in the selection or evaluation of the patients” |
| Incomplete outcome data (attrition bias) All outcomes | High risk | The number of people evaluated at the last measurement was less than half of the initial sample of participants for this outcome |
| Selective reporting (reporting bias) | Low risk | All the pre‐specified outcomes presented in the objectives and methods were included |
| Other bias | Low risk | ‐ |
Pereira 1994.
| Methods | Parallel RCT. 3 arms | |
| Participants | Men aged 18‐40 years, attending STD clinic Inclusion criteria: symptomatic with urethral discharge and microbiological confirmation of CT infection 44 patients randomised |
|
| Interventions | Doxycycline 200 mg initial dose then 100 mg twice/d for 7 d (n = 16) vs ofloxacin 200 mg‐400 mg twice/d for 7 d (n = 28) | |
| Outcomes | Microbiological failure Clinical failure Adverse events |
|
| Notes | The study was conducted in Brazil. It was not multicentric. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation by using a list of random numbers |
| Allocation concealment (selection bias) | Unclear risk | Study authors did not mention details of the allocation concealment. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low losses |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported |
| Other bias | Low risk | ‐ |
Schwebke 2011.
| Methods | Parallel RCT | |
| Participants | Heterosexual men 16–45 years of age who attended STD clinics in Birmingham, Alabama; New Orleans, Louisiana; Durham, North Carolina; and Baltimore, Maryland, USA. Exclusion criteria: a test result positive for gonorrhoea at the baseline visit; history of recurrent NGU (> 3 episodes within the previous year) or history of recent NGU (within the previous 30 days); signs or symptoms of epididymitis or prostatitis; known allergy to study drugs; receipt of systemic antibiotics within 30 days of enrolment; presence of concomitant infection that required antibiotics; unwillingness to abstain from alcohol for 24 h after enrolment; serious underlying infection, including known HIV infection or other primary or secondary immunosuppression; or voided within the hour preceding evaluation Total number randomised: 305 Age 20‐32 years old. Race mainly African American |
|
| Interventions | Azithromycin 1 g (n = 156) vs doxycycline 100 mg twice/d for 7 d (n = 149) | |
| Outcomes | Microbiological failure assessed by (NAAT) GEN‐PROBE TMA assay (Aptima Combo II; Gen‐Probe) Adverse events |
|
| Notes | The study was conducted in United States. It was multicentre: STD clinics in Birmingham, Alabama; New Orleans, Louisiana; Durham, North Carolina; and Baltimore, Maryland, USA Founders of the study: National Institute of Health (DMID contract number N01AI40073C), North Carolina Sexually Transmitted Infections and Topical Microbicides Cooperative Research Center (grant U19‐AI31496). The first participant was enrolled in November 2006, and the last follow‐up visit was completed in April 2009. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised using a block randomisation scheme with blocks of size 16 stratified by clinical centre |
| Allocation concealment (selection bias) | Unclear risk | Study authors did not mention allocation concealment method |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Its not clear how doxycycline treatment was blinded. There is no mention of participants receiving placebo to mask the administration of doxycycline for 7 days |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It was not clearly mentioned how and when microbiological cure or adverse events were evaluated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low losses in both arms |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported |
| Other bias | Low risk | ‐ |
Sendag 2000.
| Methods | Parallel RCT | |
| Participants | 131 women (15 women with CT), Turkey Inclusion criteria: signs and symptoms compatible with Mucopurulent cervicitis (MPC) (purulent endocervical discharge, oedema, erythema and friability of the zone of ectopy) Exclusion criteria: treatment with another antimicrobial agent within the previous 2 weeks, known hypersensitivity to macrolides and tetracyclines, evidence of any gastrointestinal condition that might affect study drug administration and presence of diplococci in the Gram stain of the cervical smear |
|
| Interventions | Azithromycin 1 g single dose taken in the clinic as 2 x 500 mg tablets on an empty stomach (n = 4) or 100 mg doxycycline twice daily for 7 d (n = 11) | |
| Outcomes | Microbiological failure: (cure (disappearance of all baseline signs), improvement (reduction without complete disappearance of baseline signs), failure (no improvement and reinfection unlikely. i.e. no new sexual contact). The participants with baseline cultures positive for CT, Ureaplasma urealyticum and Mycoplasma hominis were assessed for their microbiological response as follows: eradication, eradication with recurrence and persistence. Adverse events: at each visit the possible side effects were recorded |
|
| Notes | 15/131 (11.45%) participants were culture positive for CT | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "The patients were randomly allocated to receive either a 1 g single dose of azithromycin (Zitrotek. Pfizer) taken in the clinic as two 500 mg tablets on an empty stomach or 100 mg doxycycline (Tetradox. Fako) twice daily for 7 days." |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | The numbers lost to follow‐up were similar in both groups and < 20% |
| Selective reporting (reporting bias) | Unclear risk | The study authors did not mention a protocol. |
| Other bias | Unclear risk | The methods section did not mention the sample size calculation and the procedures of the participants |
Stamm 1995.
