
Figure 3 – Methods of hemostasis during excision influence visual assessment of tissue viability.
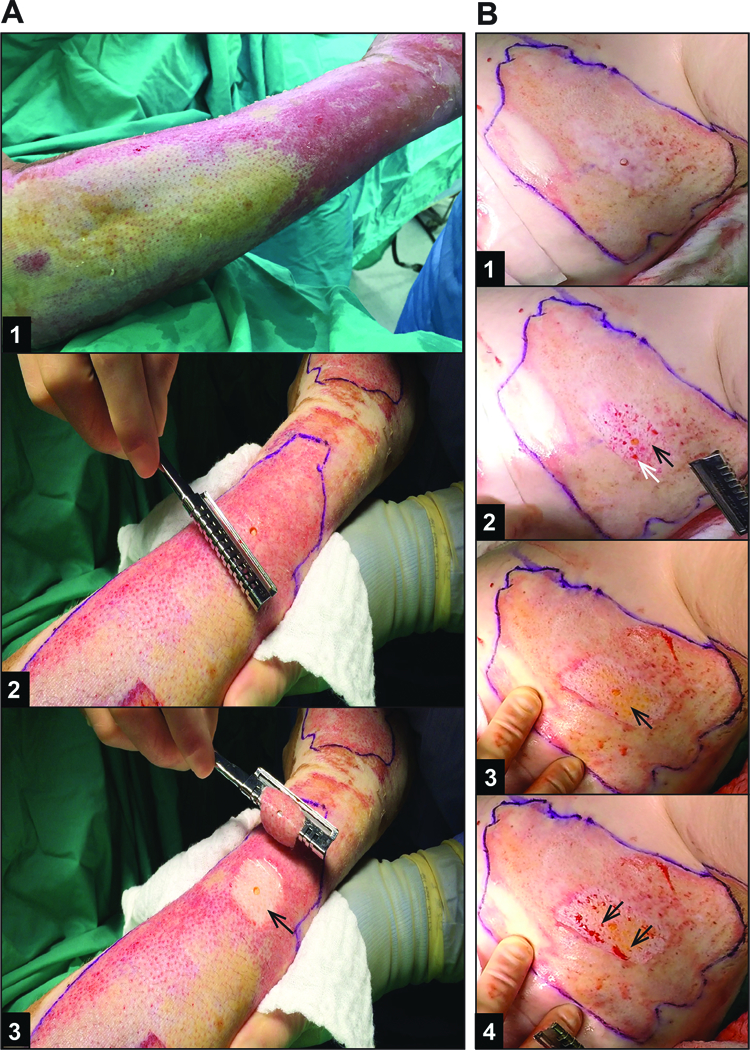
Representative patient samples of still frames from (A) an area of DPT burn excision under tourniquet and (B) FT burn excision under epinephrine tumescence without tourniquet. A1) DPT burn 10 days after injury, prior to tourniquet placement – note the heterogeneity of the burn wound with more healing having occurred in wound on the right side of the image. A2) DPT burn with biopsy after tourniquet inflated prior to excision. A3) Wound bed after 1st and only TE required to reach healthy appearing dermis (arrow). B1) FT burn 7 days after injury, after infiltration with epinephrine tumescence (flank burn). B2) Wound bed after 1st TE. Arrows indicate non-viable appearing dermis with thrombosed vessels (black arrow) and intermixed punctate bleeding (white arrow), indicating the need for further excision. B3) Wound bed after 2nd and final TE with arrow indicating healthy appearing dermis, fat, and absence of thrombosed vessels. B4) Same wound bed as in B3 after 6 seconds, showing punctate bleeding (arrows), and confirming viable, perfused wound bed.