

Abstract
We present a case of a novel PAX6 heterozygous mutation with aniridia and insulin‐dependent diabetes mellitus.To the best of our knowledge, this is the first case of its mutation with a complete loss of insulin secretory capacity. We believe that our letter will add new knowledge to diabetes mellitus associated with PAX6 mutations and might help us to understand the role of PAX6 in beta‐cell development.

PAX6 is a transcription factor involved in ocular and neural development, and PAX6 mutations result in ocular anomalies, one of which is aniridia1. PAX6 is also expressed in the pancreas, and pancreatic islet cells showed dysplasia in a PAX6 homozygous mutation mouse model1. In humans, one patient with a PAX6 heterozygous mutation presented with aniridia and early‐onset diabetes mellitus with a relatively low insulin secretory capacity2. However, most PAX6 mutations are associated with mild glucose intolerance3.
A 63‐year‐old man with diabetes was admitted to Osaka University Hospital, Suita, Japan. At the age of 12 years, he was diagnosed with aniridia. At the age of 31 years, his fasting plasma glucose and hemoglobin A1c levels were 279 mg/dL and 14.8%, respectively. He was diagnosed with diabetes, and biphasic insulin therapy was started immediately (12 U/day); intensive insulin therapy was started by the age of 40 years. On admission, his body mass index was 22.9 kg/m2. His hemoglobin A1c was 9.7%, and both fasting serum C‐peptide level and that at 6 min after an intravenous injection of 1 mg of glucagon were undetectable. The patient was negative for antibodies against glutamic acid decarboxylase, insulinoma‐associated antigen 2 and zinc transporter 8. He continued to receive basal–bolus insulin therapy and was discharged with a total daily dose of 26 units of insulin.
His eldest son also had aniridia, but was not diagnosed with diabetes until his death at the age of 26 years. His mother was diagnosed with diabetes at an older age, and she did not receive insulin therapy. His eldest daughter was diagnosed with acute‐onset type 1 diabetes at the age of 35 years, her anti‐glutamic acid decarboxylase antibody was positive and she is currently treated with continuous subcutaneous insulin infusion. She had been diagnosed with congenital glaucoma in childhood, but does not have any symptom nor sign suggesting aniridia now. The pedigree tree is shown in Figure 1.
Figure 1.
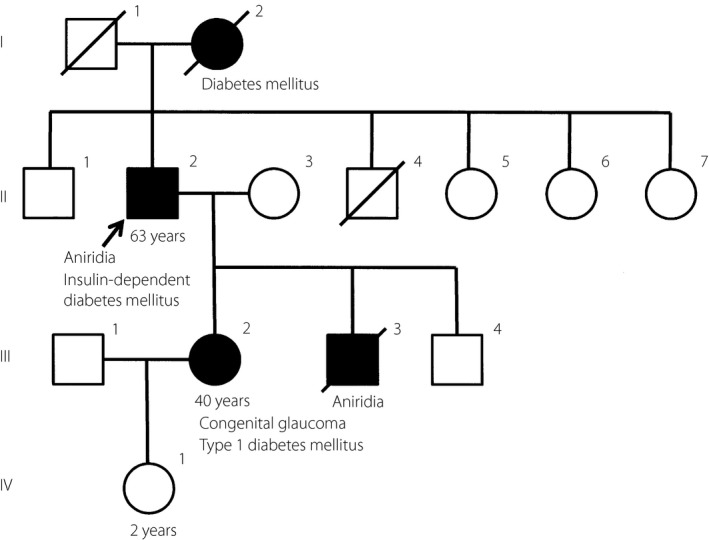
Pedigree tree of the patient. Black arrow indicates the proband. His eldest son had also aniridia and was not diagnosed with diabetes until his death at the age of 26 years. His eldest daughter was diagnosed with congenital glaucoma when she was a child and was diagnosed with autoimmune type 1 diabetes mellitus at the age of 35 years. His mother was diagnosed with diabetes mellitus at an older age.
The patient had a heterozygous 4‐bp duplication in exon 7 of the PAX6 gene (c.483_486dupTTGG); this mutation has previously been reported4. This duplication led to a frameshift and a subsequent premature stop codon in exon 8. There were no mutations in any other exons. The patient's eldest daughter did not have this mutation. These genetic analyses were carried out with the approval of the Clinical Genetics Unit in our hospital. Written informed consent was obtained after genetic counseling.
This is the first case of PAX6 mutation with aniridia and diabetes with the complete loss of insulin secretory capacity. The gradual decrease in insulin secretory capacity and negative islet autoimmunity suggests that the patient does not have typical type 1 diabetes. Considering that the function of PAX6 in the present case might be kept at half, though the messenger ribonucleic acid with premature stop codon is degraded by nonsense‐mediated messenger ribonucleic acid decay and that heterozygous PAX6 mutations usually cause mild glucose intolerance3, other genetic factors, which might have been involved in the onset of diabetes of his mother or his eldest daughter, in addition to the PAX6 mutation, might affect his insulin secretory capacity, leading to complete loss of insulin.
Disclosure
The authors declare no conflict of interest.
Acknowledgments
The authors thank Dr Kishi for informing us of the medical history of the proband's eldest daughter.
References
- 1. Sander M, Neubuser A, Kalamaras J, et al Genetic analysis reveals that PAX6 is required for normal transcription of pancreatic hormone genes and islet development. Genes Dev 1997; 11: 1662–1673. [DOI] [PubMed] [Google Scholar]
- 2. Nishi M, Sasahara M, Shono T, et al A case of novel de novo paired box gene 6 (PAX6) mutation with early‐onset diabetes mellitus and aniridia. Diabet Med 2005; 22: 641–644. [DOI] [PubMed] [Google Scholar]
- 3. Yasuda T, Kajimoto Y, Fujitani Y, et al PAX6 mutation as a genetic factor common to aniridia and glucose intolerance. Diabetes 2002; 51: 224–230. [DOI] [PubMed] [Google Scholar]
- 4. Winegarner A, Oie Y, Kawasaki S, et al Novel PAX6 mutation reported in an aniridia patient. Hum Genome Var 2017; 4: 17053. [DOI] [PMC free article] [PubMed] [Google Scholar]