| Methods | Parallel RCT | |
| Participants | Male outpatients aged ≥ 18 years Inclusion criteria: typical symptoms of urethritis Exclusion criteria: Gram's stain or subsequent culture evidence of gonococcal infection; other significant systemic disease; a urological abnormality; known HIV infection; allergy to erythromycin or doxycycline; necessity for treatment with another antibiotic; treatment with an investigational drug in the last 30 days; antimicrobial therapy in the last 2 weeks; or a gastrointestinal condition that would likely affect drug absorption. The ethnicity was mainly African American (77%) Total number randomised: 452 |
|
| Interventions | Azithrhomycin 1 g, single dose (n = 38) vs doxycycline 100 mg twice/d for 7 d (n = 28) | |
| Outcomes | Microbiological failure: assessed by urethral swabs obtained for a Gram's stain, culture for NG and CT Clinical failure Adverse events |
|
| Notes | The study was conducted in USA, funded by Pfizer. Multicentre, involving 11 STD clinics | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Participants were randomly allocated to receive either azithromycin or doxycycline, with a 2:1 randomisation ratio" |
| Allocation concealment (selection bias) | Unclear risk | Not stated. Neither the investigator nor the participant was aware of the medication assigned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Neither the investigator nor the participant was aware of the medication assigned. Quote: "Participants allocated to receive azithromycin received four 250‐mg capsules as a single dose on day 1 and 2 doxycycline placebo tablets, 1 taken in the morning and 1 in the afternoon, on day 1. Subsequently, doxycycline placebo tablets were taken twice daily for the next 6 days. Participants treated with doxycycline received 4 azithromycin placebo capsules on day 1 and 100 mg of doxycycline taken in the morning and in the afternoon on day 1 and for 6 days thereafter". |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Neither the investigator nor the participant was aware of the medication assigned. Same tests at recruitment were performed at each visit to classify individuals. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | The numbers lost to follow‐up were similar in both groups and < 20% |
| Selective reporting (reporting bias) | Unclear risk | They did not mention a protocol. Results were grouped and were not clearly stated or presented in a table. |
| Other bias | Low risk | ‐ |
Steingrímsson 1994.
| Methods | Parallel RCT | |
| Participants | 148 men that went to a STD clinic consultation in Iceland for symptoms of urethritis. Diagnostic method was urethral cultures Total number randomised: 148 The age range was 16‐48 years. Median 22 years old |
|
| Interventions | Azithromycin 1 g (4 tablets 250 mg) only dose oral (n = 79) vs doxycycline 100 mg twice/d for 7 d (n = 69) | |
| Outcomes | Microbiological failure: measured by urethral cultures for CT | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study authors mention “random assigned by use of a computer generated randomised list provided by Pfizer”. Pfizer was the manufacturer of one of the interventions |
| Allocation concealment (selection bias) | Unclear risk | Study authors did not mention any method for allocation concealment. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | It is unclear the meaning of the statement “Third party blinding”. Regimens were different and that can lead to performance bias. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Study authors did not mention blinding for outcome assessment. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No significant losses. |
| Selective reporting (reporting bias) | High risk | Study authors did not report all time points (1, 2 and 4 weeks after treatment), just a global estimate. |
| Other bias | Low risk | ‐ |
CT: Chlamydia trachomatis; ITT: intention‐to‐treat; MPC: Mucopurulent cervicitis; NAAT: nucleic acid amplification tests; NG:Neisseria gonorrhoea; NGU: non‐gonococcal urethritis; RCT: randomised controlled trial; STD: sexually transmitted diseases; WBC: White Blood Cells
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Boslego 1988 | NG co‐infection |
| Bowie 1989 | NG co‐infection |
| Bowie 1993 | NG co‐infection |
| Csango 1984 | NG co‐infection |
| Csango 1985 | NG co‐infection |
| Cummings 1989 | NG co‐infection |
| Evans 1990 | Postgonococcal infection |
| Faro 1991 | NG co‐infection |
| Hongyao 2000 | NG co‐infection |
| Lassus 1988 | NG co‐infection |
| Lassus 1990 | NG co‐infection |
| McLean 1990 | Study about post‐gonococcal urethritis |
| Morel 1996 | NG co‐infection |
| Paavonen 1989 | NG co‐infection |
| Reedy 1997 | NG co‐infection |
| Stamm 1984 | NG co‐infection |
| Stolz 1986 | NG co‐infection |
| Thorpe 1996 | NG co‐infection |
| Tio 1990 | NG co‐infection |
| Van Schouwenburg 1992 | Mycoplasma hominis co‐infection, results not reported separately |
| Wagenvoort 1987 | NG co‐infection |
NG: Neisseria gonorrhoeae
Differences between protocol and review
We changed the protocol (Paez‐Canro 2013), in May 2017 in order to include only antibiotics that are currently recommended by the clinical practice guidelines updated since 2013: Canada 2016, CDC 2015, Colombia STD Guidelines 2013, Europe 2015, UK Guidelines 2015 and WHO 2016 and modified the text accordingly.
The title was changed from Antibiotics for treating genital chlamydia trachomatis infection in men and non‐pregnant women to "Antibiotics for treating urogenital Chlamydia trachomatis infection in men and non‐pregnant women"
To make the results easier for clinicians to interpret, we made the following changes.
-
We redefined the outcomes in the following way:
-
Primary outcome
We renamed microbiological cure as microbiological failure defined as a positive result for CT on any diagnostic tests after antibiotic treatment. The test was done within one to four weeks after the end of the antibiotic treatment. Diagnostic tests were cell culture for CT, antigen‐based detection methods, immunofluorescence tests, enzyme immunoassay or NAAT.
-
Secondary outcome:
We renamed clinical cure as clinical failure. Participants self‐reported clinical failure as either complete (presence of baseline symptoms after the treatment), or partial (incomplete recovery from initial symptoms or reduction of the baseline symptoms after the treatment).
-
For meta‐analysis, we excluded studies in which a drug regimen was compared with a different regimen of the same drug.
We included 'Summary of findings' tables in the review.
Contributions of authors
Páez‐Canro C, Alzate JP independently developed studies selection, Páez‐Canro C, Alzate JP, Rubio J, Gonzalez L and Gaitan H developed extraction data. Páez‐Canro C, Gaitan H, Alzate JP and Gonzalez L wrote the review draft. Gaitan H, González L, Rubio J and Lethaby A commented and revised the manuscript draft.
Sources of support
Internal sources
No financial support, Other.
External sources
No sources of support supplied
Declarations of interest
Carol Páez‐Canro: none declared Juan Pablo Alzate: none declared Lina M González: none declared Jorge Andres Rubio‐Romero: none declared Anne Lethaby: none declared Hernando G Gaitán: none declared
Edited (no change to conclusions)
References
References to studies included in this review
Batteiger 1989 {published data only}
- Batteiger BE, Jones RB, White A. Efficacy and safety of ofloxacin in the treatment of nongonococcal sexually transmitted disease. American Journal of Medicine 1989;87(6C):75S‐S. [PubMed] [Google Scholar]
Geisler 2015 {published data only}
- Geisler WM, Uniyal A, Lee JY, Lensing SY, Johnson S, Perry RC, et al. Azithromycin versus doxycycline for urogenital Chlamydia trachomatis infection. New England Journal of Medicine 2015;24:2512‐21. [DOI] [PMC free article] [PubMed] [Google Scholar]
Guven 2005 {published data only}
- Guven MA. The demographic and behavioural profile of women with cervicitis infected with Chlamydia trachomatis, Mycoplasma hominis and Ureaplasma urealyticum and the comparison of two medical regimens. Archives of Gynecology and Obstetrics 2005;272:197‐200. [DOI] [PubMed] [Google Scholar]
Hammerschlag 1993 {published data only}
- Hammerschlag M. Single dose of azithromycin for the treatment of genital chlamydial infections in adolescents. Journal of Pediatrics 1993;6:961‐5. [DOI] [PubMed] [Google Scholar]
Kitchen 1990 {published data only}
- Kitchen VS, Donegan C, Ward H, Thomas B, Harris JR, Taylor‐Robinson D. Comparison of ofloxacin with doxycycline in the treatment of non‐gonococcal urethritis and cervical chlamydial infection. Journal of Antimicrobial Chemotherapy 1990;26:99‐105. [DOI] [PubMed] [Google Scholar]
Laurahanta 1993 {published data only}
- Lauharanta J, Saarinen K, Mustonen MT, Happonen HP. Single‐dose oral azithromycin versus seven‐day doxycycline in the treatment of non‐gonococcal urethritis in males. Journal of Antimicrobial Chemotherapy 1993;31:177‐83. [DOI] [PubMed] [Google Scholar]
Lister 1993 {published data only}
- Lister PJ, Balechandran T, Ridgway GL, Robinson AJ. Comparison of azithromycin and doxycycline in the treatment of non‐gonococcal urethritis in men. Journal of Antimicrobial Chemotherapy 1993;31:185‐92. [DOI] [PubMed] [Google Scholar]
Manhart 2013 {published data only}
- Manhart LE, Gillespie CW, Lowens MS, Khosropour CM, Colombara DV, Golden MR, et al. Standard treatment regimens for nongonococcal urethritis have similar but declining cure rates: a randomized controlled trial. Clinical Infectious Diseases 2013;56(7):934‐42. [DOI] [PMC free article] [PubMed] [Google Scholar]
Martin 1992 {published data only}
- Martin DH, Mroczkowski TF, Dalu ZA, McCarty J, Jones RB, Hopkins SJ, et al. A controlled trial of a single dose of azithromycin for the treatment of chlamydial urethritis and cervicitis. The Azithromycin for Chlamydial Infections Study Group. New England Journal of Medicine 1992;327(13):921‐5. [DOI] [PubMed] [Google Scholar]
Pereira 1994 {published data only}
- Pereira CA, Montagnini SD. A prospective randomized trial of ofloxacin vs. doxycycline in the treatment of nongonococcal urethritis caused by Chlamydia trachomatis. Arquivos Brasileiros de Medicina 1994;68(1):51‐3. [Google Scholar]
Schwebke 2011 {published data only}
- Schwebke JR, Rompalo A, Taylor S, Sena AC, Martin DH, Lopez LM, et al. Re‐evaluating the treatment of nongonococcal urethritis: emphasizing emerging pathogens‐‐a randomized clinical trial. Clinical Infectious Diseases 2011;52(2):163‐70. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sendag 2000 {published data only}
- Sendag F, Terek C, Tuncay G, Ozkinay E, Guven M. Single dose oral azithromycin versus seven day doxycycline in the treatment of non‐gonococcal mucopurulent endocervicitis. Australian & New Zealand Journal of Obstetrics & Gynaecology 2000;40:40‐7. [DOI] [PubMed] [Google Scholar]
Stamm 1995 {published data only}
- Stamm WE, Hicks CB, Martin DH, Leone P, Hook EW, Cooper RH, et al. Azithromycin for empirical treatment of the nongonococcal urethritis syndrome in men. A randomized double‐blind study. JAMA 1995;274(7):545‐9. [PubMed] [Google Scholar]
Steingrímsson 1994 {published data only}
- Steingrímsson O, Olafsson JH, Thorarinsson H, Ryan RW, Johnson RB, Tilton RC. Single dose azithromycin treatment of gonorrhea and infections caused by C. trachomatis and U. urealyticum in men. Sexually Transmitted Diseases 1994;21:43‐6. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Boslego 1988 {published data only}
- Boslego JW, Hicks CB, Greenup R, Thomas RJ, Wiener HA, Ciak J, et al. A prospective randomized trial of ofloxacin vs. doxycycline in the treatment of uncomplicated male urethritis. Sexually Transmitted Diseases 1988;15(4):186‐91. [DOI] [PubMed] [Google Scholar]
Bowie 1989 {published data only}
- Bowie WR, Willetts V, Megran DW. Dose‐ranging study of fleroxacin for treatment of uncomplicated Chlamydia trachomatis genital infections. Antimicrobial Agents and Chemotherapy 1989;33(10):1774‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bowie 1993 {published data only}
- Bowie WR, Willetts V, Binns BA, Brunham RC. Etiology of cervicitis and treatment with minocycline. Canadian Journal of Infectious Diseases 1993;4(2):95‐100. [DOI] [PMC free article] [PubMed] [Google Scholar]
Csango 1984 {published data only}
- Csango PA, Salveson A, Gundersen T, Jagars G, Bjerk O. Treatment of acute gonococcal urethritis in men with simultaneous infection with Chlamydia trachomatis. British Journal of Venereal Diseases 1984;60(2):95‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Csango 1985 {published data only}
- Csango PA, Gundersen T, Martinsen IM. Effect of amoxicillin on simultaneous Chlamydia trachomatis infection in men with gonococcal urethritis: comparison of three dosage regimens. Sexually Transmitted Diseases 1985;12(2):93‐6. [DOI] [PubMed] [Google Scholar]
Cummings 1989 {published data only}
- Cummings M, Benes S, Draft K, McCormack WM. Evaluation of difloxacin in the treatment of uncomplicated urethral gonorrhea in men. Antimicrobial Agents & Chemotherapy 1989;33(10):1721‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Evans 1990 {published data only}
- Evans BA, Lim JM, Azadin BS. Postgonococcal urethritis: a double‐blind study of doxycycline vs placebo. Genitourinary Medicine 1990;66(1):20‐23. [DOI] [PMC free article] [PubMed] [Google Scholar]
Faro 1991 {published data only}
- Faro S, Martens MG, Maccato M, Hammill HA, Roberts S, Riddle G. Effectiveness of ofloxacin in the treatment of Chlamydia trachomatis and Neisseria gonorrhoeae cervical infection. American Journal of Obstetrics and Gynecology 1991;164:1380‐3. [DOI] [PubMed] [Google Scholar]
Hongyao 2000 {published data only}
- Hongyao L, Xiaoming C, Zhenguo M, Jingping W, Haixiao W, Xuezhi L. Evaluation of treatment in gonococcal urethritis complicated with Chlamydia trachomatis by sparfloxacin. Chinese Journal of Antibiotics 2000;25(2):154‐5+60. [Google Scholar]
Lassus 1988 {published data only}
- Lassus A, Renkonen OV, Ellmen J. Fleroxacin versus standard therapy in gonococcal urethritis. Journal of Antimicrobial Chemotherapy 1988;22:223‐35. [DOI] [PubMed] [Google Scholar]
Lassus 1990 {published data only}
- Lassus A. Comparative studies of azithromycin in skin and soft‐tissue infections and sexually transmitted infections by Neisseria and Chlamydia species. Journal of Antimicrobial Chemotherapy 1990;25:115‐21. [DOI] [PubMed] [Google Scholar]
McLean 1990 {published data only}
- McLean KA, Evans BA, Lim JM, Azadin BS. Postgonococcal urethritis: a double‐blind study of doxycycline vs placebo. Genitourinary Medicine 1990;66(1):20‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Morel 1996 {published data only}
- Morel P, Gianotti B, Barlow D, Phillips I, Jean C. Comparative efficacy and safety of single oral doses of sparfloxacin versus ciprofloxacin in the treatment of acute gonococcal urethritis in men. Journal of Antimicrobial Chemotherapy 1996;37(Suppl A):115‐22. [DOI] [PubMed] [Google Scholar]
Paavonen 1989 {published data only}
- Paavonen J, Roberts PL, Stevens CE, Wolner‐Hanssen P, Brunham RC, Hillier S, et al. Randomized treatment of mucopurulent cervicitis with doxycycline or amoxicillin. American Journal of Obstetrics and Gynecology 1989;161(1):128‐35. [DOI] [PubMed] [Google Scholar]
Reedy 1997 {published data only}
- Reedy MB, Sulak PJ, Miller SL, Ortiz M, Kasberg‐Preece C, Kuehl TJ. Evaluation of 3‐day course of doxycycline for the treatment of uncomplicated Chlamydia trachomatis cervicitis. Infectious Disease in Obstetrics and Gynecology 1997;5(1):18‐22. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stamm 1984 {published data only}
- Stamm WE, Guinan ME, Johnson C, Starcher T, Holmes KK, McCormack WM. Effect of treatment regimens for Neisseria gonorrhoeae on simultaneous infection with Chlamydia trachomatis. New England Journal of Medicine 1984;310(9):545‐9. [DOI] [PubMed] [Google Scholar]
Stolz 1986 {published data only}
- Stolz E, Tegelberg‐Stassen MJ, Willigen AH, Hoek JC, Joost T, Mooi L, et al. Quinolones in the treatment of gonorrhoea and Chlamydia trachomatis infections. Pharmaceutisch Weekblad 1986;8(1):60‐2. [DOI] [PubMed] [Google Scholar]
Thorpe 1996 {published data only}
- Thorpe EM Jr, Stamm WE, Hook EW 3rd, Gall SA, Jones RB, Henry K, et al. Chlamydial cervicitis and urethritis: single dose treatment compared with doxycycline for seven days in community based practises. Genitourinary Medicine 1996;72(2):93‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Tio 1990 {published data only}
- Tio TT, Sindhunata IR, Wagenvoort JH, Angulo AF, Habbema L, Michel MF, et al. Pefloxacin compared with cefotaxime for treating men with uncomplicated gonococcal urethritis. Journal of Antimicrobial Chemotherapy 1990;26:141‐6. [DOI] [PubMed] [Google Scholar]
Van Schouwenburg 1992 {published data only}
- Schouwenburg J, Bruyn O, Fourie E, Rensburg J, Rodriques A, Pickard I. A randomized, comparative study of the efficacy and tolerance of roxithromycin and doxycycline in the treatment of women with positive endocervical cultures for Chlamydia trachomatis and Mycoplasma spp. in an in vitro fertilization program. Diagnostic Microbiology and Infectious Disease 1992;15(4 Suppl):129S‐31S. [DOI] [PubMed] [Google Scholar]
Wagenvoort 1987 {published data only}
- Wagenvoort JH, Willigen AH. Quinolones in the treatment of gonorrhoea and Chlamydia trachomatis infections. Pharmaceutisch Weekblad 1987;9(Suppl):S82‐6. [DOI] [PubMed] [Google Scholar]
Additional references
Acosta‐Cazares 1996
- Acosta‐Cazares B, Ruiz‐Maya L, Escobedo de la Pena J. Prevalence and risk factors for Chlamydia trachomatis infection in low‐income rural and suburban populations of Mexico. Sexually Transmitted Diseases 1996;23(4):283‐8. [DOI] [PubMed] [Google Scholar]
Angel‐Müller 2012
- Angel‐Müller E, Rodríguez A, Núñez‐Forero LM, Moyano LF, González P, Osorio E, et al. The prevalence of and factors associated with C. trachomatis, N. gonorrhoeae, T. vaginalis, C. albicans infection, syphilis, HIV and bacterial vaginosis in females suffering lower genital tract infection symptoms in three healthcare attention sites in Bogotá, Colombia, 2010. Revista Colombiana de Obstetricia y Ginecologia 2012;63(1):14‐24. [Google Scholar]
Bakken 2007
- Bakken IJ, Skjeldestad FE, Nordbø SA. Chlamydia trachomatis infections increase the risk for ectopic pregnancy: a population‐based, nested case‐control study. Sexually Transmitted Diseases 2007;34(3):166‐9. [DOI] [PubMed] [Google Scholar]
Barbosa 2010
- Barbosa MJ, Moherdaui F, Pinto VM, Ribeiro D, Cleuton M, Miranda AE. Prevalence of Neisseria gonorrhoeae and Chlamydia trachomatis infection in men attending STD clinics in Brazil [Prevalência de Neisseria gonorrhoeae e infecção pela Chlamydia trachomatis em homens atendidos em clínicas de DST no Brasil]. Revista da Sociedade Brasileira de Medicina Tropical 2010;43(5):500‐3. [DOI] [PubMed] [Google Scholar]
Blanchard 2011
- Blanchard A, Bébéar C. The evolution of Mycoplasma genitalium. Annals of the New York Academy of Sciences 2011;1230(1):E61‐4. [DOI] [PubMed] [Google Scholar]
Canada 2016
- Public Health Agency of Canada. Canadian Guidelines on Sexually Transmitted Infections. www.canada.ca/en/public‐health/services/infectious‐diseases/sexual‐health‐sexually‐transmitted‐infections/canadian‐guidelines/sexually‐transmitted‐infections.html 2016; Vol. 1:1.
Carcamo 2012
- Carcamo CP, Campos PE, Garcia, PJ, Hughes JP, Garnett GP, Holmes KK, et al. Prevalences of sexually transmitted infections in young adults and female sex sex workers in Peru: a national population‐based survey. Lancet Infectious Diseases 2012;12(10):765‐73. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cates 1991
- Cates W Jr, Wasserheit JN. Genital chlamydial infections: epidemiology and reproductive sequelae. American Journal of Obstetrics and Gynecology 1991;164:1771‐81. [DOI] [PubMed] [Google Scholar]
CDC 2015
- Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines, 2015. www.cdc.gov/std/tg2015/chlamydia.htm 2015;1:1. [Google Scholar]
Chen 2013
- Chen X‐S, Yin Y‐P, Liang G‐J, Wang Q‐Q, Jiang N, Liu Q, et al. The prevalences of Neisseria gonorrhoeae and Chlamydia trachomatis infections among female sex workers in China. BMC Public Health 2013;13:121. [DOI] [PMC free article] [PubMed] [Google Scholar]
Colombia STD Guidelines 2013
- Gaitán‐Duarte H, Rodriguez‐Hernandez A, Arévalo‐Rodríguez I, Angel‐Müller E, López‐Ramos H, Estrada‐Mesa S, et al. Clinical practice guideline for syndromic management of patients with sexually transmitted infections and other genital tract infections ‐ 2013 [Guía de práctica clínica para el manejo sindrómico de los pacientes con infecciones de transmisión sexual y otras infecciones del tracto genital ‐ 2013]. Revista Colombiana de Obstetricia y Ginecología 2013;64(2):126‐77. [Google Scholar]
Datta 2012
- Datta SD, Torrone E, Kruszon‐Moran D, Berman S, Johnson R, et al. Chlamydia trachomatis trends in the United States among persons 14 to 39 years of age, 1999–2008. Sexually Transmitted Diseases 2012;39:92‐6. [DOI] [PubMed] [Google Scholar]
De Codes 2006
- Codes JS, Cohen DA, Almeida de Melo N, Gonzaga G, dos Santos A, Silva T, et al. Detection of sexually transmitted diseases in clinical and non‐clinical settings in the City of Salvador, Bahia, Brazil [Detecção de doenças sexualmente transmissíveis em ambientes clínicos e não clínicos na Cidade de Salvador, Bahia, Brasil]. Cad Saúde Pública Rio de Janeiro 2006;22:325‐34. [DOI] [PubMed] [Google Scholar]
Deeks 2017
- Deeks JJ, Higgins JP, Altman DG (editors), on behalf of the Cochrane Statistical Methods Group. Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). The Cochrane Collaboration, 2017. Available from www.training.cochrane.org/handbook.
Dreses‐Werringloer 2001
- Dreses‐Werringloer U, Padubrin I, Zeidler H, Köhler L. Effects of azithromycin and rifampin on Chlamydia trachomatis infection in vitro. Antimicrobial Agents and Chemotherapy 2001;45:3001‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Eksi 2011
- Eksi F, Dikensoy E, Gayyurhan ED, Balci I, Balat O, Karsligil T, et al. The prevalence of Chlamydia trachomatis and Neisseria gonorrhoeae in the endocervical swab specimens of symptomatic, asymptomatic and infertile women in Turkey. Archives of Gynecology and Obstetrics 2011;283(6):1349‐56. [DOI] [PubMed] [Google Scholar]
Europe 2015
- Lanjouw E, Ouburg S, Vries HJ, Stary A, Radcliffe K, Unemo M. 2015 European guideline on the management of Chlamydia trachomatis infections. International Journal of STD & AIDS 2015;0:1‐16. [DOI] [PubMed] [Google Scholar]
Geisler 2003
- Geisler WM, Suchland RJ, Whittington WL, Stamm WE. The relationship of serovar to clinical manifestations of urogenital Chlamydia trachomatis infection. Sexually Transmitted Diseases 30;2:160‐5. [DOI] [PubMed] [Google Scholar]
Ginocchio 2012
- Ginocchio CC, Chapin K, Smith JS, Aslanzadeh J, Snook J, Hill CS, et al. Prevalence of Trichomonas vaginalis and coinfection with Chlamydia trachomatis and Neisseria gonorrhoeae in the United States as determined by the Aptima Trichomonas vaginalis nucleic acid amplification assay. Journal of Clinical Microbiology 2012;50(8):2601‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Haggerty 2010
- Haggerty CL, Gottlieb SL, Taylor BD, Low N, Xu F, Ness RB. Risk of sequelae after Chlamydia trachomatis genital infection in women. Journal of Infectious Diseases 2010;201 Suppl 2:S134‐55. [DOI] [PubMed] [Google Scholar]
Herbst 2016
- Herbst de Cortina S, Bristow CC, Joseph Davey D, Klausner JD. A systematic review of point of care testing for Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis. Infectious Diseases in Obstetrics and Gynecology 2016;2016:4386127. [PUBMED: 27313440] [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2017a
- Higgins JP, Altman DG, Sterne JA (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Hogan 2004
- Hogan RJ, Mathews SA, Mukhopadhyay S, Summersgill JT, Timms P. Chlamydial persistence: beyond the biphasic paradigm. Infection and Immunity 2004;72(4):1843‐55. [DOI] [PMC free article] [PubMed] [Google Scholar]
Jensen 2016
- Jensen JS, Cusini M, Gomberg M, Moi H. 2016 European guideline on Mycoplasma genitalium infections. Journal of the European Academy of Dermatology and Venereology : JEADV 2016;30(10):1650‐6. [PUBMED: 27505296] [DOI] [PubMed] [Google Scholar]
Kong 2014
- Kong F, Tabrizi S, Law M, Vodstrcil LA, Chen M, Fairley CK, et al. Azithromycin versus doxycycline for the treatment of genital chlamydia infection: a meta‐analysis of randomized controlled trials. Clinical Infectious Diseases 2014;59(2):193‐205. [DOI] [PubMed] [Google Scholar]
Lan 1995
- Lan J, Melgers I, Meijer CJ, Walboomers JM, Roosendaal R, Burger C, et al. Prevalence and serovar distribution of asymptomatic cervical Chlamydia trachomatis infections as determined by highly sensitive PCR. Journal of Clinical Microbiology 1995;33(12):3194‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lau 2002
- Lau CY, Qureshi AK. Azithromycin versus doxycycline for genital chlamydial infections: a meta‐analysis of randomized clinical trials. Sexually Transmitted Diseases 2002;29:497‐502. [DOI] [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Miranda 2004
- Miranda AE, Szwarcwald CL, Peres RL, Page‐Shafer K. Prevalence and risk behaviors for chlamydial infection in a population‐based study of female adolescents in Brazil. Sexually Transmitted Diseases 2004;31(9):542‐6. [DOI] [PubMed] [Google Scholar]
Moher 2009
- Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred reporting items for systematic reviews and meta‐analyses: the PRISMA Statement. PLoS Medicine 6;7:e1000097. [DOI: 10.1371/journal.pmed1000097] [DOI] [PMC free article] [PubMed] [Google Scholar]
Molano 2005
- Molano M, Meijer CJ, Weiderpass E, Arslan A, Posso H, Franceschi S, et al. The natural course of Chlamydia trachomatis infection in asymptomatic Colombian women: a 5‐year follow‐up study. Journal of Infectious Diseases 2005;191(6):907‐16. [DOI] [PubMed] [Google Scholar]
Mylonas 2012
- Mylonas I. Female genital Chlamydia trachomatis infection: where are we heading?. Archives of Gynecology and Obstetrics 2012;285:1271‐85. [DOI] [PubMed] [Google Scholar]
Nahmias 2011
- Nahmias SB, Nahmias D. Society, sex, and STIs: human behavior and the evolution of sexually transmitted diseases and their agents. Annals of the New York Academy of Sciences 2011;1230:59‐73. [DOI] [PubMed] [Google Scholar]
Narvaez 1986
- Narváez M, Izurieta A, Tello S, López Jaramillo P, Escobar L, Guevara A, et al. Prevalence of cervicitis by Chlamydia trachomatis in Ecuador [Prevalencia de cervicitis por Chlamydia trachomatis en Ecuador]. Revista de la Facultad de Ciencias Médicas 1986;11:5‐8. [Google Scholar]
Ness 2006
- Ness RB, Smith KJ, Chang CC, Schisterman EF, Bass DC. Prediction of pelvic inflammatory disease among young, single, sexually active women. Sexually Transmitted Diseases 2006;33:137‐42. [DOI] [PubMed] [Google Scholar]
O'Connell 2016
- O'Connell CM, Ferone ME. Chlamydia trachomatis genital infections. Microbial Cell 2016;3(9):390‐403. [PUBMED: 28357377] [DOI] [PMC free article] [PubMed] [Google Scholar]
Oakeshot 2010
- Oakeshott P. Randomised controlled trial of screening for Chlamydia trachomatis to prevent pelvic inflammatory disease: the POPI (prevention of pelvic infection) trial. BMJ 2010;340:c1642. [DOI] [PMC free article] [PubMed] [Google Scholar]
Patton 2005
- Patton DL, Sweeney YTC, Stamm WE. Significant reduction in inflammatory response in the macaque model of chlamydial pelvic inflammatory disease with azithromycin treatment. Journal of Infectious Diseases 2005;192:129‐35. [DOI] [PubMed] [Google Scholar]
Pollet 2013
- Pollett S, Calderon M, Heitzinger K, Solari V, Montano SM, Zunt J. Prevalence and predictors of cervicitis in female sex workers in Peru: an observational study. BMC Infectious Diseases 2013;13:195. [DOI] [PMC free article] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rodriguez 2013
- Rodriguez AE. Validity of syndromic diagnostic of cervicitis and vaginal flux in reproductive age women, Bogota‐Colombia 2010 [Validez del diagnóstico sindrómico de cervicitis y flujo vaginal en mujeres en edad reproductiva, Bogotá‐Colombia 2010] [Thesis]. Bogotá: Universidad Nacional de Colombia, 2013. [Google Scholar]
Santos 2003
- Santos C, Teixeira F, Vicente A, Astolfi‐Filho S. Detection of Chlamydia trachomatis in endocervical smears of sexually active women in Manaus‐AM, Brazil, by PCR. The Brazilian Journal of Infectious Diseases : an official publication of the Brazilian Society of Infectious Diseases 2003;7(2):91‐5. [DOI] [PubMed] [Google Scholar]
Satpathy 2017
- Satpathy G, Behera HS, Ahmed NH. Chlamydial eye infections: current perspectives. Indian Journal of Ophthalmology 2017;65(2):97‐102. [PUBMED: 28345563] [DOI] [PMC free article] [PubMed] [Google Scholar]
Schachter 2008
- Schachter J, Stephens RS. Biology of Chlamydia trachomatis. In: Holmes KK, Parling PF, Stamm WE, Piot P, Wasserheit J, Corey L, et al. editor(s). Sexually Transmitted Diseases. New York: McGraw Hill, 2008:555‐74. [Google Scholar]
Schünemann 2013
- Schünemann H, Brożek J, Guyatt G, Oxman A, editors. GRADE handbook for grading quality of evidence and strength of recommendations. The GRADE Working Group, 2013 Updated October 2013.
Schünemann 2017a
- Schünemann HJ, Oxman AD, Higgins JP, Vist GE, Glasziou P, Akl E, et al. on behalf of the Cochrane GRADEing Methods Group and the Cochrane Statistical Methods Group. Chapter 11: Completing ‘Summary of findings’ tables and grading the confidence in or quality of the evidence. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Schünemann 2017b
- Schünemann HJ, Oxman AD, Vist GE, Higgins JP, Deeks JJ, Glasziou P, et al. on behalf of the Cochrane Applicability and Recommendations Methods Group. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). Cochrane, 2017. Available fromwww.training.cochrane.org/handbook.
Somani 2000
- Somani J, Bhullar VB, Workowski KA, Farshy CE, Black CM. Multiple drug‐resistant Chlamydia trachomatis associated with clinical treatment failure. Journal of Infectious Diseases 2000;181(4):1421‐7. [DOI] [PubMed] [Google Scholar]
Soto 2007
- Soto RJ, Ghee AE, Nunez CA, Mayorga R, Tapia KA, Astete SG. Sentinel surveillance of sexually transmitted infections/HIV and risk behaviors in vulnerable populations in 5 Central American countries. Journal of Acquired Immune Deficiency Syndromes 2007;46:101‐11. [PubMed] [Google Scholar]
Stamm 2008
- Stamm WE. Chlamydia trachomatis infections of the adult. In: Holmes KK, Parling PF, Stamm WE, Piot P, Wasserheit J, Corey L, et al. editor(s). Sexually Transmitted Diseases. New York: McGraw Hill, 2008:575‐93. [Google Scholar]
Sterne 2017
- Sterne JA, Egger M, Moher D, Boutron I (editors). Chapter10: Addressing reporting biases. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Tramacere 2015
- Tramacere I, Giovane C, Salanti G, D’Amico R, Filippini G. Immunomodulators and immunosuppressants for relapsing‐remitting multiple sclerosis: a network meta‐analysis. Cochrane Database of Systematic Reviews 2015, Issue 9. [DOI: 10.1002/14651858.CD011381.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
UK Guidelines 2015
- Nwokolo N, Dragovic B, Patel S, Tong W, Barker G, Radcliffe K. 2015 UK national guideline for the management of infection with Chlamydia trachomatis ‐ draft. www.bashh.org/documents/UK%20guideline%20for%20the%20management%20of%20%20Chlamydia%20trachomatis%20(8‐06‐15%20v4)%20submitted%20to%20IJSA.pdf 2015. [DOI] [PubMed]
Vishwanath 2000
- Vishwanath S, Talwar V, Prasad R, Coyaji K, Elias CJ, Zoysa I. Syndromic management of vaginal discharge among women in a reproductive health clinic in India. Sexually Transmitted Infections 2000;76(4):303‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wang 2005
- Wang SA, Papp JR, Stamm WE, Peeling RW, Martin DH, Holmes KK. Evaluation of antimicrobial resistance and treatment failures for Chlamydia trachomatis: a meeting report. Journal of Infectious Diseases 2005;191:917‐23. [DOI] [PubMed] [Google Scholar]
Weidner 2002
- Weidner W, Diemer T, Huwe P, Rainer H, Ludwig M. The role of Chlamydia trachomatis in prostatitis. International Journal of Antimicrobial Agents 2002;19(6):466‐70. [PUBMED: 12135834] [DOI] [PubMed] [Google Scholar]
WHO 2016
- World Health Organization. Guidelines for the treatment for Chlamydia trachomatis. apps.who.int/iris/bitstream/10665/246165/1/9789241549714‐eng.pdf?ua=1 2016. [WHO 2016]
Witkin 2002
- Witkin SS. Immunological aspects of genital chlamydia infections. Best Practice & Research. Clinical Obstetrics & Gynaecology 2002;16(6):865‐74. [DOI] [PubMed] [Google Scholar]
Zdrodowska‐Stefanow 2000
- Zdrodowska‐Stefanow B, Ostaszewska I, Darewicz B, Darewicz J, Badyda J, Pucilo K, et al. Role of Chlamydia trachomatis in epididymitis. Part I: Direct and serologic diagnosis. Medical Science Monitor 2000;6(6):1113‐8. [PUBMED: 11208465] [PubMed] [Google Scholar]
References to other published versions of this review
Paez‐Canro 2013
- Paez‐Canro C, Martinez‐Martinez F, Alzate JP, Lethaby A, Gaitán HG. Antibiotics for treating genital chlamydia trachomatis infection in men and non‐pregnant women. Cochrane Database of Systematic Reviews 2013, Issue 12. [DOI: 10.1002/14651858.CD010871] [DOI] [PMC free article] [PubMed] [Google Scholar]